PHASE I PERIODONTAL THERAPY
The major goal of phase I therapy is to control the factors responsible for the periodontal inflammation; the removal of subgingival bacterial deposits and the subsequent control of plaque levels by patients are particularly significant.Phase I therapy should be comprehensive and include scaling, root planing, and oral hygiene instruction, as well as other therapies such as caries control, replacement of defective restorations, occlusal therapy, orthodontic movement, and smoking cessation.
Comprehensive reevaluation after phase I therapy is essential to validate treatment options and to estimate prognosis. Many patients can have their periodontal disease controlled with phase I therapy and not require further surgical intervention. In patients who do need surgical treatment, phase I therapy is advantageous in that it also provides tissue with reduced inflammatory infiltration, thus improving the surgical management of the tissue and improving the healing response.
For patients with 5 mm or more of attachment loss and with pockets present after phase I treatment, surgical treatment should be planned. Advanced cases may be best treated by periodontal specialists.
To alter or eliminate the microbial etiology and factors that contribute to gingival and periodontal diseases to the greatest extent possible, therefore stopping the progression of disease and returning the dentition to a state of health and comfort.
OBJECTIVE
Phase I procedures are a required part of periodontal therapy, regardless of the extent of disease present. In many cases, phase I therapy will be the only set of procedures required to restore periodontal health, or they will constitute the preparatory phase for surgical therapy.
RATIONALE
Phase I therapy is a critical aspect of periodontal treatment. The long-term success of periodontal treatment depends predominantly on maintaining the results achieved with phase I therapy and much less on any specific surgical procedures.
In addition, phase I therapy provides an opportunity for the dentist to evaluate tissue response and patient motivation about periodontal care, both of which are crucial elements to the overall success of treatment.
Good oral hygiene is most easily accomplished if the tooth surfaces are free of calculus deposits and other irregularities so that surfaces are easily accessible. Therefore, in addition to teaching periodontal patients adequate home plaque control procedures, management of contributing local factors includes the following therapies, as required:
1. Complete removal of calculus
2. Correction or replacement of poorly fitting restorations and prosthetic devices
3. Restoration or temporization of carious lesions
4. Orthodontic tooth movement
5. Treatment of food impaction areas
6. Treatment of occlusal trauma
7. Extraction of hopeless teeth
8. Possible use of antimicrobial agents including necessary plaque sampling and sensitivity testing
TREATMENT SESSIONS
After careful analysis and diagnosis of the specific periodontal condition present, the dentist must develop a treatment plan that includes all required procedures and estimates the number of appointments necessary to complete phase I therapy.In most cases, patients require several treatment sessions for the complete debridement of tooth surfaces. Sometimes carious lesions and other contributing factors have to be controlled before an accurate estimate can be made.
All of the following conditions must be considered when determining and developing the phase I treatment plan:
• General health and tolerance of treatment
• Number of teeth present• Amount of subgingival calculus
• Probing pocket depths and attachment loss
• Furcation involvements
• Alignment of teeth
• Margins of restorations
• Developmental anomalies
• Physical barriers to access (i.e., limited opening or tendency to gag)
• Patient cooperation and sensitivity (requiring use of anesthesia or analgesia)
SEQUENCE OF PROCEDURES
Step 1: Plaque Control Instruction.
Plaque control is the essential component to successful periodontal therapy, and instruction should begin in the first treatment appointment.The patient must learn to correctly brush the teeth, focusing on applying the bristles at the gingival third of the clinical crowns of the teeth, and begin using floss or other aids for interdental cleaning. This is sometimes referred to as “targeted oral hygiene” and emphasizes thorough plaque removal around the periodontal tissues.
The multiple appointment approach to phase I therapy permits the dentist to evaluate, reinforce, and improve the patient’s oral hygiene skills.
Step 2. Removal of Supragingival and Subgingival Calculus.
Removal of calculus is accomplished using scalers, curettes, ultrasonic instrumentation, or combinations of these devices during one or more appointments.Evidence suggests that the treatment results for chronic periodontitis are similar for all instruments, and some dentists now incorporate laser technology into periodontal therapy, including phase I therapy
Step 3. Recontouring Defective Restorations and Crowns.
Corrections for restorative defects, which are plaque traps, may be made by smoothing surfaces and overhangs with burs or hand instruments or by replacing restorations. These procedures can be completed concurrently with other phase I procedures.Step 4. Management of Carious Lesions.
Removal of the carious tissue and placement with either temporary or permanent restorations is indicated in phase I therapy because of the infectious nature of the caries process. Healing of the periodontal tissues will be maximized by removing the reservoir of bacteria in these lesions so that they cannot repopulate the microbial plaque.


Effects of overhanging amalgam margin on interproximal gingiva of maxillary first molar in otherwise healthy mouth. Bleeding elicited by gentle probing of interproximal pocket indicating severe inflammation.
Step 5. Tissue Reevaluation.
After scaling, root planing, and other phase I procedures, the periodontal tissues require approximately 4 weeks to heal sufficiently to be probed accurately.Patients also need the opportunity to improve their plaque control skills to both reduce inflammation and adopt new habits.
At the reevaluation appointment, periodontal tissues are probed, and all related anatomic conditions are carefully evaluated to determine if further treatment, including periodontal surgery, is indicated.
Additional improvement from periodontal surgical procedures can be expected only if phase I therapy resulted in the gingiva being free of overt inflammation and the patient has learned effective daily plaque control.
RESULTS
Studies indicated that scaling and root planing therapy is both effective and reliable. Up to 80% reduction in bleeding on probing and mean probing depth reductions of 2 to 3 mm could be achieved. The percentage of periodontal pockets of 4-mm or greater depth could be reduced more than 50% and up to 80%.Recent studies suggested both the one appointment and staged or multiple appointment treatment strategies work well, regarding clinical parameters of healing and microbial parameters.
Staged therapy permits the advantage of evaluating and reinforcing oral hygiene care, and the one or two appointment therapies can be more efficient in reducing the number of office visits the patient is required to attend.


Severe chronic periodontitis. A 45-year-old patient with deep probe depths, bone loss, severe swelling, and redness of the gingival tissues.
3 weeks after the finishing phase I therapy. Note the gingival tissue has returned to a normal contour; redness and swelling dramatically reduced.

moderate chronic periodontitis. A 52-year-old patient with moderate attachment loss and 4-6 mm probe depths. Lingual view shows visible inflammation and heavy calculus deposits
18 months after phase I therapy the same area shows significant improvement in gingival health.
HEALING
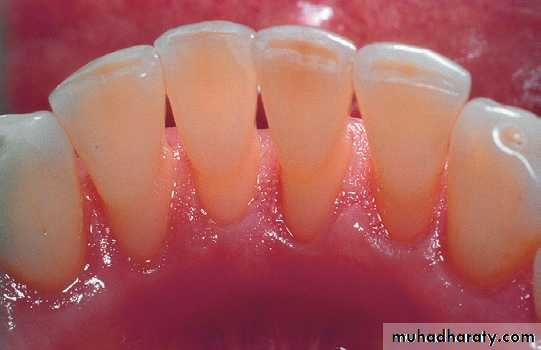
Healing of the gingival epithelium consists of the formation of a long junctional epithelium rather than new connective tissue attachment to the root surfaces. The attachment epithelium reappears 1 to 2 weeks after therapy.Gradual reductions in inflammatory cell population, crevicular fluid flow, and repair of connective tissue result in decreased clinical signs of inflammation, including less redness and swelling. One or two millimeters of recession is often apparent as the result of tissue shrinkage.
Transient root sensitivity frequently accompanies the healing
process. This development is common and can be disconcerting to patients. The extent of the sensitivity can be diminished through good plaque removal. Warning patients about these potential outcomes, the teeth appearing longer because of shrinkage of periodontal tissues and tooth root sensitivity, at the beginning of the treatment sequence will avoid surprise if these changes occur. Unexpected and possibly uncomfortable consequences to treatment may result in distrust and loss of motivation to continue therapy.
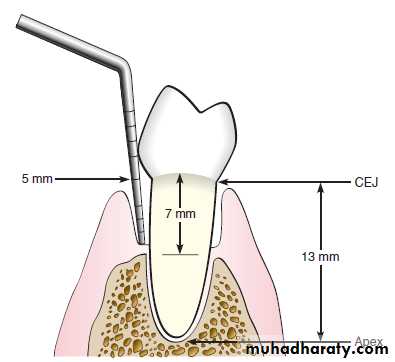
The 5-mm standard has been commonly used as a guideline for identifying candidates for referral and relates to the presence of 5 mm or more of clinical attachment loss present at the reevaluation appointment.
In terms of probing depths, the treatment of periodontal diseases is generally successful in patients with 6- to 8-mm probe depths. Success rates diminish when probing depths are 9 mm or greater, so early referral of advanced cases is likely to provide the best results.
To be continued…