
بسم الله الرحمن الرحيم
Classification of periapical disease
Acute apical periodontitis
It is an acute painful inflammation of the periodontium.
Etiology: Occlusal trauma, egress of bacteria from infected
pulps, toxins from necrotic pulps, chemicals, irrigants or over instrumentation in root canal therapy.
Signs and symptoms: Clinically, the tooth is tender to biting.
Widening of the periodontal space may be seen on a radiograph.
Treatment: range from occlusal adjustment to root canal therapy or extraction.Chronic apical periodontitis
It is a chronic inflammation of the periodontium.Etiology: Chronic apical periodontitis occurs as a result of pulp necrosis.
Signs and symptoms: Affected teeth do not respond to pulp sensitivity tests.
Tenderness to biting is usually mild; however some tenderness may be noted to palpation over the root apex.

Radiographic appearance is varied, ranging from minimal widening of the periodontal ligament space to a large area of destruction of periapical tissues.
Treatment: Root canal therapy or extraction.
Condensing osteitis
Condensing osteitis is a variant of chronic apical periodontitis and represents a diffuse increase in trabecular bone in response to irritation.Radiographically, a concentric
radio-opaque area is seen around the offending root.
Treatment: is only required if symptoms/pulpal diagnosis indicate a need.

Acute apical abscess
An acute apical abscess is a severe inflammatory response to microorganisms or their irritants that have leached out into the periradicular tissues.Signs and symptoms: It varies from moderate discomfort or swelling to systemic involvement, such as raised temperature and malaise. Teeth involved are usually tender to both palpation and percussion.
Radiographic changes are variable depending on the amount of periradicular destruction already present; however, usually there is a well-defined radiolucent area, as in many situations an acute apical abscess is an acute exacerbation of a chronic situation.
Treatment: Initial treatment of an acute apical abscess involves removal of the cause as soon as possible.
Drainage should be established either by opening the tooth or incision into a related swelling.
An antibiotic may need to be prescribed, depending on the patient’s condition. Once the acute symptoms have subsided, then root canal therapy or extraction may be performed.
Chronic apical abscess
In a chronic apical abscess, the abscess has formed a communication through which it discharges. Such communications may be through an intraoral sinus or, less commonly, extraorally. Alternatively the discharge may be along
the periodontal ligament; such cases resemble a periodontal pocket.
Usually these communications or tracts heal spontaneously following root canal therapy
or extraction.
• A tooth with a chronic apical abscess will not generally present with clinical symptom.
• This tooth will not respond to pulp vitality tests.
• Radiographicaly will exhibit an apical radiolucency.
• The tooth is generally not sensitive to biting pressure but can “feel different” to the patient on percussion.
• The entity is distinguished from asymptomatic apical periodontitis because it will exhibit intermittent drainage through an associated sinus tract.
Access Opening
Access opening is the cavity that is prepared in the crown of a tooth toobtain adequate and direct access (straight line access) to the apical foramen to ensure free movement of the instruments during pulp extirpation, preparation and obturation of the root canal.
Objectives of Access Opening:
1) To facilitate visualization of all the root canal orifices.
2) To provide direct access to the apical portion of the canal.
The outline form of the access cavity must be correctly shaped and positioned according to:
a- The size of the pulp chamber.
b- The shape of the pulp chamber.
c- The number of individual root canals and their direction of curvature.
The outline form is affected by the size of the pulp chamber, so access opening for young patients is larger, because the pulp chamber is larger, while in old patients the pulp chamber is smaller.
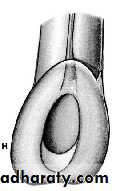
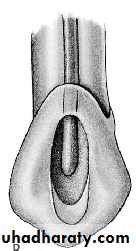
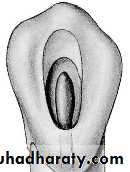
The finished outline should reflect accurately the shape of the pulp chamber, e.g. in premolars the pulp chamber is oval in cross section so the access opening is oval, elongated buccolingually than mesiodistally (following the pulp chamber shape).
Sometimes a modification is needed to get the
objective of access opening.
The number of individual root canals and their curvature modifies the outline of the access opening. Sometimes we have to remove part of a cusp of a molar or incisal ridge in order to facilitate better visualization to the root canals.
The dentist must be able to see, locate and reach by the instruments each
root canal.Shape of access opening for each anterior tooth
1- Maxillary Central Incisor: The access opening is triangular in shape.
The root is straight, single, large, oval at the beginning, then tapered
till it becomes rounded apically.
2- Maxillary Lateral Incisor: Similar in shape to the max. central incisor,
but smaller in size with: disto-palatal curvature at the apex of theroot.
3- Maxillary Canine: The canal is big and it is wider buccoingually
than mesiodistally. At the cervical third the orifice is oval, at the
middle third: it is oval., and in the apical third it is rounded.
4- Mandibular Incisors: If we take an x-ray from buccal direction we
will find small, tiny root canal, but if we take an x-ray film frommesial or distal direction, we will find large, wide pulp “labiolingually”
with a possibility of two canals one labially and the second
one is located lingually, so we have to widen the root canal orifice
“Labiolingually”.
Also, in the lower incisor, some times we have slight curvature in the
root apex “to the lingual side” so, there is a possibility of perforation
during instrumentation.
.

5- Mandibular Canine: There is one canal which is big and oval in shape. Another root canal may be present lingually to the major
root canal but this rarely happens

Thank You
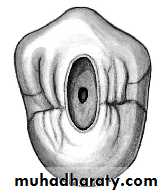
Access openings of each posterior tooth1- Maxillary first premolar-
- Access opening: ovoid and elongated buccopalatally.
- The canal shape is wide in buccopalatal direction at cervical portion, slight ovoid at mid-root and rounded at apical third.
- Canal Orifices: below and slightly central to cusps tips. -

Multiple canal possibilities:
(i) 20% single canal in single root, elliptical or figure (8) inshape, wider buccopalatally than mesiodistally. It may be
mistaken as two canals.
(ii) 80%: two canals, either single root with either one or two
apical foramenae, or two canals with two separated roots “and the palatal one is
longer”.
(iii) Rarely there are (3) roots with (3) root canals.
Type (ii)or (iii), usually have two roots.
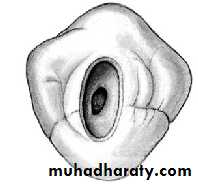
2- Maxillary Second Premolar
- Mostly it has a single root and the canal shape is ovoid and
very wide in buccopalatal direction, ovoid in the mid root, and
rounded in the apical area.
- Canal orifice is centrally located and often appears as a slot
than as a single ovoid opening.
- Multiple canals possibilities: 40% 2 canals, 60% one
canal.
3- Mandible First Premolar:
Mandibular first premolar has well developed buccal cusp and a small lingual cusp, the root is more rounded than mandibular second premolar and shorter.The pulp chamber is ovoid and buccal pulp horn higher.
- Canal shape: At cervical level is wide in buccolingual dimension. At the mid-root area it is ovoid and at the apical third it is rounded.
- Canal configuration possibilities: Type I = 73.5%, Type II =
6.5%, Type III =19.5% We may also see Type IV.- Access opening: ovoid and made slightly buccally to the central groove and the final preparation should have a slightly lingual inclination.
4- Mandibular second Premolar:
It has a well developed buccal cusp and much less formed lingual cusp.There is a one root canal, and the pulp chamber is gradually
merging with root canal.
- Canal orifice:
a- At cervical wide in buccolingual dimension.
b- Mid-root level elongated ovoid.
c- Apical third level generally round.
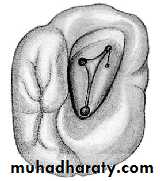
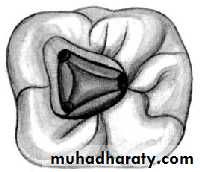
5- Maxillary 1st Molar
- There are three roots, with three root canals mesiobuccal, distobuccal, andpalatal canal which is the biggest one.
- The access opening is in the mesial part of the tooth and we
may leave the oblique ridge as it is if it is caries free.
- The final preparation of the access opening is triangular in
shape and there are three canals:
a- Mesiobuccal canal: It is a tiny canal, difficult to find. It is
possible to find another mesiobuccal canal (70%) lingual to the
main one.
b- Distobuccal canal: It is toward the distopalatal side.
- The palatal canal: It is in between.
6- Maxillary 2nd Molar
- Similar to max. 1st molar but the distobuccal canal is located inbetween the mesiobuccal canal and palatal canal and slightly
distally.
- Variations: We may have 2 canals: one buccally and one
palatally instead of 3 canal, in this case the two canals are large in
size and opposite to each other.
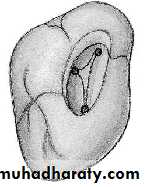
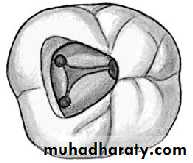
7- Mandibular 1st Molar
- There are 3 canals, 2 mesial “mesiobuccal and mesiolingual” and one locateddistally.
- We start preparation in mesial part of the tooth and access
opening is triangular-rectangular in shape.
- There is a possibility of 2 canals located distally (33%)
“and they may end with separate orifices or joined orifice so
if the distal canal is tiny and more toward the buccal side
then the possibility of 2 canals is high but if it is in the center buccolingually
then the possibility of one canal is high.
8- Mandibular 2nd Molar
- The access opening resembles that of the mand. 1st molar with 3 root canals, 2 mesially and 1 distally.- There is a possibility of 2 canals: mesial canal and distal canal with each canal opposite to other.
- Mesial canal is larger than the distal one.
Isthmus classification:
An isthmus is a narrow, ribbon-shaped communication between two root canals that contains pulp or pulpally derived tissue. All isthmi must be found, prepared, and filled during surgery, because they can function as bacterial reservoirs. Any root with two or more canals may have an isthmus. Therefore the presence of an isthmus should be suspected whenever multiple canals are seen on a resected root surface.Type I: is an incomplete isthmus; it is a
faint communication between two canals.
Type II: is characterized by two canals with a
definite connection between them (complete isthmus).
Type III: is a very short, complete isthmus between two canals.

Type IV: is a complete or incomplete isthmus between three or more canals.

Type V: is marked by two or three canal openings without visible connections.
