Cardiology Lectures Dr. Ahmed Moyed Hussein
Mitral stenosis (MS)Aetiology and pathophysiology
Mitral stenosis is almost always rheumatic in origin, although in older people it can be caused by heavy calcification of the mitral valve apparatus. There is also a rare form of congenital mitral stenosis.In rheumatic mitral stenosis, the mitral valve orifice is slowly diminished by progressive fibrosis, calcification of the valve leaflets, and fusion of the cusps and subvalvular apparatus. The flow of blood from LA to LV is restricted and left atrial pressure rises, leading to pulmonary venous congestion and breathlessness.
There is dilatation and hypertrophy of the LA. Any increase in heart rate shortens diastole when the mitral valve is open and produces a further rise in left atrial pressure. Situations that demand an increase in cardiac output also increase left atrial pressure, so exercise and pregnancy are poorly tolerated.
The mitral valve orifice is normally about 5 cm2 in diastole and may be reduced to 1 cm2 in severe mitral stenosis. Patients usually remain asymptomatic until the stenosis is less than 2 cm2. Reduced lung compliance, due to chronic pulmonary venous congestion, contributes to breathlessness, and a low cardiac output may cause fatigue.
Atrial fibrillation due to progressive dilatation of the LA is very common. Its onset often precipitates pulmonary oedema because the accompanying tachycardia and loss of atrial contraction lead to marked haemodynamic deterioration with a rapid rise in left atrial pressure. In contrast, a more gradual rise in left atrial pressure tends to cause an increase in pulmonary vascular resistance, which leads to pulmonary hypertension that may protect the patient from pulmonary oedema. Pulmonary hypertension leads to right ventricular hypertrophy and dilatation, tricuspid regurgitation and right heart failure.
Clinical features:
Effort-related dyspnoea is usually the dominant symptom. All patients with mitral stenosis, and particularly those with atrial fibrillation, are at risk from left atrial thrombosis and systemic thromboembolism. Prior to the advent of anticoagulant therapy, emboli caused one-quarter of all deaths.
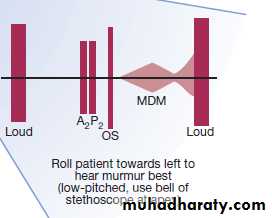
The physical signs of mitral stenosis are often found before symptoms develop and their recognition is of particular importance in pregnancy. The first heart sound (S1) is loud and can be palpable (tapping apex beat). An opening snap may be audible and moves closer to the second sound (S2) as the stenosis becomes more severe and left atrial pressure rises. However, the first heart sound and opening snap may be inaudible if the valve is heavily calcified. Turbulent flow produces the characteristic low pitched mid-diastolic murmur and sometimes a thrill. The murmur is accentuated by exercise. Pulmonary hypertension may ultimately lead to right ventricular hypertrophy and dilatation with secondary tricuspid regurgitation, which causes a systolic murmur and giant ‘v waves’ in the venous pulse.
Investigations:
Management:
Patients with minor symptoms should be treated medically. This consists of diuretic therapy to control pulmonary congestion. and in atrial fibrillation: anticoagulation to reduce the risk of systemic embolism and ventricular rate control (digoxin, β-blockers or rate-limiting calcium antagonists).
Intervention by balloon valvuloplasty, mitral valvotomy or mitral valve replacement should be considered if the patient remains symptomatic despite medical treatment or if pulmonary hypertension develops.
Mitral Regurgitation (MR)
Aetiology and pathophysiology:
Chronic mitral regurgitation causes gradual dilatation of the LA with little increase in pressure and therefore relatively few symptoms. Nevertheless, the LV dilates slowly and the left ventricular diastolic and left atrial pressures gradually increase as a result of chronic volume overload of the LV. In contrast, acute mitral regurgitation causes a rapid rise in left atrial pressure (because left atrial compliance is normal) and marked symptomatic deterioration.
Mitral valve prolapse:
This is also known as ‘floppy’ mitral valve and is one of the more common causes of mild mitral regurgitation. It is caused by congenital anomalies or degenerative myxomatous changes, and is sometimes a feature of connective tissue disorders such as Marfan’s syndrome.In its mildest forms, the valve remains competent but bulges back into the atrium during systole, causing a mid-systolic click but no murmur. In the presence of a regurgitant valve, the click is followed by a late systolic murmur, which lengthens as the regurgitation becomes more severe. A click is not always audible and the physical signs may vary with both posture and respiration.
Mitral valve prolapse is associated with a variety of typically benign arrhythmias, atypical chest pain and a very small risk of embolic stroke or TIA. Nevertheless, the overall long-term prognosis is good.
Clinical features of MR:
Symptoms depend on how suddenly the regurgitation develops. Chronic mitral regurgitation produces a symptom complex that is similar to that of mitral stenosis, but sudden-onset mitral regurgitation usually presents with acute pulmonary oedema.The regurgitant jet causes an apical systolic murmur, which radiates into the axilla and may be accompanied by a thrill. Increased forward flow through the mitral valve causes a loud third heart sound and even a short mid-diastolic murmur. The apex beat feels active and rocking due to left ventricular volume overload and is usually displaced to the left as a result of left ventricular dilatation.
Investigations:
Management:
Mitral regurgitation of moderate severity can be treated medically. In all patients with mitral regurgitation, high afterload may worsen the degree of regurgitation, and hypertension should be treated with vasodilators, such as ACE inhibitors. Patients should be reviewed at regular intervals because worsening symptoms, progressive cardiomegaly or echocardiographic evidence of deteriorating left ventricular function are indications for mitral valve replacement or repair.