CLEANSING AND POLISHING INSTRUMENTS
Rubber Cups. Rubber cups consist of a rubber shell with or without webbed configurations in the hollow interior. The handpiece and rubber cup must be sterilized after each patient use, or a rubber cup may be used and then discarded.A good cleansing and polishing paste that contains fluoride should be used and kept moist to minimize frictional heat as the cup revolves. Polishing pastes are available in fine, medium, or coarse grits and are packaged in small, convenient, single-use containers.
Aggressive use of the rubber cup with any abrasive may remove the layer of cementum, which is thin in the cervical area.
Bristle Brushes. Bristle brushes are available in wheel and cup shapes. The brush is used in the with a polishing paste. Because the bristles are stiff, use of the brush should be confined to the crown to avoid injuring the cementum and the gingiva.

SONIC AND ULTRASONIC INSTRUMENTATION AND IRRIGATION
Sonic and ultrasonic instruments are as effective as hand instruments used for root planing. They offer advantages in that they are efficient and the new smaller tips have better access to hard-to-reach subgingival areas such as narrow furcations and root concavities. Some of the older implanted cardiac pacemakers could be inhibited by magnetostrictive ultrasonic instruments, thus these instruments should not be used for these patients.Sonic and ultrasonic instruments are primarily used during initial therapy, but they also are valuable during periodontal surgery to remove residual calculus from previously inaccessible locations such as furcations, grooves concavities, and distal surfaces of posterior teeth.
Powered irrigation oral hygiene devices may add to the effectiveness of the patient’s other oral hygiene procedures when used with water or with antimicrobial solutions such as chlorhexidine.
Pulsed jets are more effective than constant stream devices and can give reductions in gingivitis, bleeding on probing, and periodontal pathogenic bacteria similar to that seen with flossing. These devices are particularly useful in patients with fixed orthodontic appliances, complex prosthetic treatment, and intermaxillary fixation, as well as in patients noncompliant with floss.


MECHANISM OF ACTION OF POWER SCALERS
Various physical factors play a role in the mechanism of action of power scalers. These factors include frequency, stroke, and water flow. In addition to rate of flow, the physiologic effects of water may play a contributing role in the efficacy of power instruments.Water contributes to three physiologic effects that play a role
in the efficacy. These are acoustic streaming, acoustic turbulence, and cavitation.
.
)) Acoustic steaming is the unidirectional fluid flow caused by ultrasound waves.
)) Acoustic turbulence is created when the movement of the tip causes the coolant to accelerate, producing an intensified swirling effect. This turbulence continues until cavitation occurs.
)) Cavitation is the formation of bubbles in water caused by the high turbulence. The bubbles implode and produce shock waves in the liquid, creating further shock waves throughout the water. The combination of acoustic streaming, acoustic turbulence, and cavitation has been shown to disrupt microflora
TYPES OF POWER INSTRUMENTS
1)) Sonic units work at a frequency of 2000 to 6500 cycles per second and use a high or low speed air source from the dental unit. Water is delivered via the same tubing used to deliver water to a dental handpiece. Sonic scaler tips are large in diameter and universal in design.2)) Magnetostrictive ultrasonic devices work in a frequency range of 18,000 to 50,000 cycles per second. Metal stacks that change dimension when electrical energy is applied power magnetostrictive technology. Vibrations travel from the metal stack to a connecting body that causes the vibration of the working tip. Tips move in an elliptical or orbital stroke pattern. This allows the tip four active working surfaces.

3)) Piezoelectric ultrasonic units work in a frequency range of 18,000 to 50,000 cycles per second. They have ceramic discs that are located in the handpiece power piezoelectric technology. They change in dimension as electrical energy is applied to the tip. Piezoelectric tips move in a linear pattern, giving the tip two active surfaces. A variety of insert tip designs and shapes are available for use
Tip Designs
There are tips designed to remove heavy supragingival calculus or to definitively debride periodontal pockets. Large diameter tips are created in a universal design and are indicated for the removal of large, tenacious deposits. A high power setting is generally recommended.
Thinner diameter tips may be site specific in design. The straight tip design is ideal for use in treating patients with gingivitis and deplaquing maintenance patients. The right and left contra-angled instruments allow for greater access and adaptation to root morphology. These inserts are designed to work in a low power setting.

EFFICIENCY AND CLINICAL OUTCOMES
Power instrumentation has the potential to make scaling less demanding, more time efficient, and more ergonomically friendly.Modified tip designs allow for improved access in many areas, including furcations. Newer, slimmer designs operate effectively at lower power settings, thus improving patient comfort. Sonic and ultrasonic tips can reduce the time needed for scaling.
No differences were found in the efficacy of subgingival debridement between sonic, magnetostrictive, and piezoelectric scalers versus hand instruments in the treatment of chronic periodontitis.
With the advent of new designs and thinner tips, deplaquing of root surfaces may be effectively accomplished by power-scalers.
Both sonic and ultrasonic instruments have been shown to be effective in removing calculus similar to hand instrumentation. Ultrasonic instruments through high-speed action produce a cavitational activity and acoustic microstreaming that some believe may help enhance the disruption of the bacteria in subgingival biofilms.
In comparing power scalers to hand instruments, both types demonstrate similar outcomes for reductions in bleeding on probing and probing depth and gains in clinical attachment.
SPECIAL CONSIDERATIONS
Furcations present one of the greatest scaling challenges. In many instances, the opening of the furcation is narrower than the conventional hand instrument. For this reason, power scalers may be recommended as a means to improve access when scaling furcations.Aerosol Production
Universal infection control procedures can help minimize the amount of aerosol produced. Three levels of defense in the reduction of dental aerosols are recommended.
1)) Personal protective barriers such as a mask, gloves, and safety glasses.
2)) Routine use of an antiseptic preprocedural rinse.
3)) The use of a high-speed evacuation device either by a dental assistant or attached to the instrument being used.
In all cases and with all patients, the guidelines for infection control should be adhered to.
Cardiac Pacemakers
In patients with cardiac pacemakers, atrial and ventricular pacing was found to be inhibited by electromagnetic interference produced by a magnetostrictive ultrasonic scaler. A sonic scaler was also tested but did not produce the same effect. So, as a precaution, it is advocated using only hand instruments on individuals with pacemakers.
PRINCIPLES OF INSTRUMENTATION
Ultrasonic technique is not different from instrumentation with hand scalers. A modified pen grasp is used with an ultrasonic scaler along with an extraoral fulcrum. The purpose of the extraoral fulcrum is that it allows the operator to maintain a light grasp and easier access physically and visually to the oral cavity. Alternate fulcrums of cross arch or opposite arch fulcrums are acceptable alternatives.
Modified pen grasp with tip.
Light pressure is needed with a power instrument. The tip is traveling at a set frequency in a set stroke pattern. Increased clinician pressure on the tip causes decreased clinical efficacy.Sonic/ultrasonic instrumentation requires removal from the coronal to the apical portion of the deposit. This stroke pattern allows the insert to work at its optimal stroke pattern and frequency for quick effective deposit removal. A deplaquing stroke should be used when the focus is removal of biofilm and soft debris for the resolution of gingival inflammation. This stroke entails accessing every square millimeter of the tooth surface during ultrasonic deplaquing as a result of the limited lateral dispersion of the lavage subgingivally
ORAL IRRIGATION (WATER JET)
The body of evidence on the dental water jet consistently has been shown to significantly reduce gingivitis, bleeding on probing, and periodontal pathogens. These oral health improvements have been demonstrated with the use of either water or an antimicrobial agent.Emerging evidence indicates the dental water jet effectively removes biofilm and is as effective as dental floss when added to toothbrushing.
The mechanism of action of irrigation occurs through the direct application of a pulsed stream of water or other solution. Studies have found pulsation and pressure to be critical components of an irrigation device.
Dental water jets with varying pulsation and pressure are available.

MECHANISM OF ACTION OF IRRIGATION
A pulsation rate of 1200 per minute has been shown to create
two zones of hydrokinetic activity: the impact zone, in which the solution initially contacts, and the flushing zone, in which the solution reaches into the subgingival sulcus. The outcome of hydrokinetic activity is subgingival penetration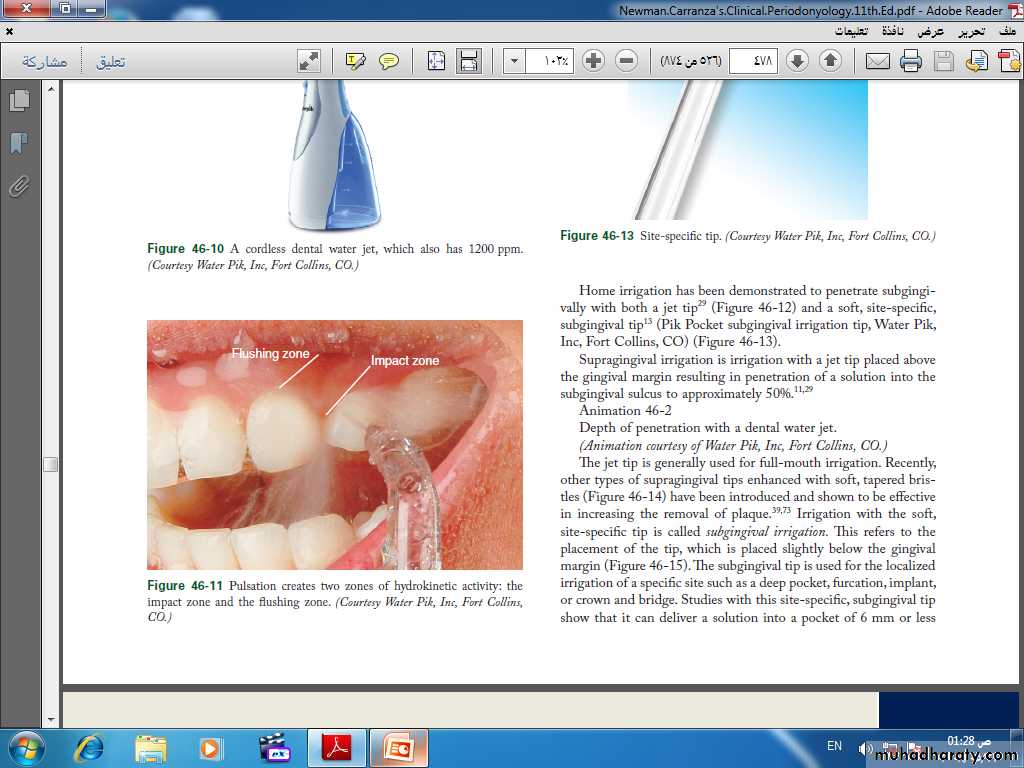
Supragingival irrigation is irrigation with a jet tip placed above the gingival margin resulting in penetration of a solution into the subgingival sulcus to approximately 50%.
Recently, other types of supragingival tips enhanced with soft, tapered bristles have been introduced and shown to be effective in increasing the removal of plaque. Irrigation with the soft, site-specific tip is called subgingival irrigation. This refers to the placement of the tip, which is placed slightly below the gingival margin


The Pik Pocket tip is gently placed slightly subgingivally
CLINICAL OUTCOMES OF IRRIGATIONHome irrigation has been studied and found safe and effective for those with gingivitis,† implants, crown and bridge, orthodontics, intermaxillary fixation, and diabetes; patients who are noncompliant with dental floss; and in periodontal maintenance.
Oral irrigation with water added to toothbrushing reduced gingivitis by 52% compared to a 30% reduction for toothbrushing alone. Throughout the years, other researchers have found concurring results with the use of plain water. The use of an antimicrobial agent, such as diluted chlorhexidine or an essential oil, generally enhances reductions in gingivitis and bleeding.