Specialized EmbryologyGASTROINTESTINAL SYSTEM .The Foregut
The part of the foregut cranial to the side of the origin of the laryngotracheal groove forms part of the oral cavity as well as the pharynx,
while its caudal part to the groove develops into the following parts:
EsophagusStomach
Upper half of duodenum
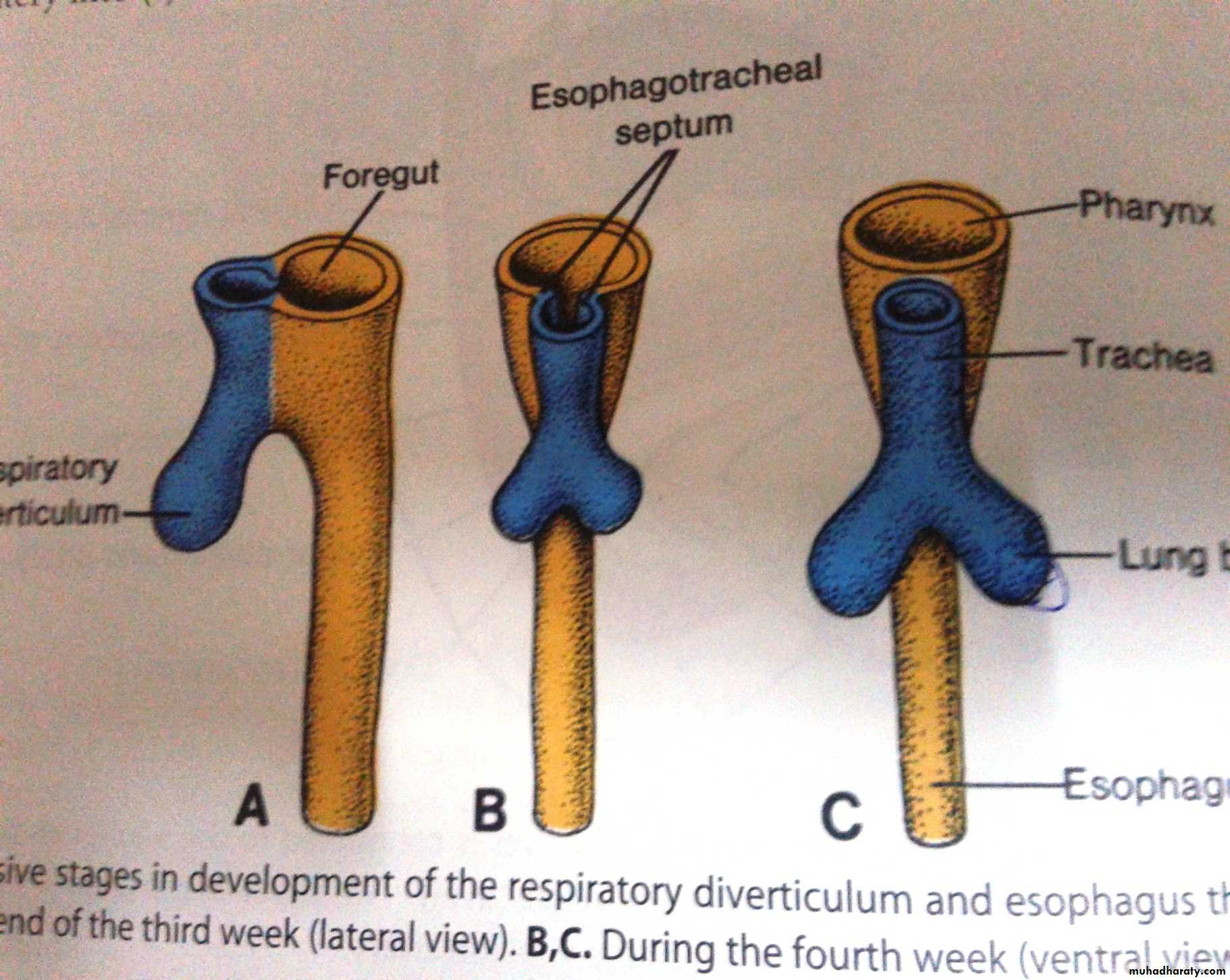
The esophagus develops the foregut just caudal to the opening of the laryngotracheal tube.
It is long and narrow tube ,then proliferation of its epithelial lining leads to transient obliteration of its lumen, which is rapidly becomes re-canalized again after short time.
• Congenital Anomalies
• 1.Esophageal stenosis due to incomplete re-canalization.• 2.Esophageal atrasia due to complete failure of re-canalization.
• 3.Abnormally short esophagus
• 4.A patch of epithelial lining the esophagus may differentiate into gastric mucosa (secrete HCl and leads to ulceration of the lower part of Esophageal mucosa).
• Tracheo-esophageal fistula due to failure of separation.
STOMACH
It develops from the caudal part of the for gut as spindle –shaped dilatation which attached ventrally by ventral mesogastrium and dorsally by dorsal mesogastrium.The liver will formed inside the ventral mesogastrium ,thus dividing it into :
Lesser omentum between porta hepatis of liver and lesser curvature of somach.Falciform and coronary ligament ,it is ligament that connects the liver to the inner surface of anterior abdominal wall(new umbilicus)and diaphragm.
The spleen develops in the dorsal mesogastrium and divides it into:
Gasrtosplenic ligament
Leinorenal ligament
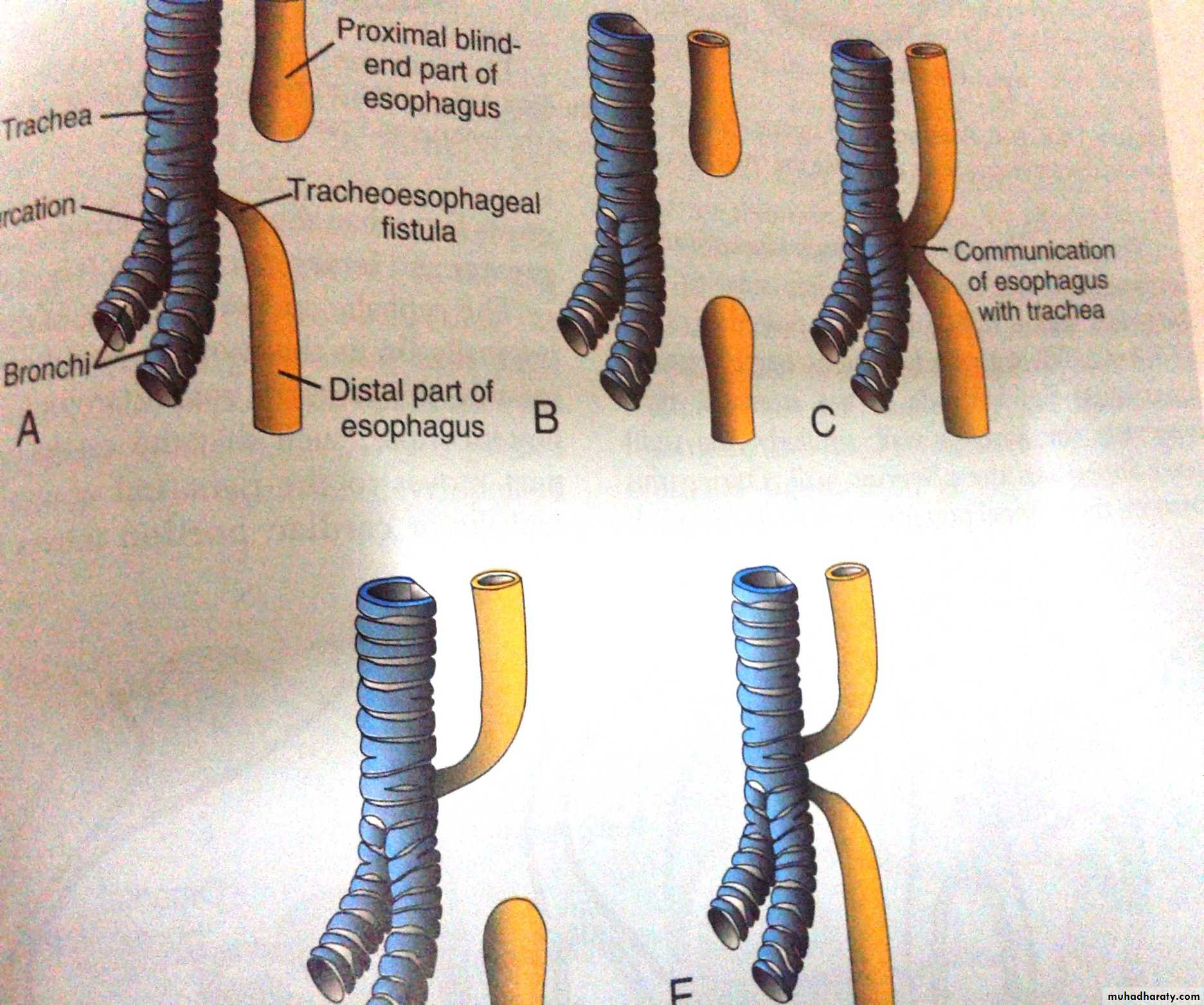
Rotation of stomach
The stomach differentiate more and thus fundus ,greater and lesser curvatures become very clear, now lesser curvature faces ventrally ,while ,greater curvature faces dorsally.Then the stomach rotates 90° clockwise rotation, thus lesser curvature faces to the right while the greater one faces to the left.
As the result of this rotation a small space becomes trapped between the lesser omentum ,posterior surface of stomach and upper part of posterior abdominal wall(stomach bed)this space is known as omental bursa or lesser sac which communicates with the general peritoneal cavity by the epiploic foramen.

Congenital Anomalies of Foregut
Congenital hypertrophic pyloric stenosis cause projectile vomitingEctopic pancreatic tissue may develops inside the submucosa of pyloric antrum due to invasion of the stomach by the pancreatic bud
Duplication of stomach an d abnormal shaped prepyloric septum
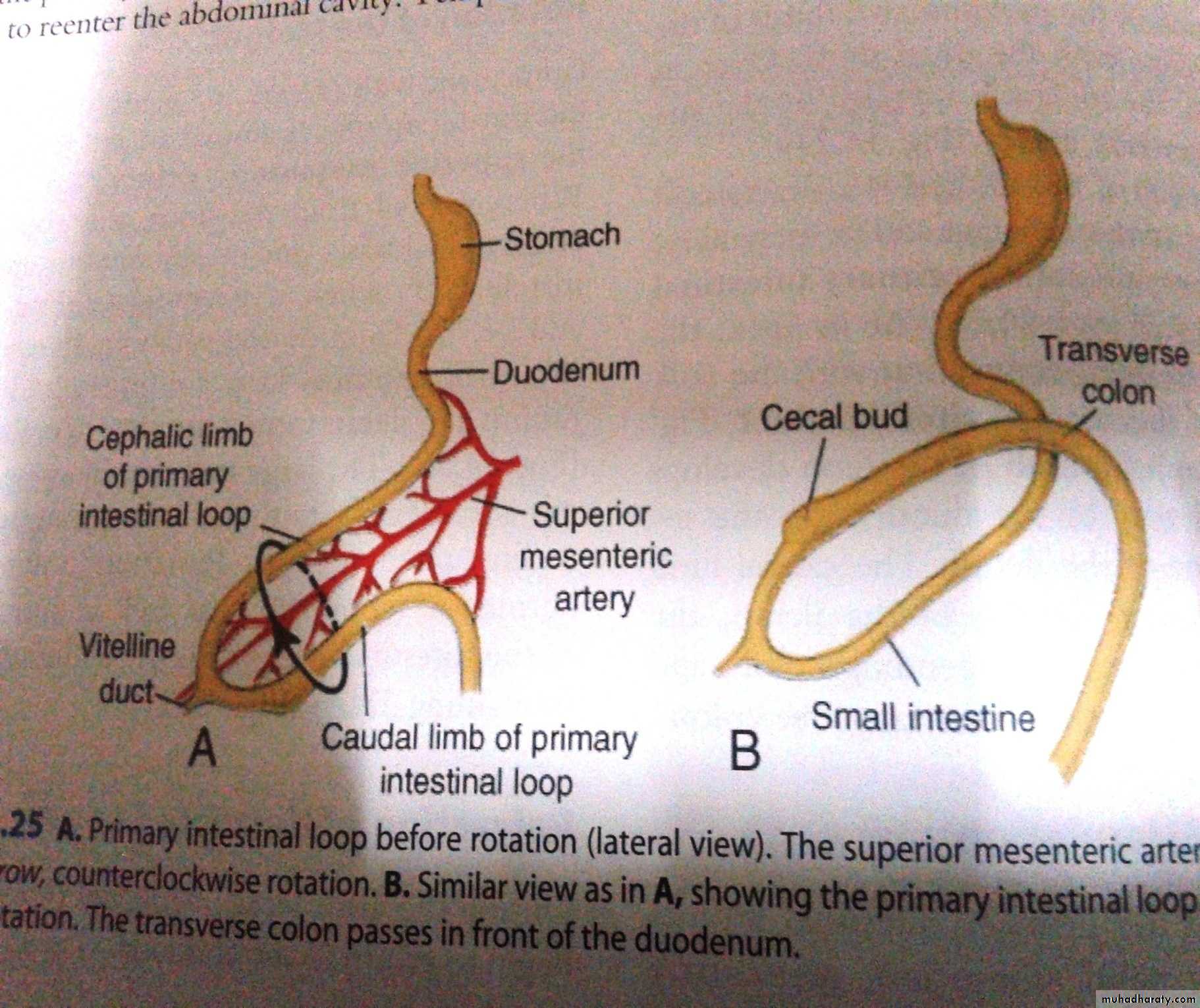
The Mid gut
• It grows faster than the vertebral column ,thus it will becomes U-shaped structure with inverted apex.
• This structure has a proximal (cranial) and distal (caudal) limbs with superior mesenteric artery in between the two limbs, while the apex is connected to the umbilicus by vitelline ligament.
The cranial limb will give rise into:
Caudal half of duodenumJejunum
Most of ileum
The caudal limb will give rise into:
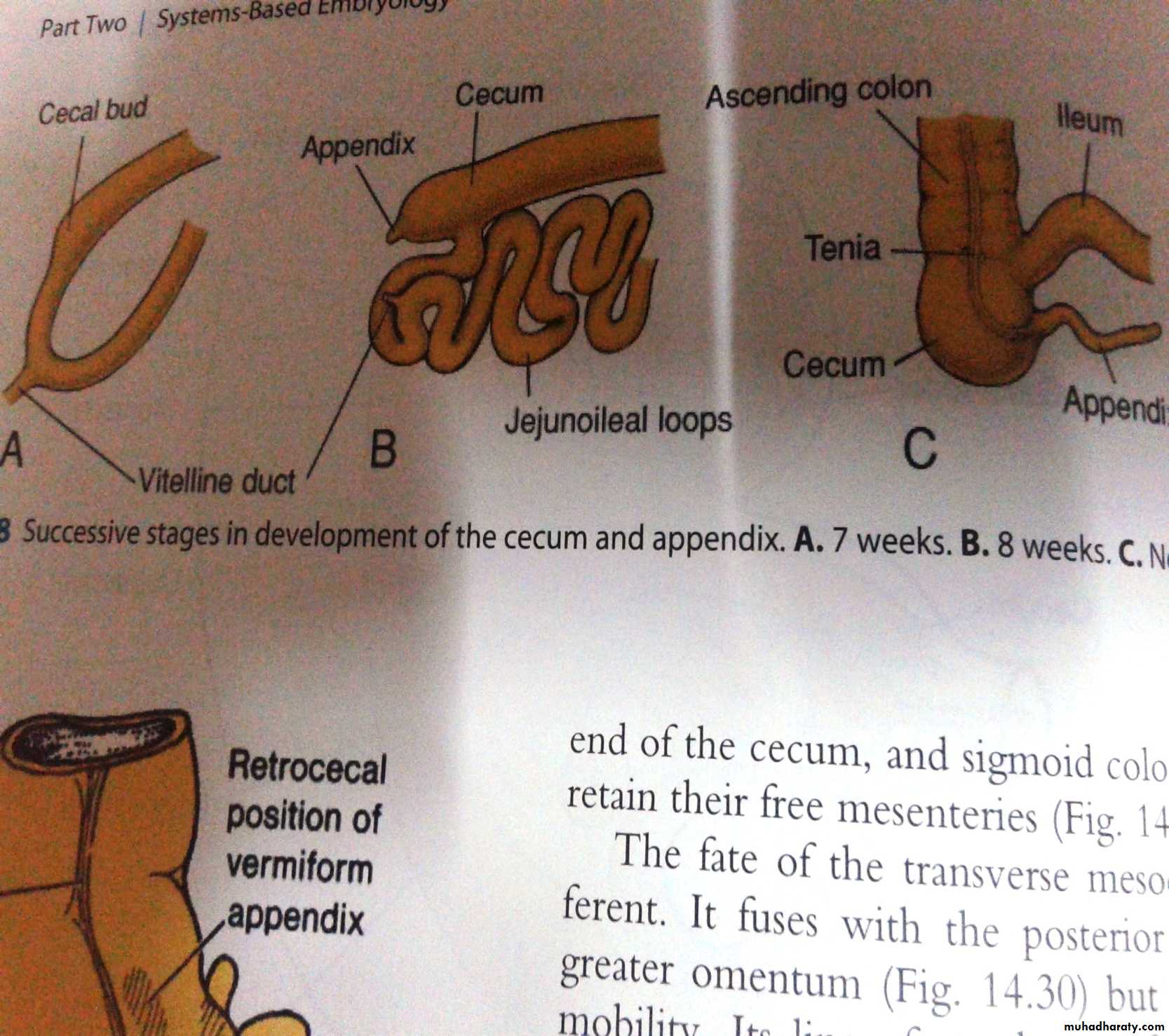
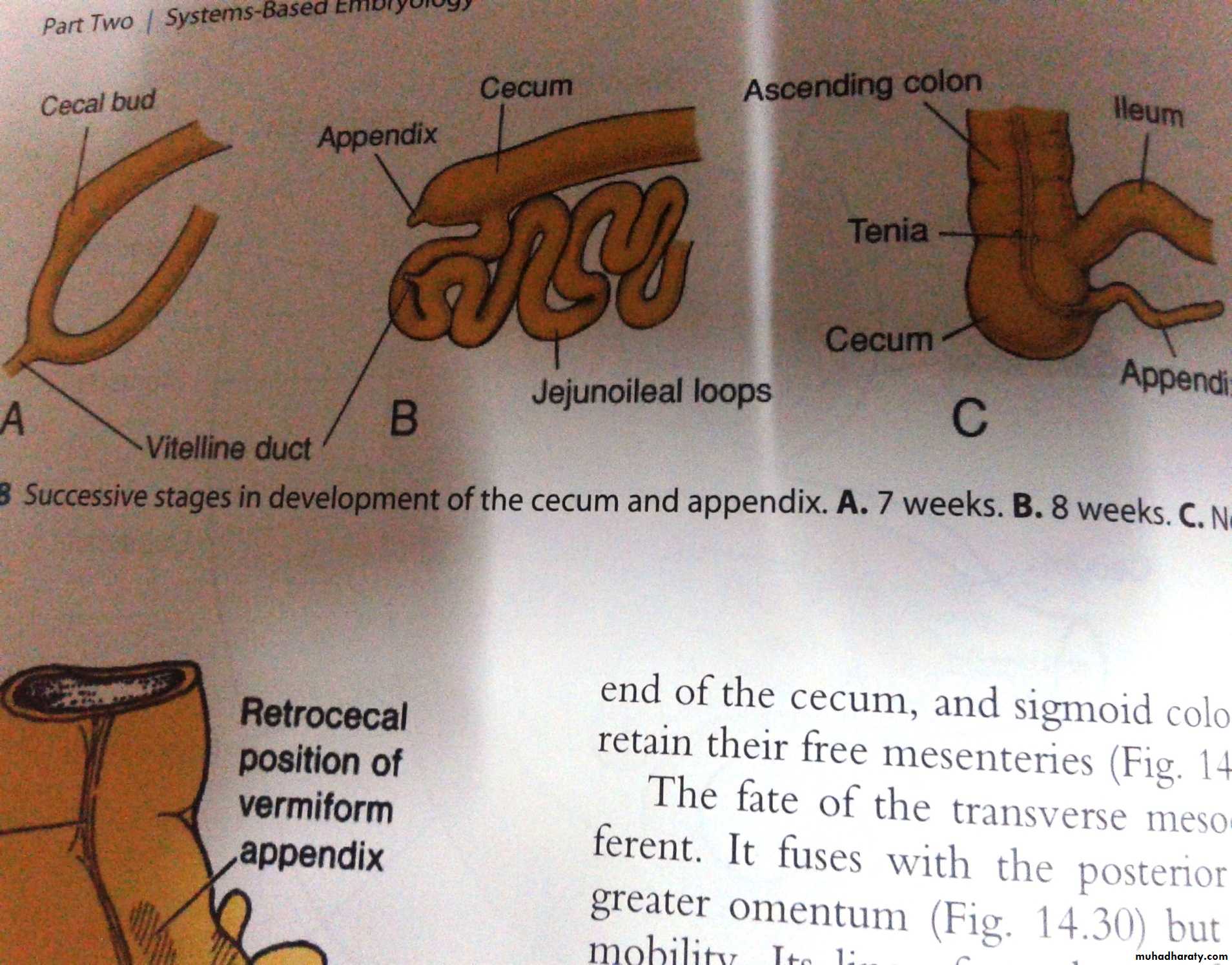
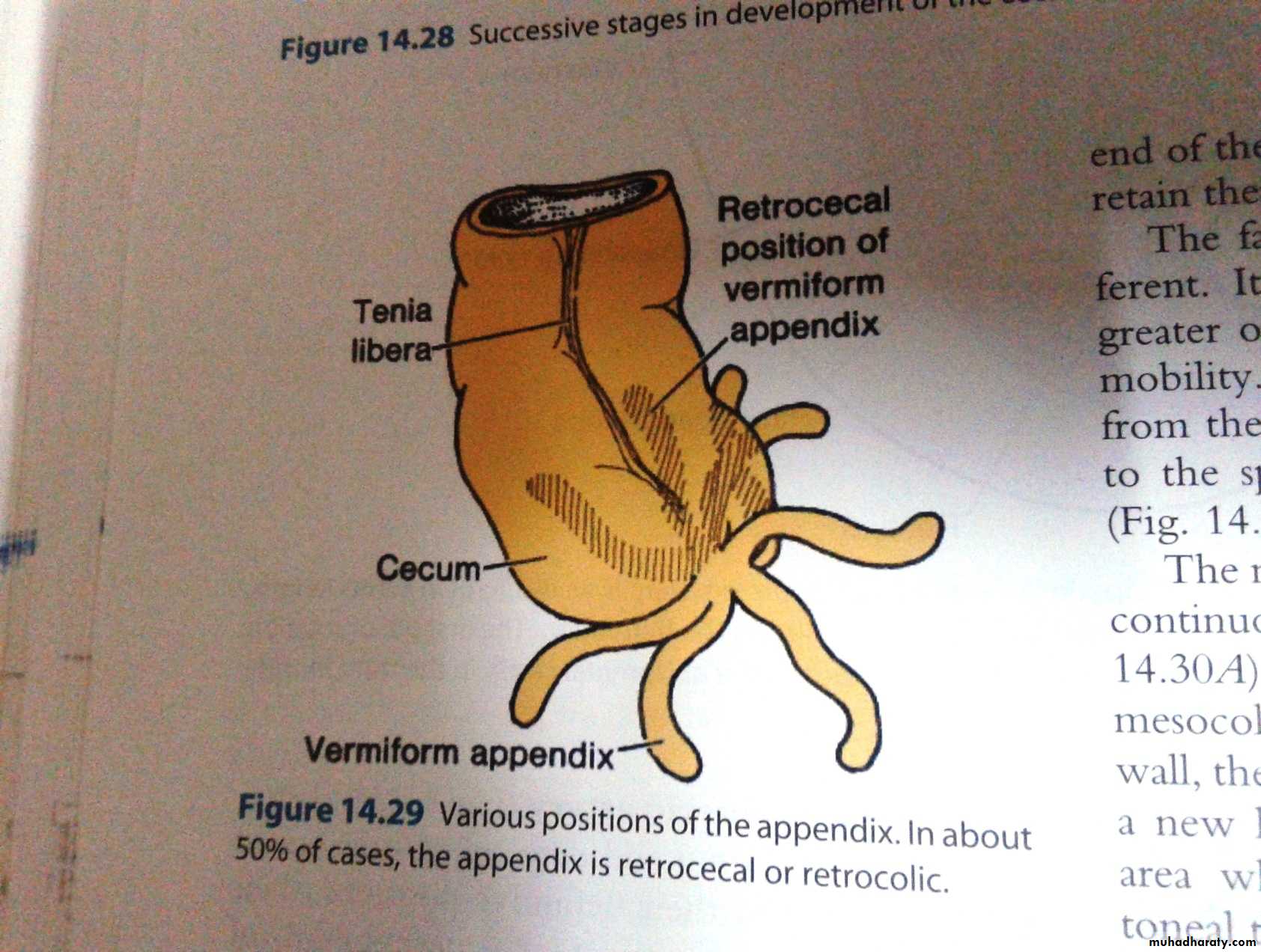
Terminal part of ileumCaecum and appendix
Ascending colonRight 2/3of transverse colon
The caecum with the appendix attached to its tip arises as a conical diverticulum from the caudal limb close to the apex of the loop, i.e the point of attachment of the vitello-intestinal duct.
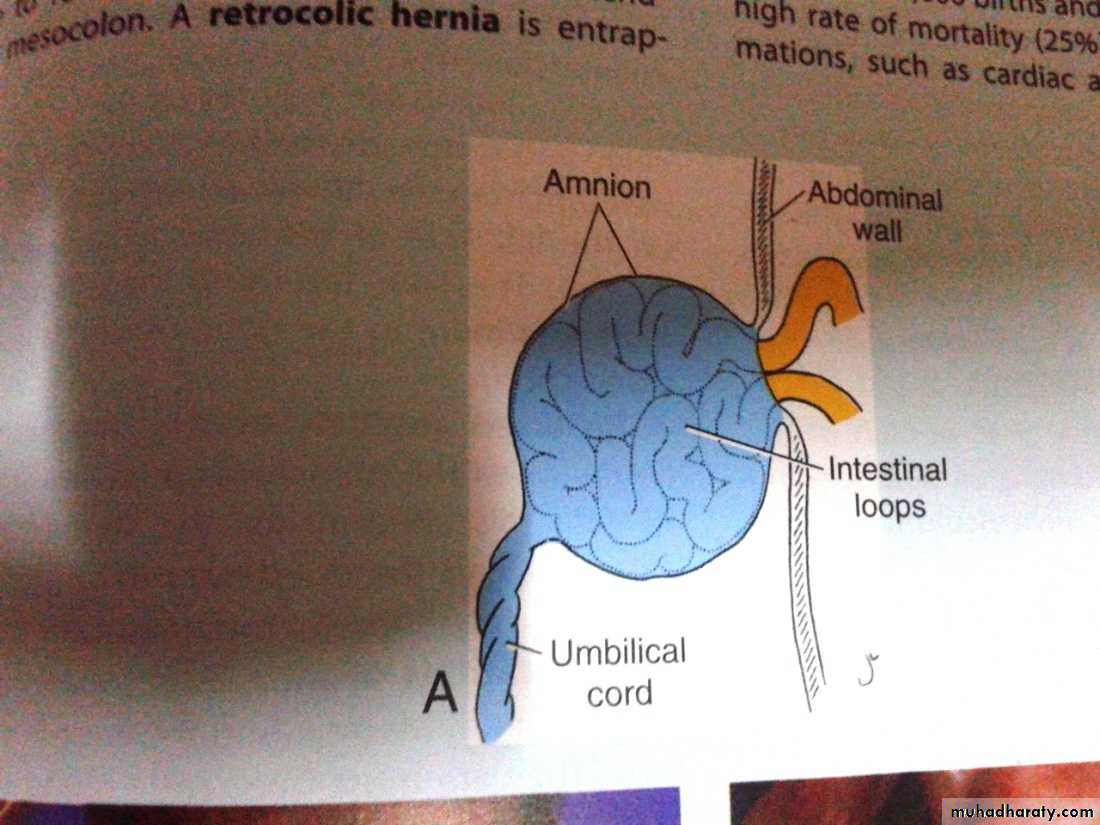
The u-shaped loop projects inside the umbilical cord to form the umbilical hernia of the fetus which is a normal feature between the 6th -12th weeks of intrauterine life.
Such hernia is due to :
inadequacy of abdominal cavity which is largely occupied by:1.The rapidly growing liver.
2.The large sized mesonephron on each side of the vertebral column.By the end of the 12thweek of development ,the loop of the intestine starts to return back into the abdominal cavity because of the following reasons:
1.Regression of mesonephrons.
2.No more increase in the size of the liver.3.An increase in the expansion o the abdominal cavity with an increase in the length of the abdominal wall.
Rotation of the loop and reduction of the hernia
Just before the reduction is started ,the loop will rotate 90° anticlockwise, thus the original proximal limb comes to the right while the distal comes to the left.
Once reduction starts the loop will complete its rotation anticlockwise to an angle of 270°, so that the original caudal limb comes to the right and superficial.
The last segment to inter is the caecum which comes to lie superficial to small intestine .
The caecum the descends from just below the liver to reach its adult position (the right iliac fossa).
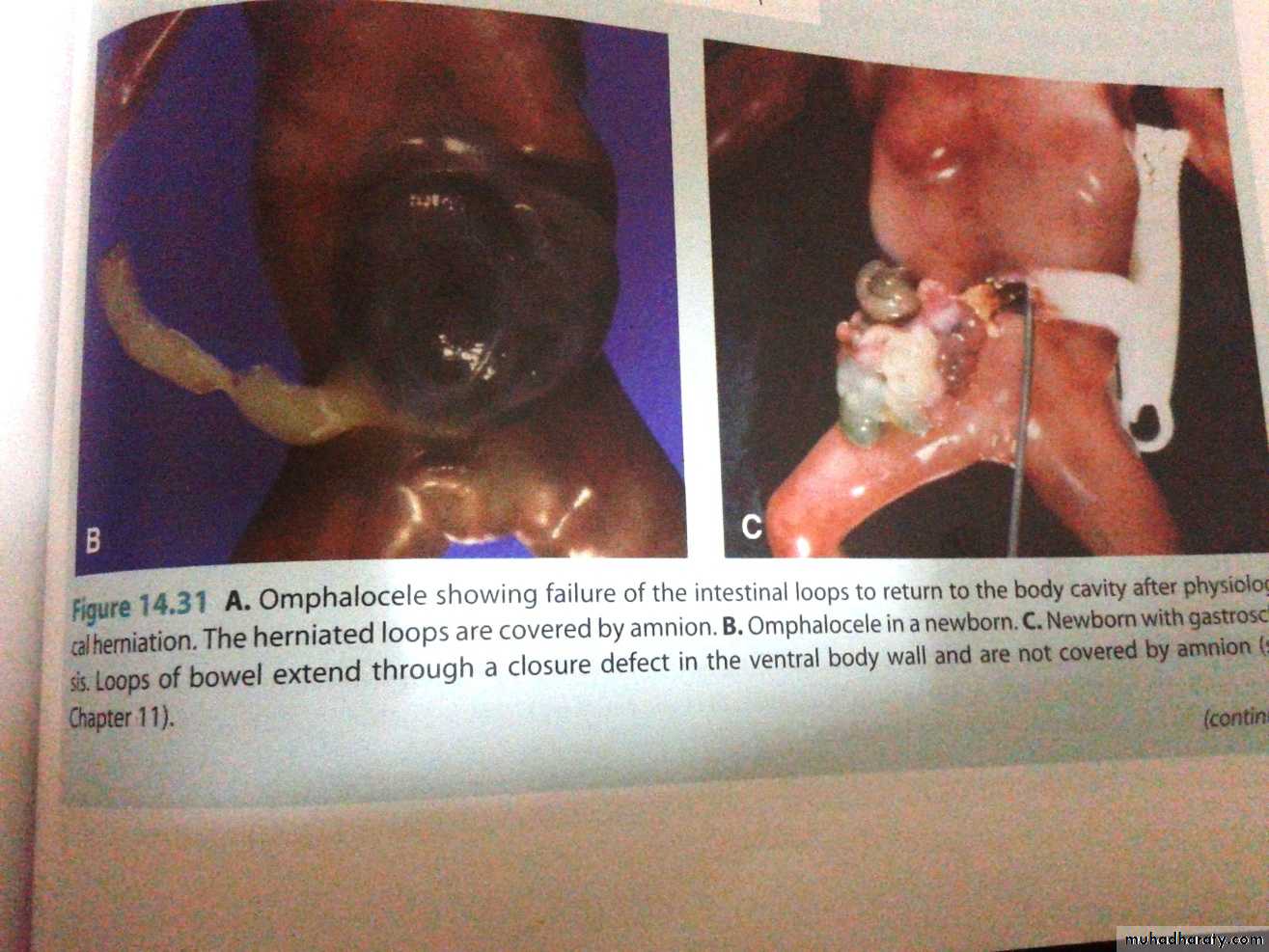
Congenital Anomalies of Mid gut
• Incomplete reduction results in (omphalocele),where the loop is trapped outside and covers only by amnion of the embryo.
• Incomplete reduction may result congenital umbilical hernia, which is mainly due to defect in the central part of the abd wall.
• The mid gut loop may rotate in opposite direction(clockwise) leading to reverse position of the duodenum and becomes superficial to the colon.
Anticlockwise rotation to 90° only leads to reverse position of abdominal content(situs in versus).
Sub hepatic position of caecum and appendix as it fails to descend to right iliac fossa.
Ligaments: They include:
Meckel’s diverticulum ,it measures 2 inches in length, and about 2 feets proximal to ilio-caecal valve and is seen in 2% of population.Vitello-intestinal fistula connect the intestine with the umbilicus and discharge some of the intestinal contents into the umbilicus.
The whole duct may persists as fibrosed cord extending from the umbilicus to the ileum.
A part of the duct may persists and forms vitelline cyst along the course of the duct.