Expansion in orthodontic
ByDr. Zaid Al-Dewachi
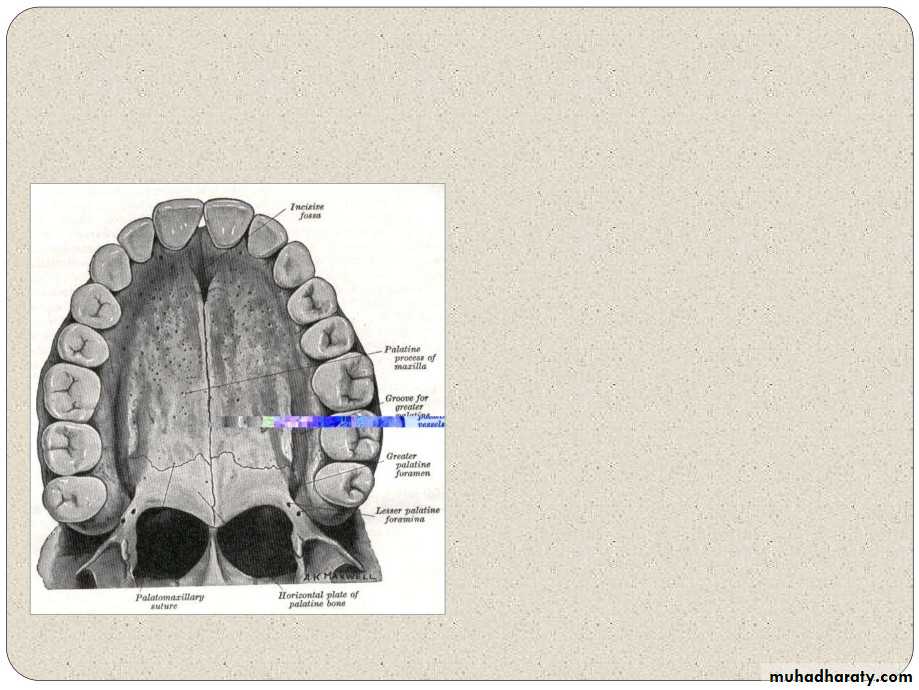
ANATOMY
Midpalatal suture isformed by the junctionof the three opposingpairs of bones namelypremaxillae, maxillaeand the palatines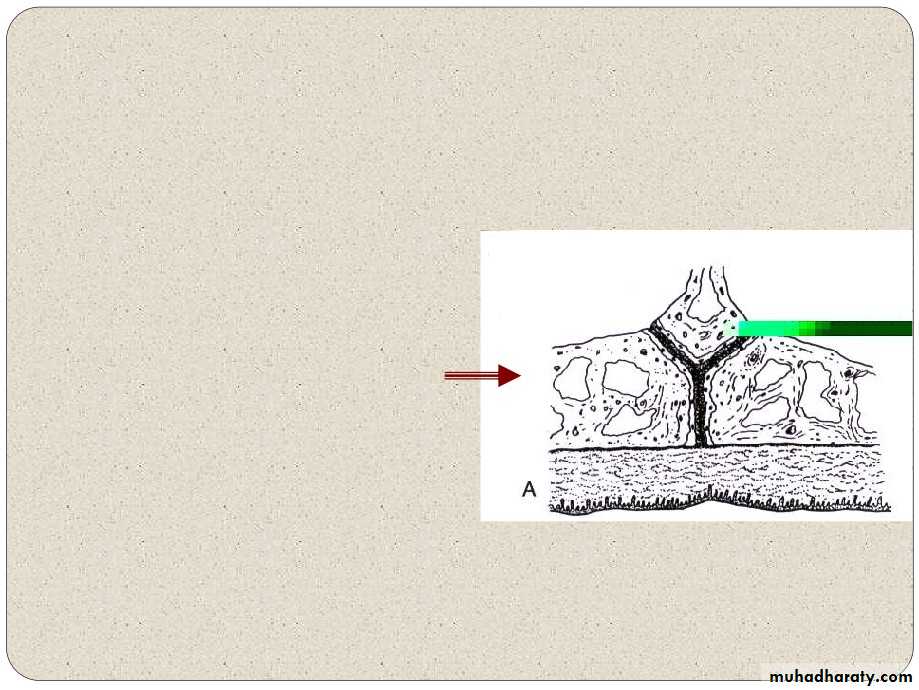
ANATOMY
The morphology of themid palatal suture hasbeen studied by MELSEN (1975).
Stages of developmentused by Bjork and Helm
First stage : Covering theinfantile
period.The
suture is very broad and Y
shaped with the vomerinebone placed in a Vshaped groove between the maxilla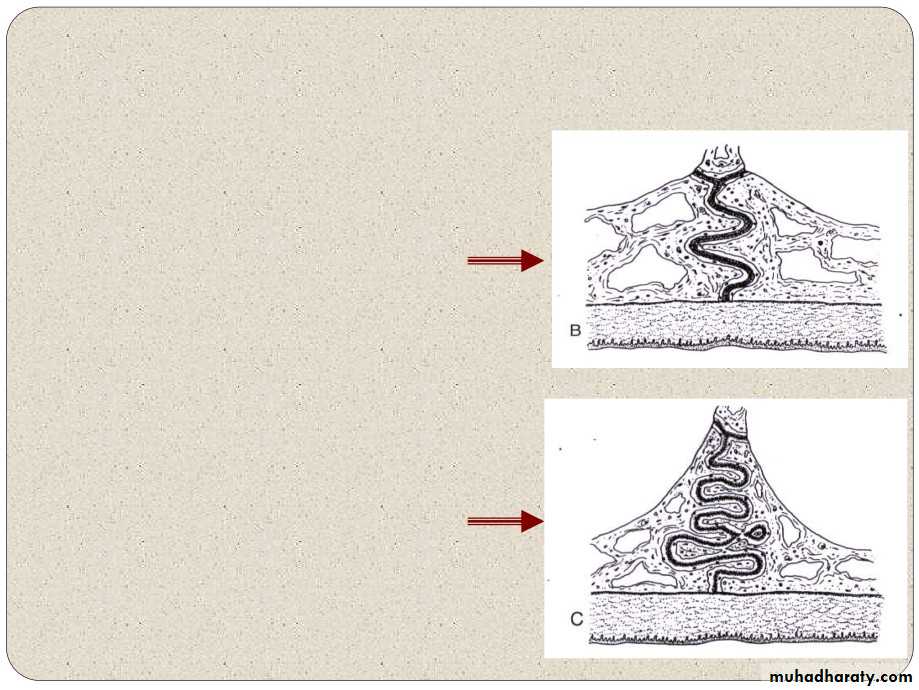
ANATOMY
Second stage :
Juvenile period, thesuture is found to bemore wavy.
Third stage :Adolescent period, the
sutureis
characterized by amore tortuous coursewith increasing inter
Etiology:
Bishara and Staley AJODO 1987 Buccolingual discrepancies could be either genetic or environmental.
Graber, Harvold, Cheirici, stated that many constricted maxillary dental arches are the result of abnormal function.
Harvold in his experimental work created narrow maxillary dental arches in rhesus monkeys by converting them from nasal to obligatory oral respiration.
All patients considered for RME should be
examined for nasal obstruction and, ifobstruction is found, they should be referred to
an otolaryngologist before orthodontic treatmenton and treatment of the problem.
RAPID EXPANSION:
1.Results in major change occurring in basalstructures of mandible and maxilla
2.Force application is more than 5 ounces.
3.Rate of separation varies from 0.2 to 0.5 mm /day4.Intermolar width - 10mm
5. Time required is 1- 4 weeks6.Skeletal changes - 50%
INDICATION OF R.M.E
(JCO 1968 Apr ;DR. JAMES)1.
In subjects, demonstrating
severe maxillary constriction:
RME is an appliance ofchoice for expansion of
maxillaryhalves
whenmaxillary
basesare
constricted.
2. Patients who have lateral
discrepancies that result ineither unilateral or bilateralposterior cross bites involving
several teeth are candidatesfor RME.
3. Patients with Class IIImalocclusions-
borderlineskeletal and pseudo Class III
problems are candidates
INDICATION Of R.M.E
4. Cleft lip and palate patients with collapsed maxillae are also RME candidates.
5. Some clinicians use this procedure to gain arch length in patients who have moderate maxillarycrowding.
6. Narrowness of the maxillary arch and nasal stenosis.7. According to Bell, the enhanced skeletalresponse that accompanies RME redirects thedeveloping posterior teeth into normal occlusion
8. RME causes a relative reduction in the nasal airway resistance by disarticulating the
maxilla from other bone particularly Septaland palatine boneCONTRA INDICATIONS FOR RME
(AJODO 1987) BISHARA AND STANLEY
1. Patients who do not cooperate with the clinician.2. Patients who have single tooth in cross bite do not need RME.
3. Patients who have anterior open bite.4. Patients with steep mandibular plane and convex profiles are generally not suited for RME.
5. Patients who have skeletal asymmetry of the maxilla or mandible.
6. Patients with severe anteroposterior and vertical skeletal discrepancies are not goodRME.
Expansion screws:
SCREWS
Skeletal expansion type, in this category wehave three types.Maximum (Maxi)Medium
Minimum (Mini) Hyrax expansion screw:
For mid palatal suture separation by means of fixedappliance without the need for acrylic plate. Metalframe work used in combination with performedband which are soldered to the retention arm.
Trapezoidal expansion screw:
This skeleton type is used mainly for narrowpalates.
This tiny screw with trapezoidal design is for 5mmexpansion.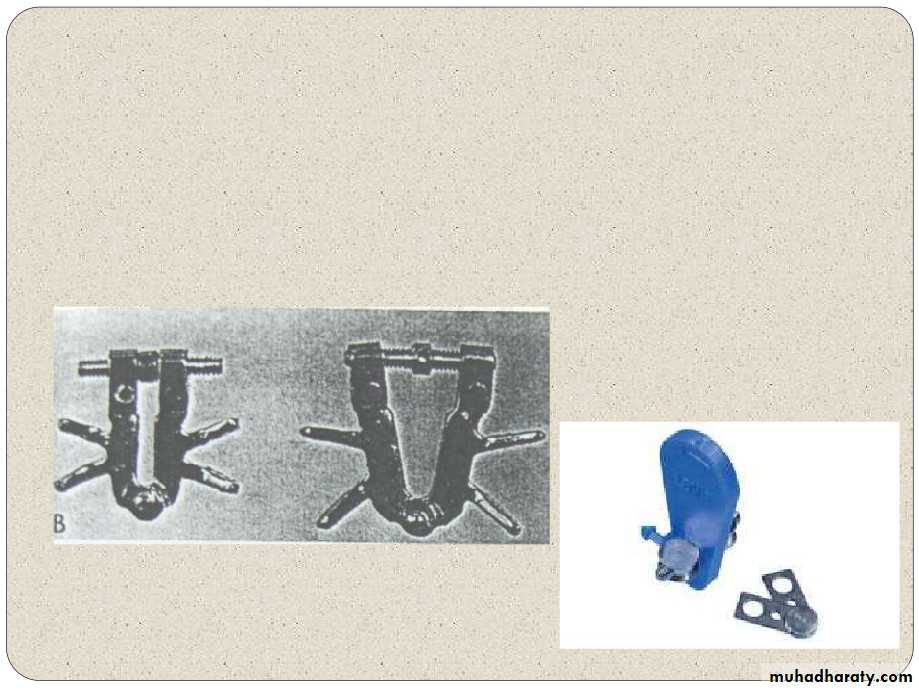
Fan type expansion screw:
For sectional expansion of maxillary anteriors. Platesections are opened up fan wise. It is designed as to stretch the arms angularly apartby progressive actions to be exerted on the samescrew.
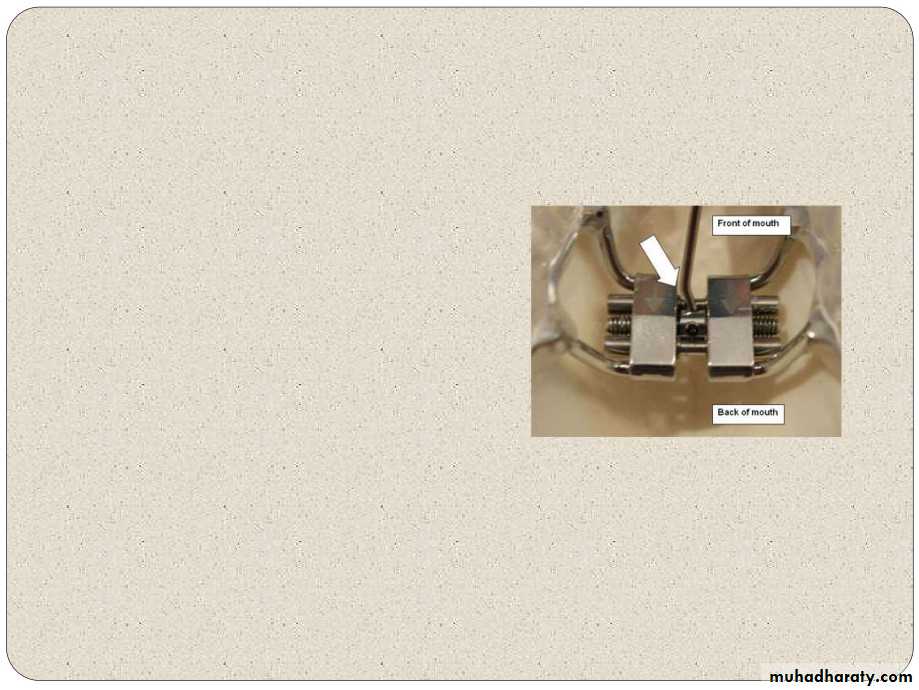
Telescopic or spring loaded screws:
Telescopic stainless steel expansion screw withrectangular guide pin for lateral expansion. Telescopic expansion screw are available inminimum - medium and maximum size.
Conventional devices used for surgically assistedrapid palatal expansion and are tooth-borne
applainces.
Some time two stage expansion screw :
Widening of the maxillary arch by palatal expansiontechnique often necessitates using, two differentexpansion screw appliance - An initial one, small enough to fit in an extremelynarrow arch and produce preliminary expansion A subsequent larger appliance with which toachieve desired arch width
Types of appliances used:
Removable appliances Fixed appliances
tooth borne
tooth and tissue borne
Tooth and tissue borne appliances include:1. Derichsweiler type
2. Haas type Tooth borne appliances include:
1. Isaacson type2. Hyrax type
www.indiandentalacademy.com
HASS TYPE EXPANDER:
AJODO 1970 March The first type of expansionscrew popularized by Haasin 1961.
It consists of bands placedon maxillary 1st premolarsand molars. A midline jackscrew is
incorporated into the acrylicpads that closely contactthe palatal mucosa.
0.045inch SS wire solderedto palatal aspect of the
HAAS TYPE EXPANDER:
Support wire extendalong the buccal and
lingual surfaces of theposterior teeth, to addrigidity to the appliance. Haas in 1961 stated thatmore bodily movementand less dental tipping isproduced when acrylicpalatal coverage is added
to support the appliance,
thus pertaining forces tobe generated not onlyagainst the teeth but alsoagainst the underlying
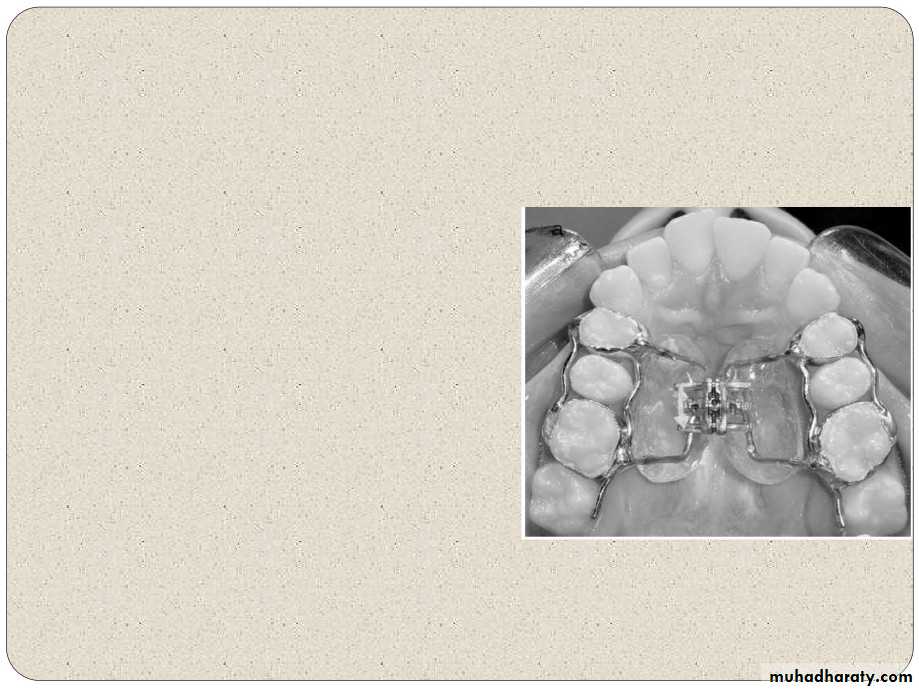
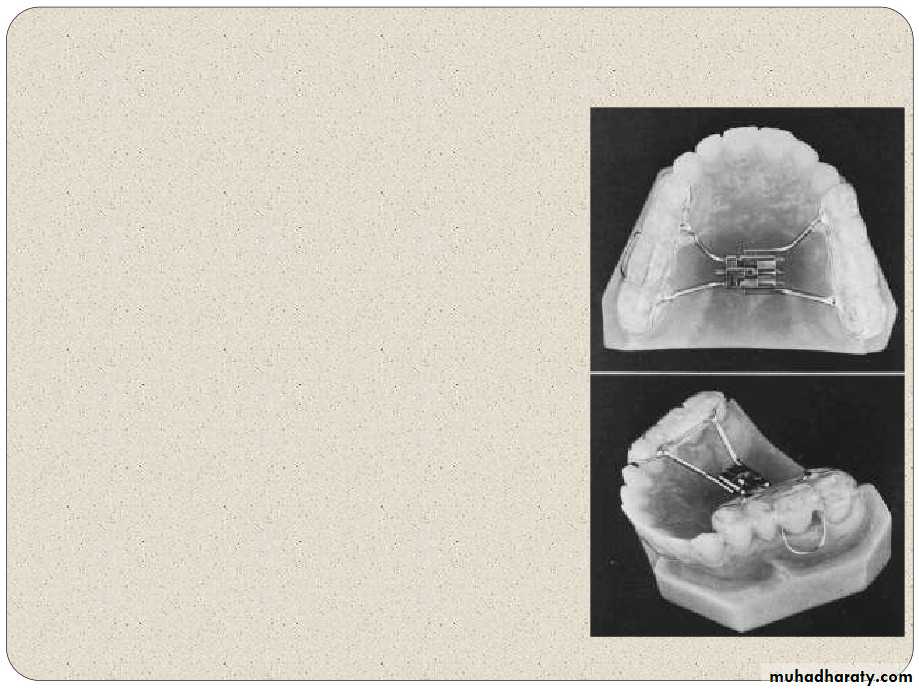
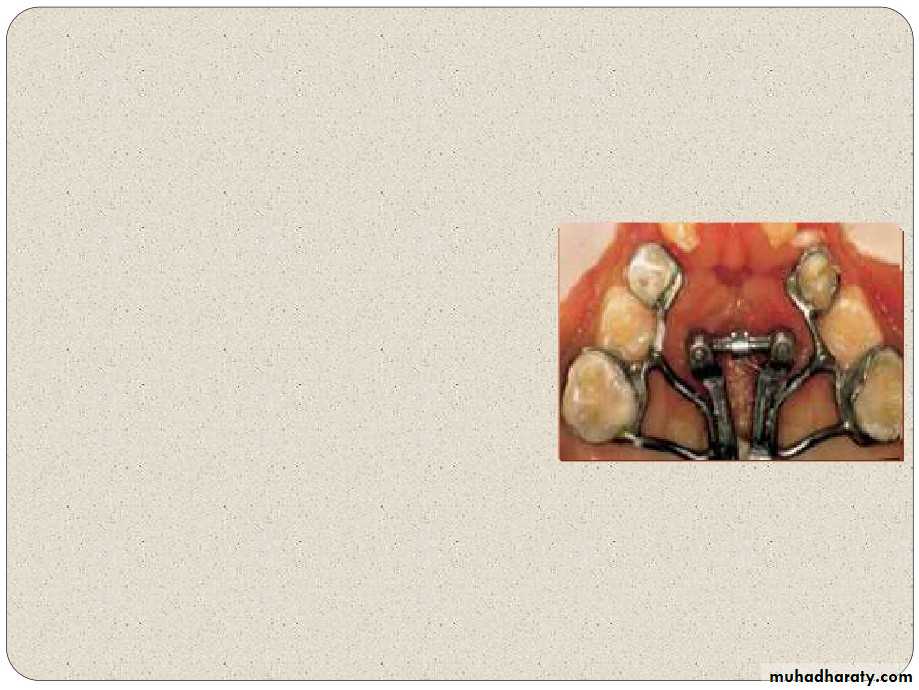
HYRAX TYPE EXPANDER:
The more commonly used type of banded RMEappliance is the hyrax type expander. It is entirely made from stainless steel.
Bands are placed on the maxillary first molarsand first premolars. The expansion screw is located in the palate inclose proximity to the palate contour.
HYRAX TYPE EXPANDER:
Buccal and lingual support wires also may beadded for rigidity. The maxilla opens as if on a hinge, with its apexat the bridge of the nose.
The suture also opens on a hinge
anterioposteriorly, seperating more anteriorly than
posteriorly.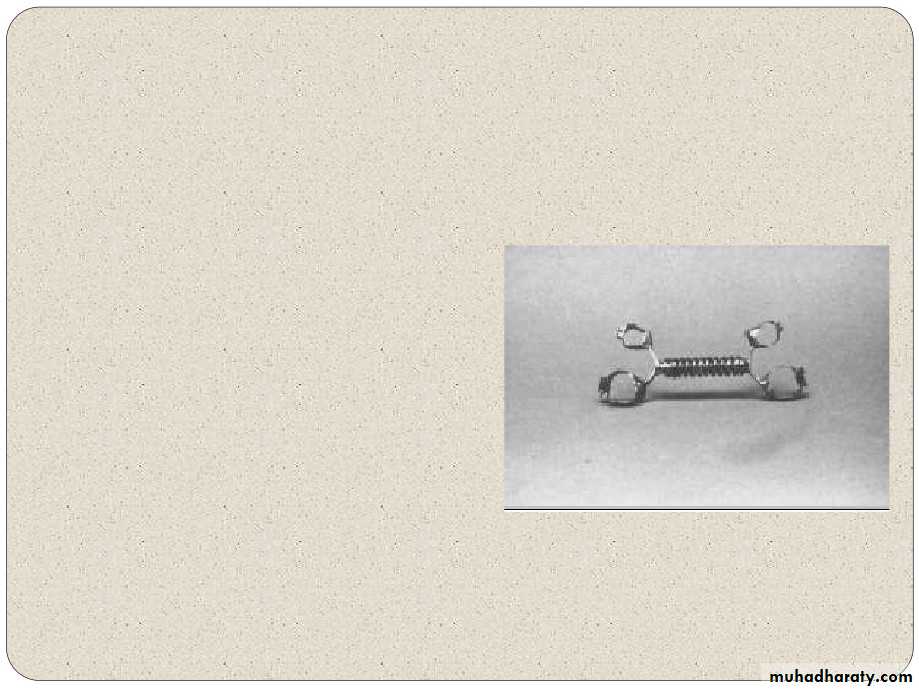
ISSACSON:
(1971) This is a tooth borneappliance with out anyacrylic palatal covering
Mini expander(developed by university of
minnesota,dental school)
soldered directly
to thebands
Screw reduced in length fornarrow arches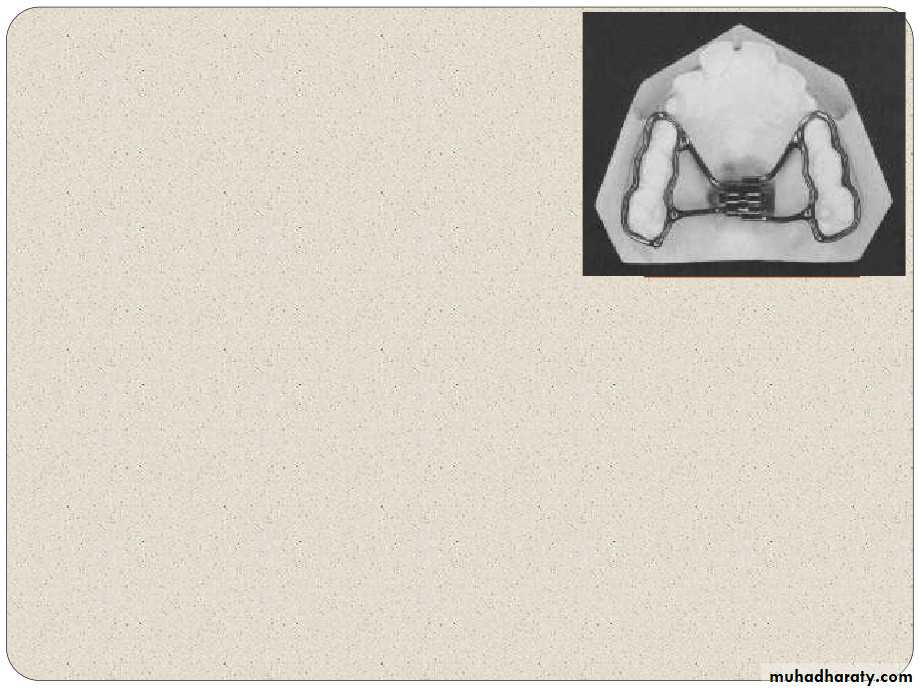
RAYMOND P HOW:
(1982)BONDED APPLIANCE.
Mid palatal Jack Screw4
rigid
0.060SS wire loops
-circumferentially at cervical level to includeposterior teeth.
Encased by collar of acrylic surrounding wireloops only. Extending from free gingivalmargin to occlusal surface. Advantage :-
Used in deciduous & severely malposedteeth Reduced food deposition as palatal acrylicremoved
David Sarver
AJODO 1989 June Bonded RME, covers overocclusal & buccal surface ofposterior teeth.
Expand & interfere free wayspace by its vertical thicknessacts as a functional appliance.
Elevatormusculature
stretched gives stretch reflexthus giving apically directed
forceon
maxillary
&mandibular teeth.
Vertical holding by intrusiveforces.
Butterfly Expander for Use in the Mixed Dentition (JCO
Oct 1999)RPE have been shown to create undesirable side effects such as dental
extrusion and tipping. A new RPE appliance, called a “butterfly expander”, that isused to treat patients in the mixed dentition was devised.
Appliance Design :
• The butterfly expander follows the basic design of Hass, with a fewmodifications.• A high midpalatal jackscrew is attached to a butterfly-shaped stainless steel
framework that extends forward to the palatal surfaces of the deciduous canines.• The appliance is soldered to bands on the second deciduous molars.
• A high -powered laser is used to weld the two arms to the screw housing,ensuring perfect, one-piece joints and eliminating any possibility of detachment.
• The rigidity of the appliance and its location high in the palatal vault allow thetransverse force to be delivered closer to the center of resistance of the posteriorteeth than with conventional expander.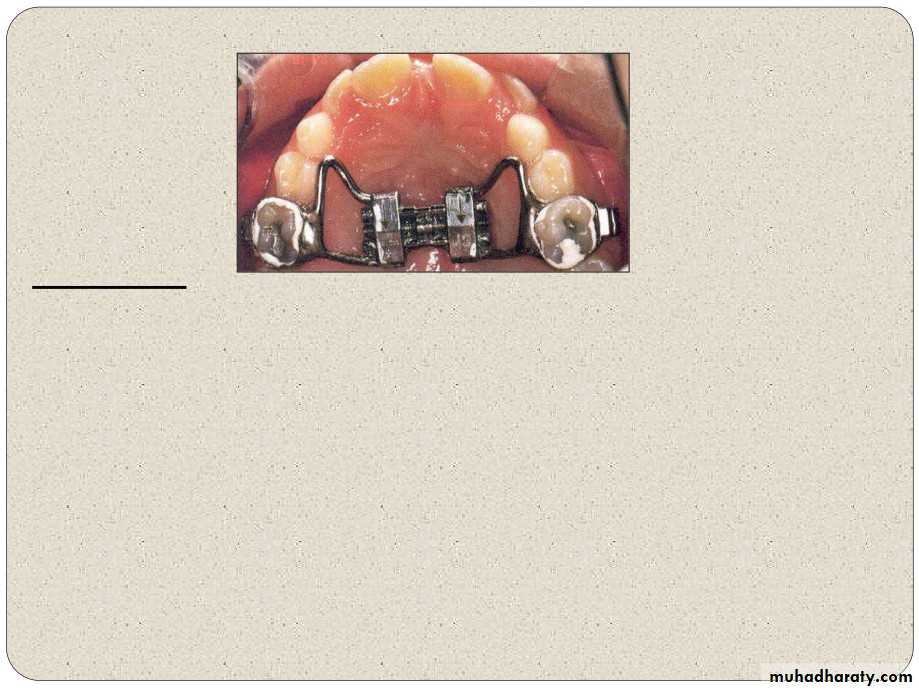
• The butterfly design thus minimizes posterior tipping and extrusion.
Activation :
• Activation of the screw is begun with a complete turn (four quarter -turns)immediately after cementation of the appliance.• The parents should be instructed to activate the screw a quarter-turn three, timesa day (morning, afternoon, and evening).
• Active expansion takes seven to nine days, depending on the degree of maxillaryconstriction.
• Transverse expansion is usually deemed sufficient when the posterior crossbite is
over corrected by 2-3 mm.• Screw is then blocked, and the appliance is left in place as a passive retainer.
•
A Fan-Shaped Maxillary Expander
LUCA LEVRINI JCO NOVEMBER 1999
The expander is made of stainless steel, with the spider screw as the activecomponent.
There are three pivot points: a posterior one - “fan” opening
two anterior ones- counteract the
torquingforces
produced duringexpansion.
Four arms, two mesial and two distal, are welded to the expander and to bands on the teeth.
Dental arch and arch perimeter
changesSME - Minne Expander
Results:(By Lorenzon & Ucem EJO 1998)
RME - HYRAX1.
2.
3.
Increase in upper intercanine width greater in RME group than
in SME.Regression analysis indicated maxillary arch perimeter gain :-arch perimeter gain = 0.65 times of posterior expansion inRME & 0.60 times in SME group.
prediction equation shows maxillary arch perimeter gain
:- 0.54 times at premolar width in RME & 0.52 in SME
How Much To Expand
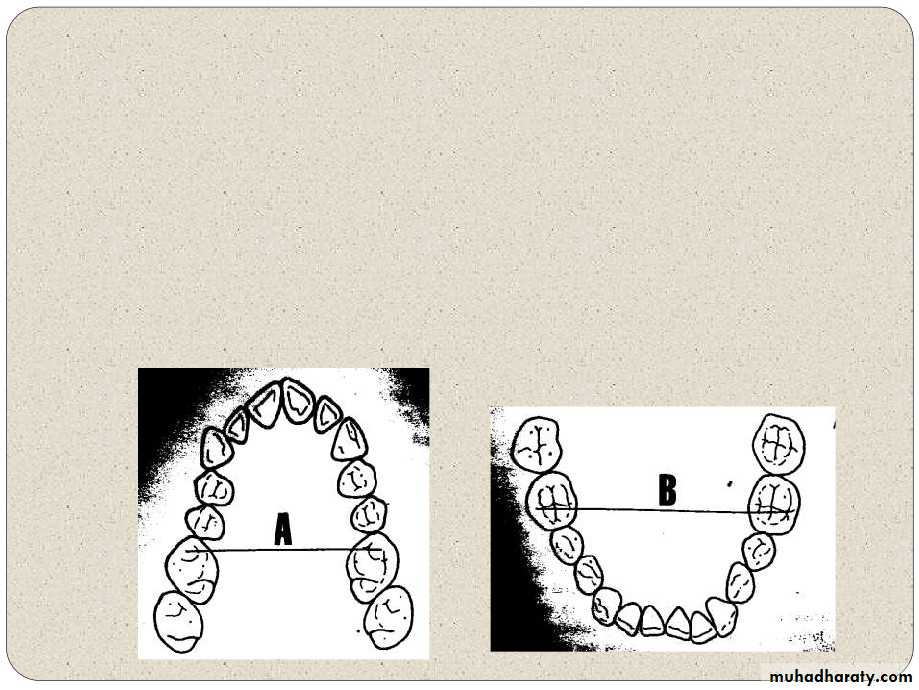
Measure the distance between the tips of themesiobuccal cusps of the maxillary 1st molars.
Subtract the mandibular measurment from themaxillary measurement
The average differences in persons withnormal occlusion are1.6mm for males and1.2mm for females
Rapid expansion should not be done in youngchildren as there is a risk of distortion of facialstructures with rapid expansion and there is no
evidence that rapid movement and higher forces
produce better and more stable expansion.Effects of RME:
EFFECT OF R.M.E. ON THE MAXILLARYAND MANDIBULAR COMPLEX
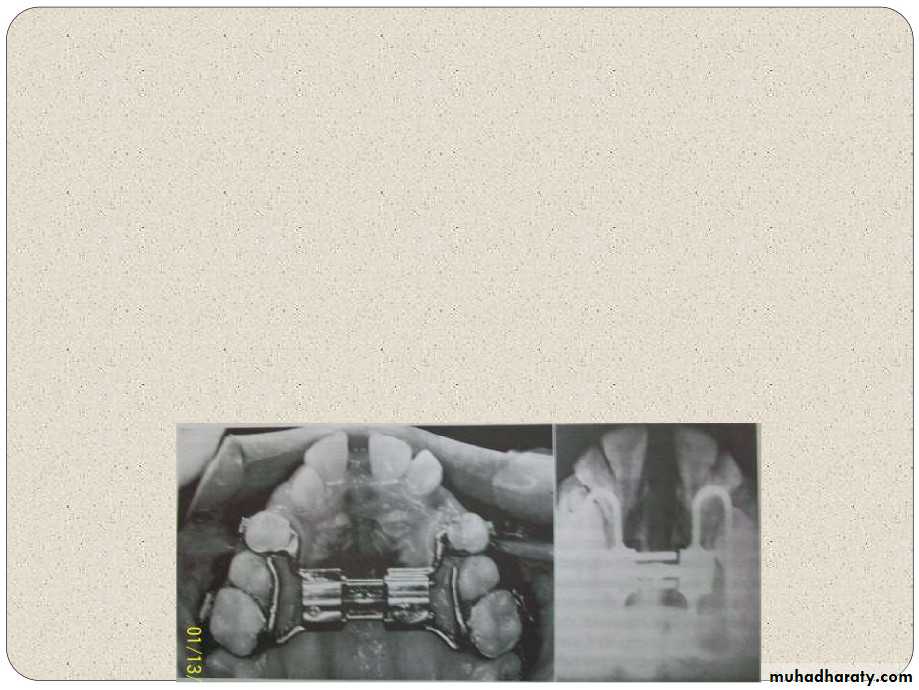
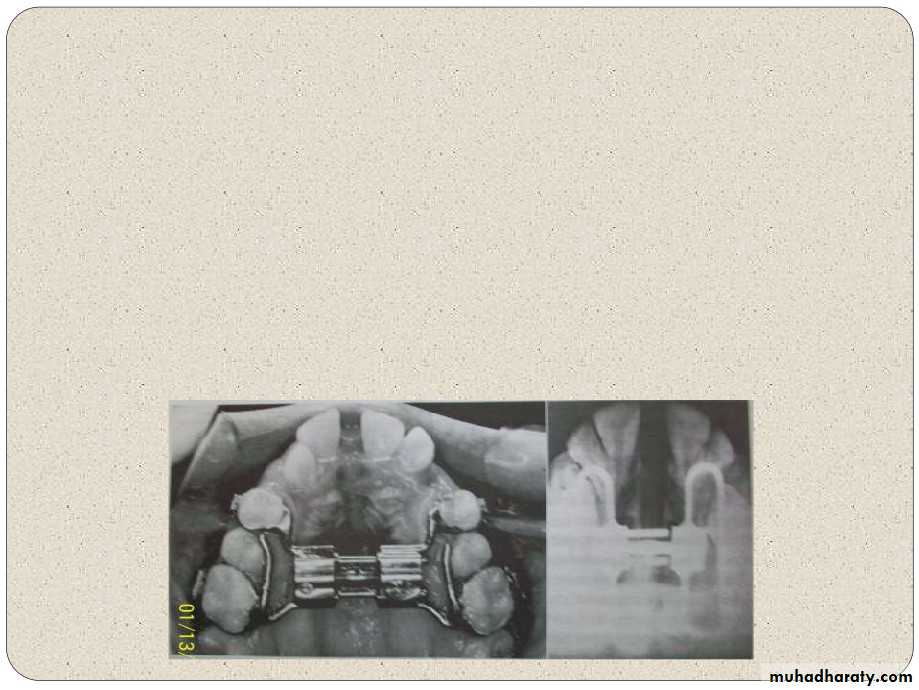
(AJODO 1987 BISHARA AND STANLEY) Rapid maxillary expansion occurs when theforce applied to the teeth and the maxillaryalveolar processes exceeds the limits needed
for orthodontic tooth movement.
The applied pressure acts as an orthopedicforce that opens the midpalatal suture.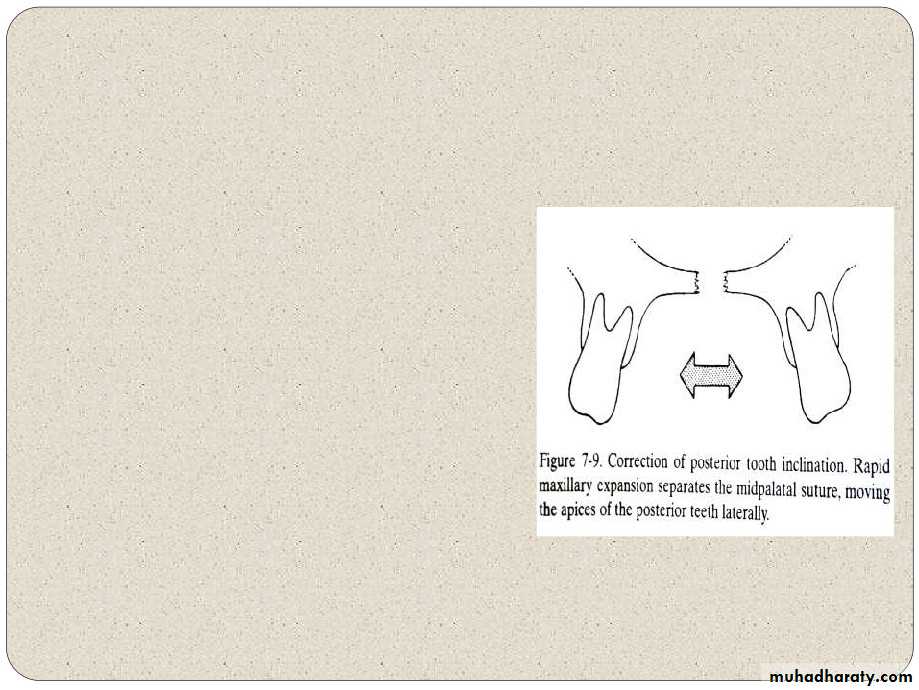
The
compressesperiodontal
bends theprocesses,
appliance
theligament,
alveolartips the
anchorteeth,
andgradually
opens themidpalatal suture.
Relation between amount of
sutural separation and extent ofmolar expansion
the amount of sutural opening was equal to or less than one half the amount of dental arch expansion. Changes during fixation and retention. Krebsnoted that although dental arch width was
maintained during fixed retention, the distancebetween implants in the infrazygomatic ridgesdecreased during the3months of fixedretention by an average of 10% to 15%.
This relapse continued during retention withremovable appliances. After an averageperiod of 15 months, approximately 70% of
the infrazygomatic maxillary width increase
was maintained
SLOW EXPANSION DEVICES
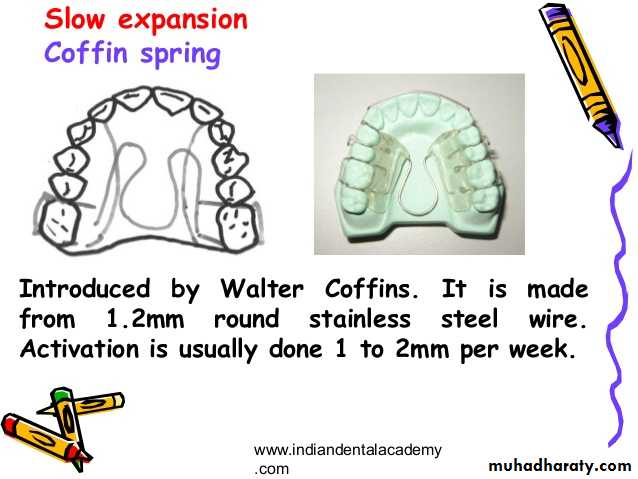
Coffin spring:Designed by Walter Coffin
Removable applianceDento-alveolar expansion
Made up of 1.25mm thick omega shaped wire placed in mid palatal region
Free ends of omega embedded in acrylic
Activated 1 to 2 mm per week
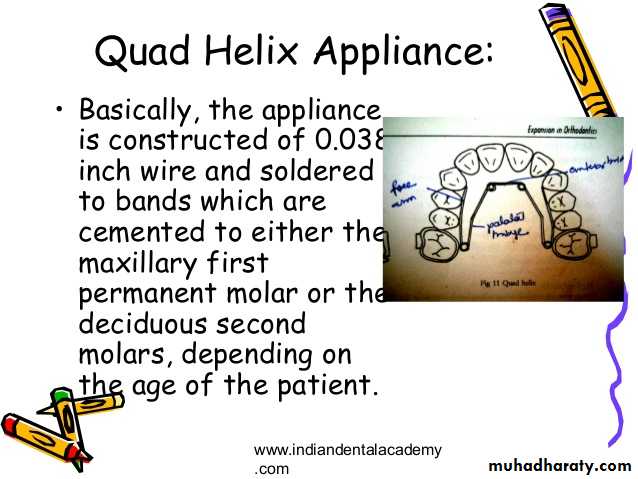
Quad helix:
Described by Ricketts
Constructed using a 0.038 inch wire
Incorporates 4 helices, therefore flexibility and range of application is more
• Differences between slow expansion and RME
3. Effects on tissues mild• Dental
Skeletal mainly & Dental effects
Relapse tendency
Results more
Duration of Treatment
• Stable
• 2-4 months
• One month
• 6. Arch Perimeter changes Lesser
• Significantly greater
• Inter- canine width
• Mandibular rotation
• 0.60 times
• the posterior expansion
• nil
0.65 times the posterior expansion
Downward & backward
• 1-SN angle
• Properties
• Slow Expsn
• RME
• 1. Bio Mechanical
• Orthodontic Effect
• Orthopaedic Effect
• Effect
• 2. Type & Amount of
• Light force
• Heavy force
• force applied
• (400-500gms)
• (2000-5000gms)
• 9. ANB
• Lesser than RME
• Significant increase
• 10.decrease in
• nil
• Significant
• 11. N-Pg-A
• not significant• Significant
• change