
Lecture 4 Dr. Janan Alrefaee
Reabsorption and secretion along different parts of the nephron
Tubular reabsorption is highly selective unlike glomerular filtration which is nonselective.
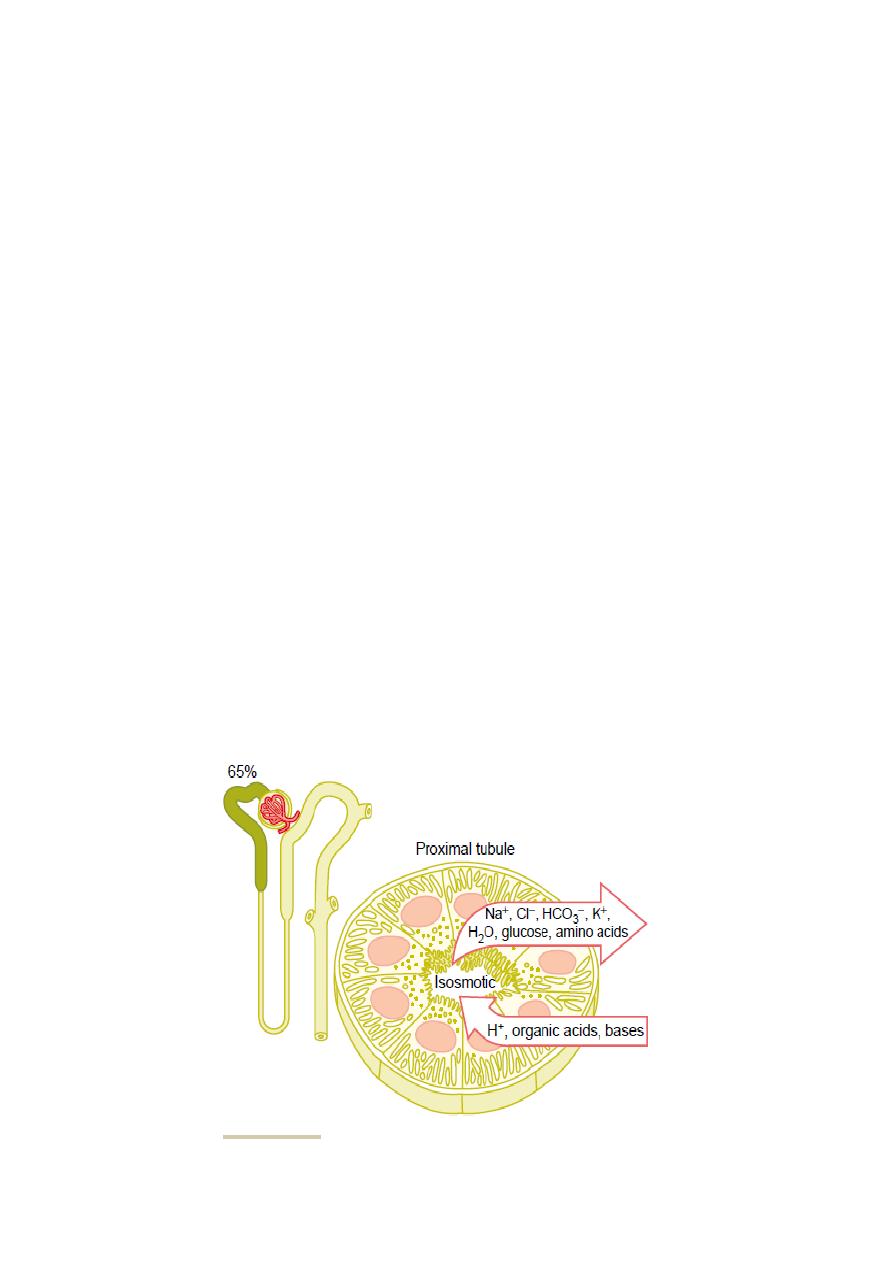
1-Proximal tubular reabsorption
Normally, about 65 % of the filtered load of sodium and water and a slightly lower
percentage of filtered chloride are reabsorbed by the proximal tubule before the filtrate
reaches the loops of Henle.
*The osmolarity remains constant (isotonic, 300 mOsm/L), along the proximal tubule
because the water reabsorption of the proximal tubules proportional to Na reabsorption.
*The high capacity of the proximal tubule reabsorption results from its special
epithelial cell characteristics (Fig.4.1), as following:
1- Highly metabolic. 2- Have large numbers of mitochondria for active transport. 3- Have an
extensive brush border on the luminal (apical) side of the membrane and have extensive
labyrinth of intercellular and basal channels which provide an extensive membrane surface
area on the luminal and basolateral sides of the epithelium. 3-The brush border is loaded with
carrier protein.
The reabsorbtion and secretion of the proximal tubule as follow:
*In the first half of the proximal tubule: sodium is co-transport with glucose, amino acid
and other solutes.
*In the second half of the proximal tubule: a little glucose and amino acids remain to be
reabsorbed from its lumen, while sodium is reabsorbed mainly with chloride as high chloride
concentration.
* Others as HCO3- and K+ are reabsorbed from proximal tubule.
* Proximal tubule is moderately passively reabsorbed urea.
*Sodium is reabsorbed by counter-transport secreting hydrogen ions into tubular lumen.
*The proximal tubule is also the site for secretion of organic acids and bases (bile salts,
oxalate, urate, catecholamines),drugs, toxins and para-aminohippuric acid (PAH).*The
average person can clear about 90 % of the PAH from the plasma flowing through the
kidneys and excrete it in the urine, so PAH clearance is used to estimate the renal plasma
flow).

2-Solute and water transport in the Loop of Henle
The thin descending and thin ascending segments of the loop of Henle have thin epithelial
membranes with no brush borders, few mitochondria, and minimal levels of metabolic
activity (Fig. 4.2).
In descending thin segment about 20 % (high permeability) of the filtered water is
reabsorbed but it is moderately permeable to urea and sodium. The ascending limb,
including both the thin and the thick portions, is impermeable to water.
The thick segment of the loop of Henle has thick epithelial cells that have high metabolic
activity (Fig. 4.2). About 25 % of the filtered loads of sodium, chloride, and potassium are
reabsorbed in the loop of Henle, mostly in the thick ascending limb.
*The thin segment of the ascending limb has a much lower reabsorptive capacity than the
thick segment.
In the thick ascending limb (Fig. 4.3), the sodium is reabsorbed by 1- 1sodium-2chloride-
1potassium co-transporter {by it, the energy from downhill sodium reabsorption drive the
potassium reabsorption uphill (its action is inhibited by“loop” diuretics as furosemide)}.and
2- by sodium hydrogen counter-transport mechanism.
*There is also paracellular reabsorption of Mg++, Ca++, Na+, and K+, in the thick segment
due to relative more +ve charge in lumen than interstitial fluid due to a slight backleak of
potassium ions into the lumen.
Distal Tubule
The first portion of the distal tubule is part of the juxtaglomerular complex. The next part is
the early distal tubule is highly convoluted and reabsorbs sodium, potassium, and chloride,
but is impermeable to water and urea (diluting segment). About 5 % of sodium chloride is
reabsorbed in the early distal tubule by sodium-chloride co-transporter (inhibited by thiazide
diuretics) (Fig. 4.4). Chloride diffuses from the cell into the renal interstitial fluid through
chloride channels in the basolateral membrane (Fig. 4.5).
Late distal tubule and cortical collecting tubule: both have same functions which are:
1- Both have two cell types, the principal cells and the intercalated cells (Fig. 4.4).
*Principal cells: reabsorb sodium and secrete potassium (depend on Na-K ATPase pump
and concentration gradient) under the effect of the aldosterone hormone (Fig. 4.6). Principal
cells reabsorbe water as well.
*Intercalated cells secrete hydrogen (by hydrogen-ATPase) and reabsorb both
bicarbonate and potassium ions.
2- Almost completely impermeable to urea.
3-The permeability of both segments to water is controlled by the concentration of
antidiuretic hormone ADH (vasopressin). With high levels of ADH, these tubular segments
are permeable to water, but in the absence of ADH, they are almost impermeable to water.
Medullary collecting duct (fig. 4.7)
It is the final site process the urine and reabsorbs less than 10 % of the filtered water and
sodium. The epithelial cells of it are nearly cuboidal with smooth surfaces and relatively few
mitochondria. The characteristics of medullary collecting duct are:
1. The permeability of it to water is controlled by the level of ADH (
ADH increases its
permeability to water forming concentrated urine).
2. It is permeable to urea (important in concentrated urine).
3. It secretes hydrogen ions against a large concentration gradient (important in acid-base
balance).
Concentrations of different solutes in the different tubular segments:
A solute concentration in the tubular fluid is determined by its degree of reabsorption versus
water reabsorption. Inulin, is not reabsorbed or secreted by the renal tubules, so its
concentration reflect water reabsorption at different parts of the renal tubule.
Figure 4.1 Cellular ultrastructure and primary transport characteristics of the
proximal tubule
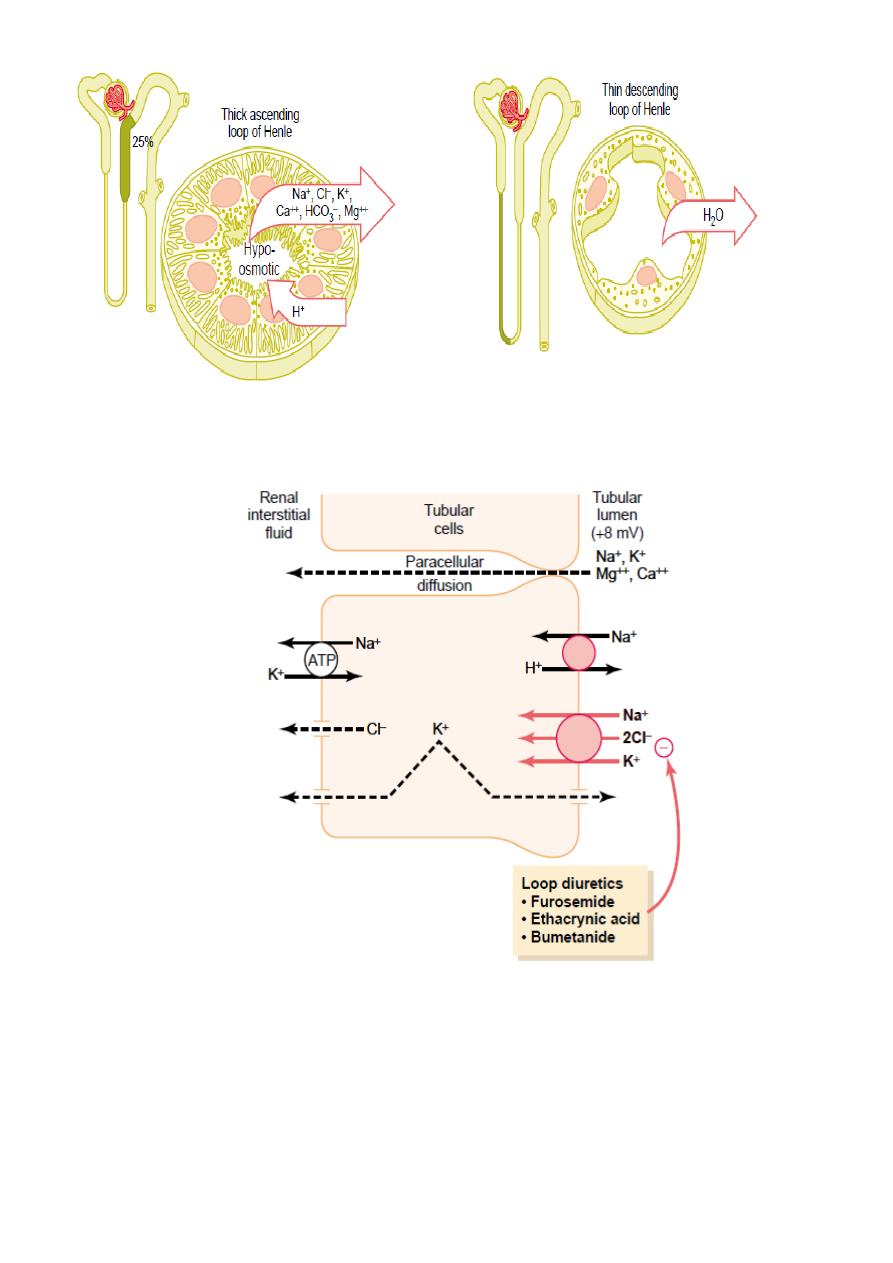
Figure 4.2 Cellular ultrastructure and transport characteristics of loop of Henle
Figure 4.3 Mechanisms of sodium, chloride, and potassium transport in the thick
ascending loop of Henle.
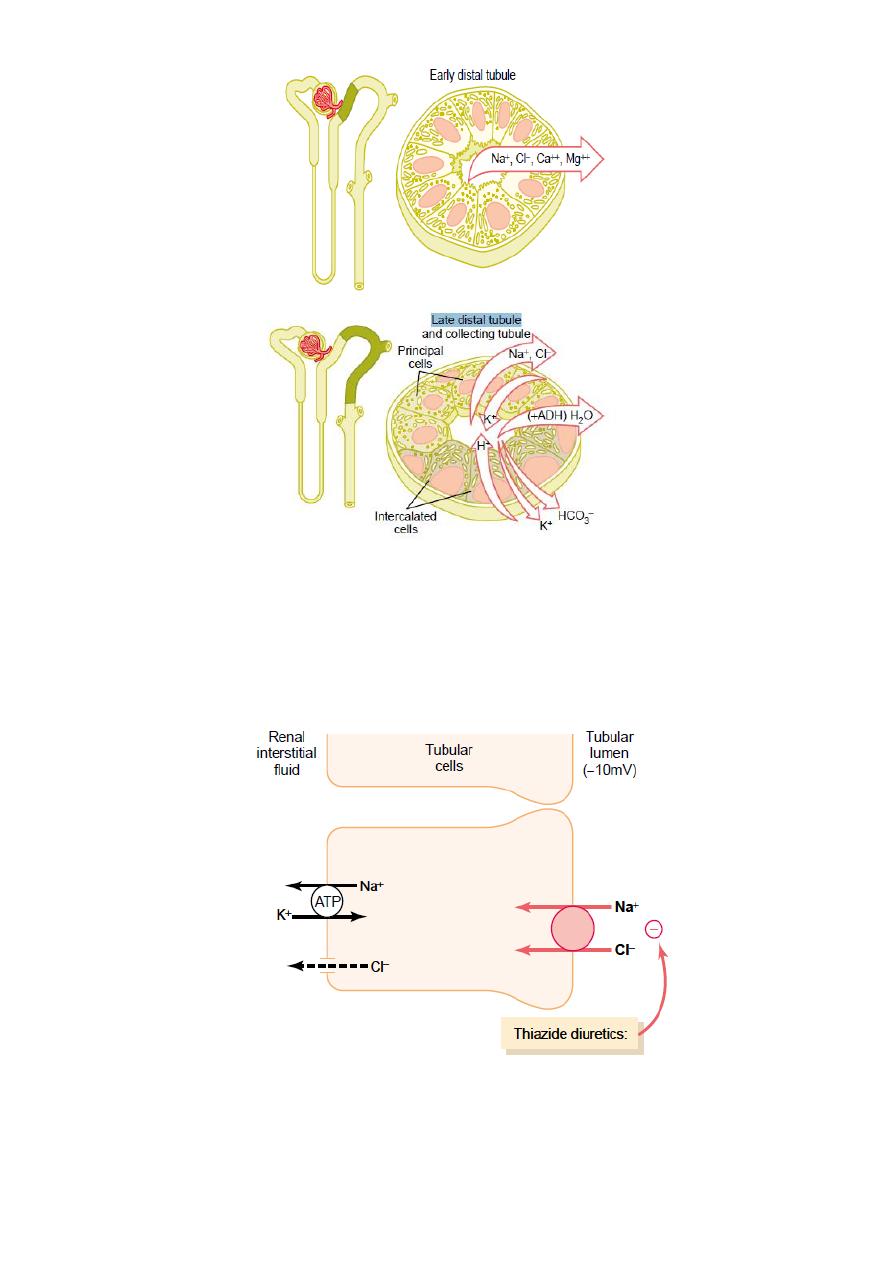
Figure 4.4 Cellular ultrastructure and transport characteristics of the early distal
tubule and the late distal tubule and collecting tubule.
Figure 4.5 Mechanism of sodium chloride transport in the early distal tubule
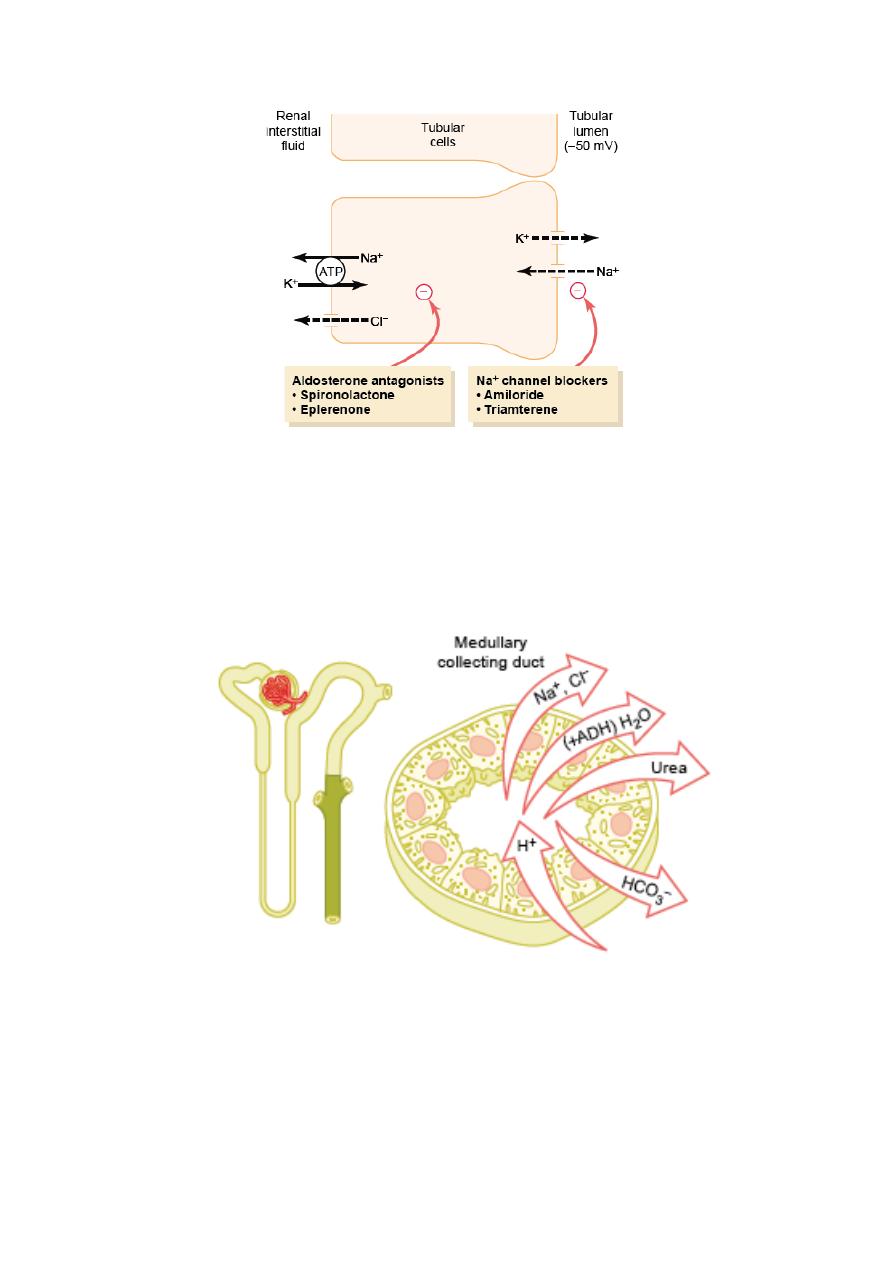
Figure 4.6 Mechanism of sodium chloride reabsorption and potassium secretion in the
late distal tubules and cortical collecting tubules.
Figure 4.7 Cellular ultrastructure and transport characteristics of medullary collecting
duct.