1
د. رؤى طفيليات
31
\
2
\
2132
( عدد االوراق
2
) م
\
1
\
موصل
lec: 1+2
Helminthes
class Trematode
Objectives:
• Learn students, the General characteristics of Trematodes.
Morphology, types of life cycle. Some thing about pathogenicity,
symptoms and diagnosis.

2
Flukes
Fluke
Introduction
*Helminthes are world wide in distribution. *Helminthic
infections are common in the countries with poor hygiene and low socio-
economic conditions. *The climate, food habits, exposure to vectors etc.,
are other factors, which influence the prevalence of the disease in the
community.
Introduction
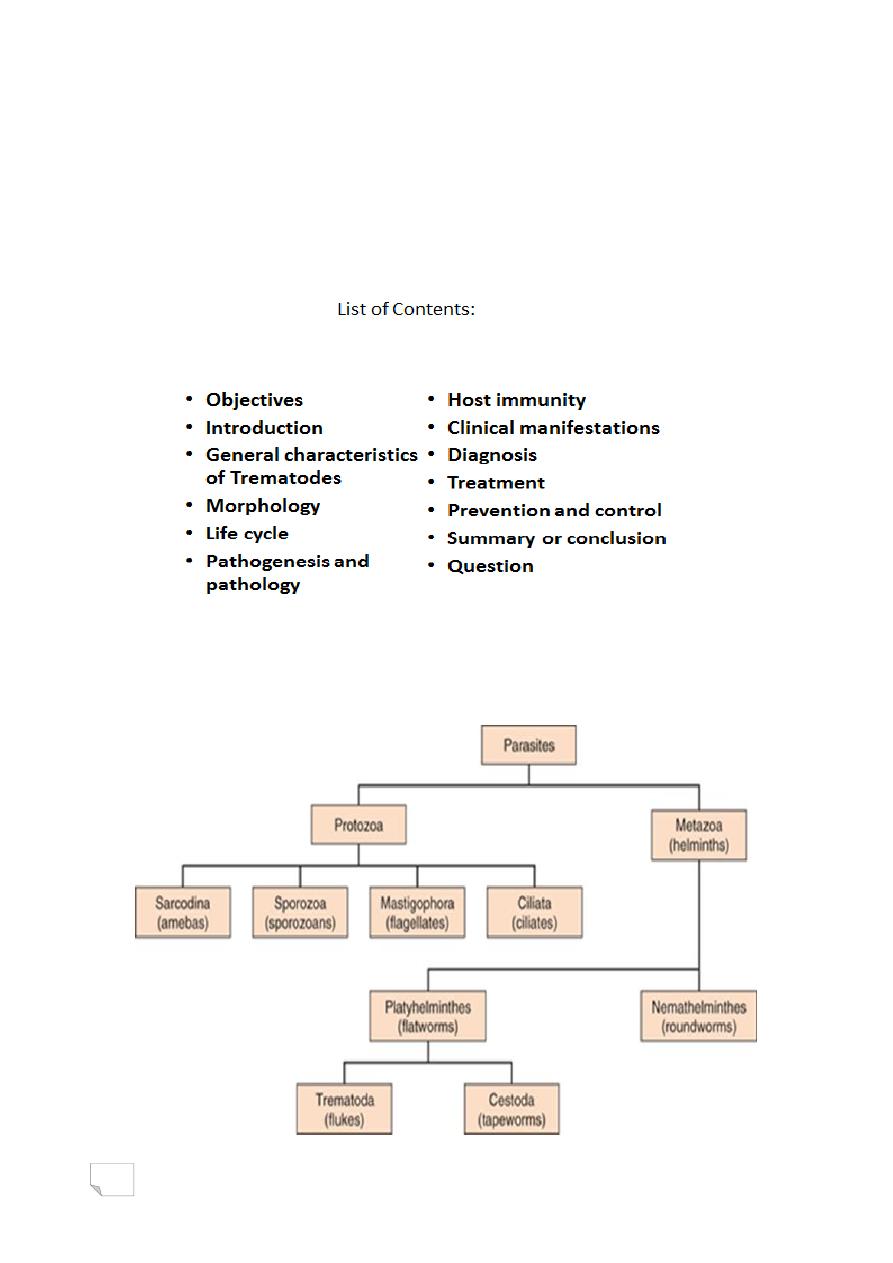
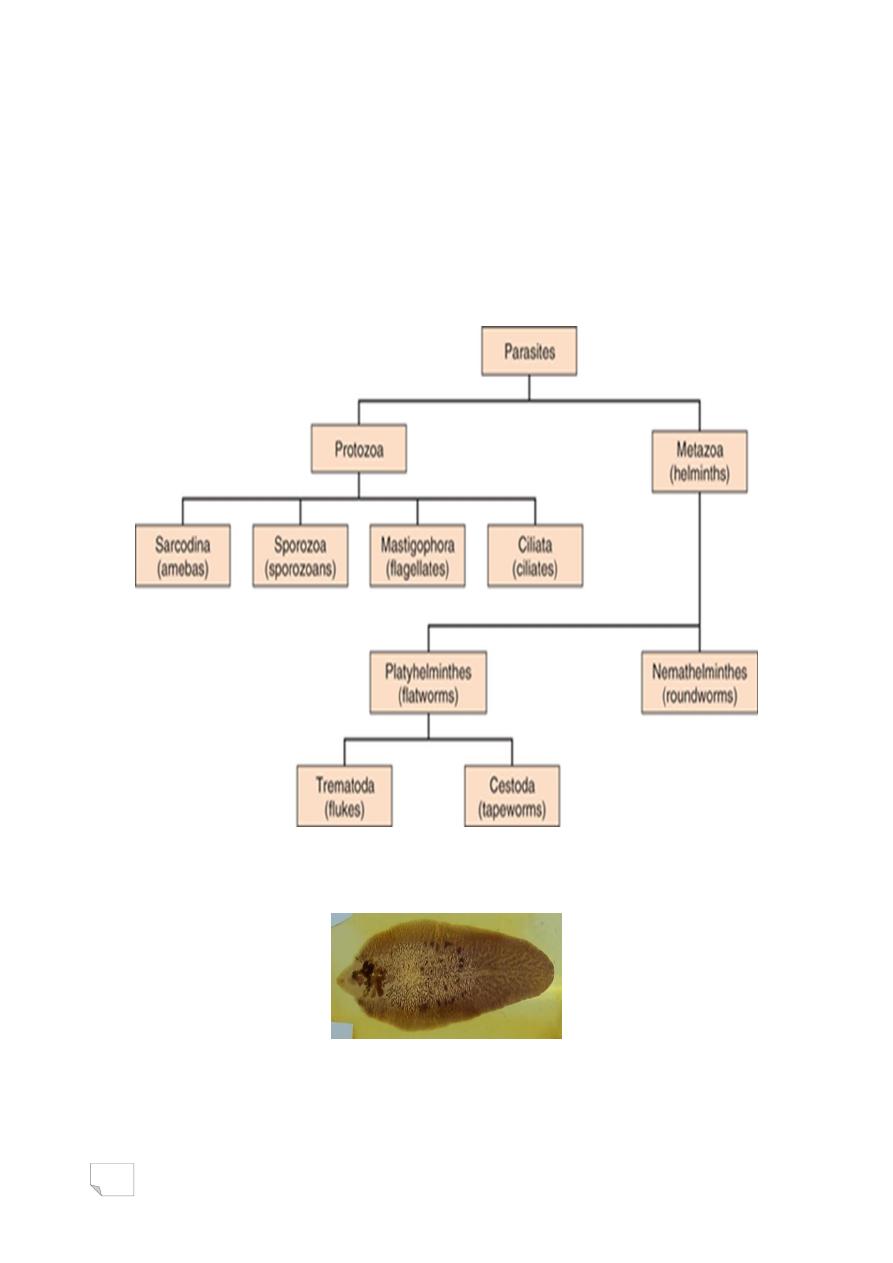
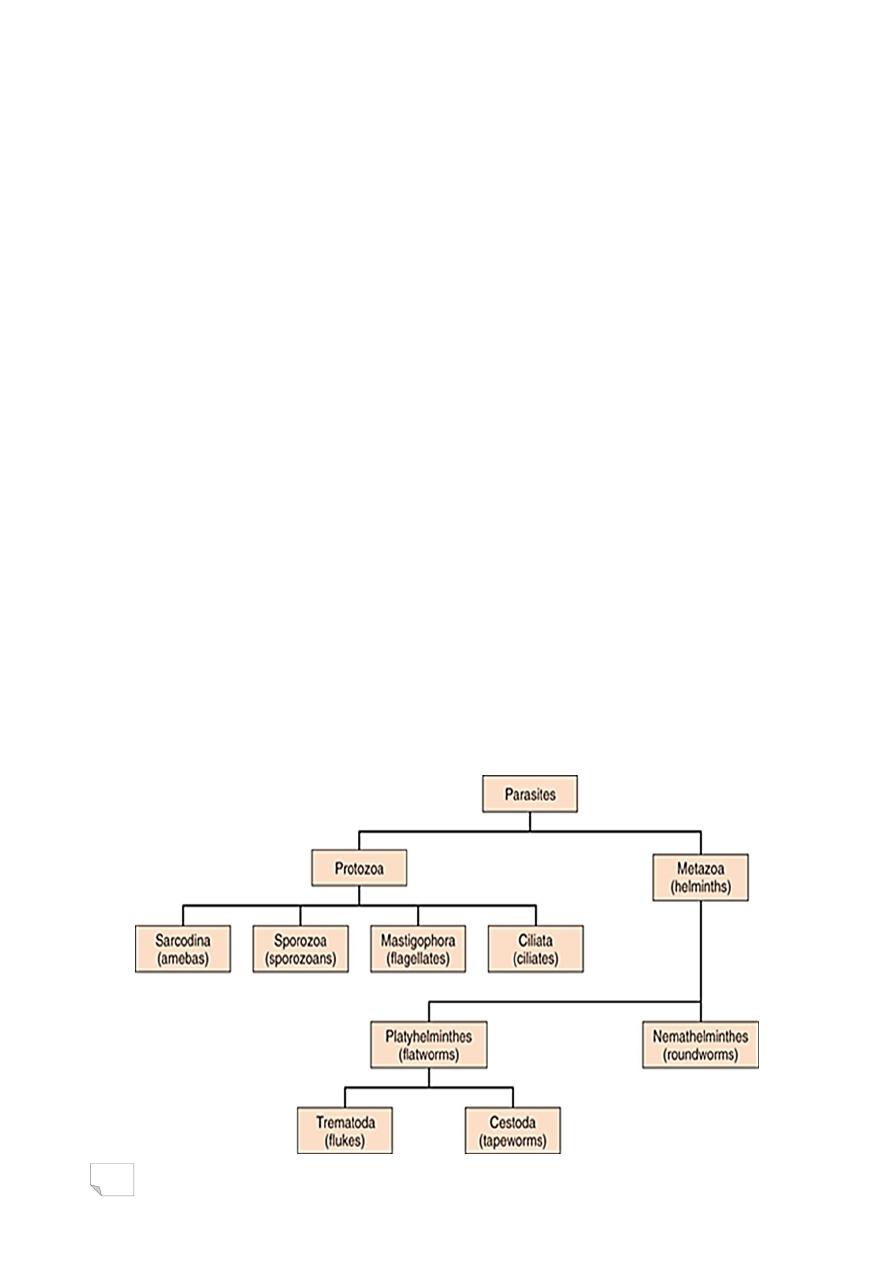
Helminthes are broadly classified into:
Phylum: Platyhelminthes
Platyhelminthes or Flatworms (Platy=flat):
These include flukes and tape worms.
Phylum: Nemathelminthes
Nemathelminthes or Round worms
(Nemato=thread): These include nematodes.
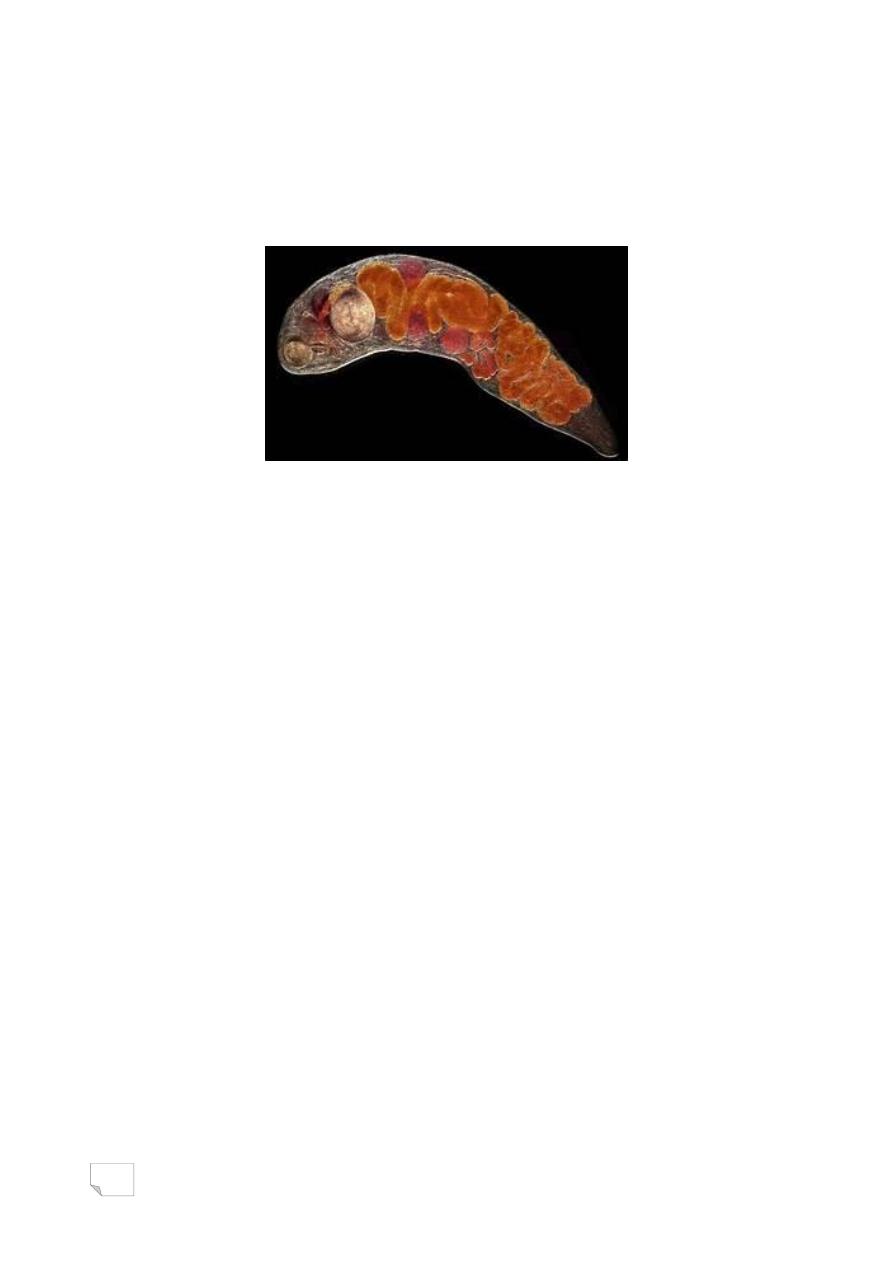
General characteristics of Trematodes
1. They are leaf-shaped, unsegmented worms and flattened
dorsoventrally.
2. They vary in size.
3
3. They have two suckers the organs of attachment. Oral
sucker and ventral sucker.
4. Alimentary canal is present but incomplete, including a
mouth but the anus is absent.
General characteristics of Trematodes
5. The body surface is covered with integument
(plasma membrane).
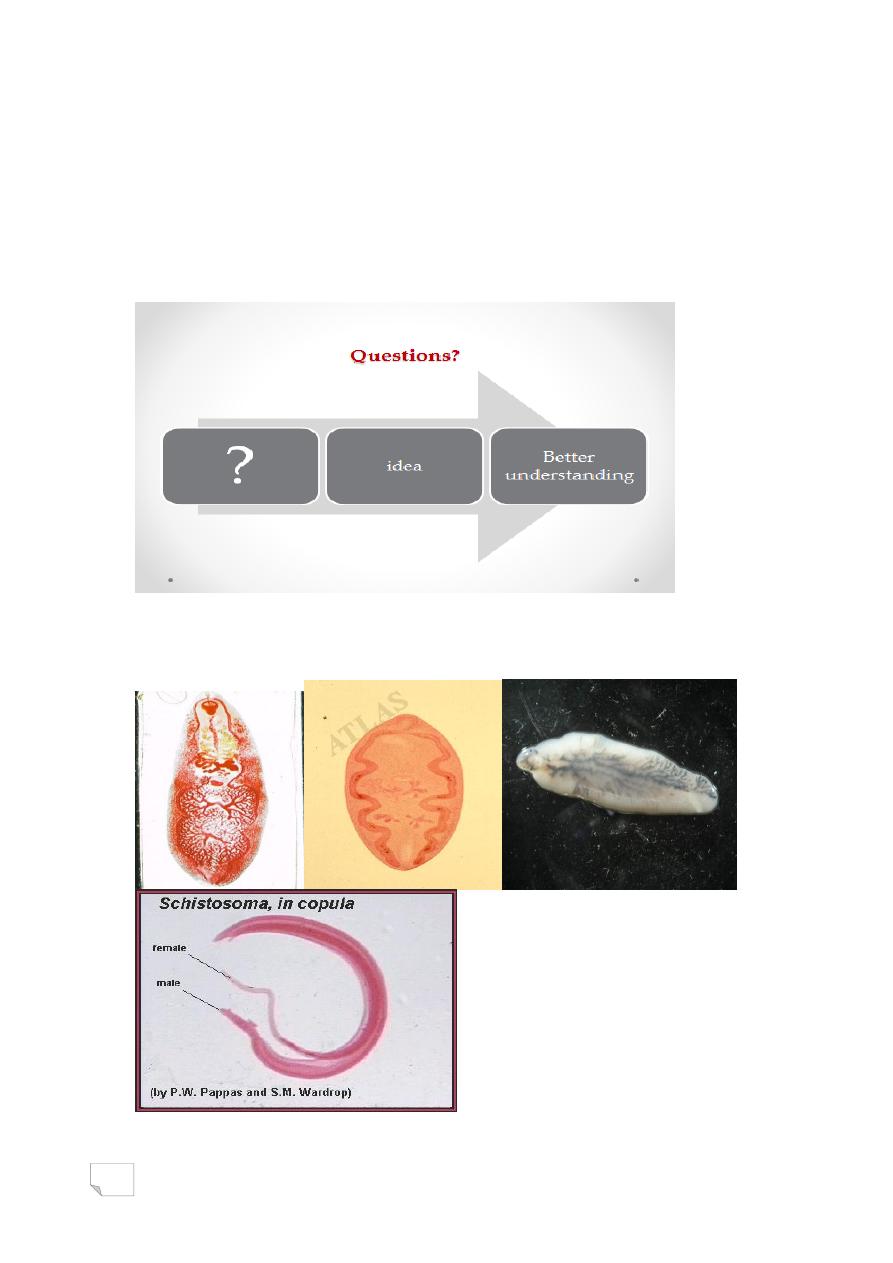
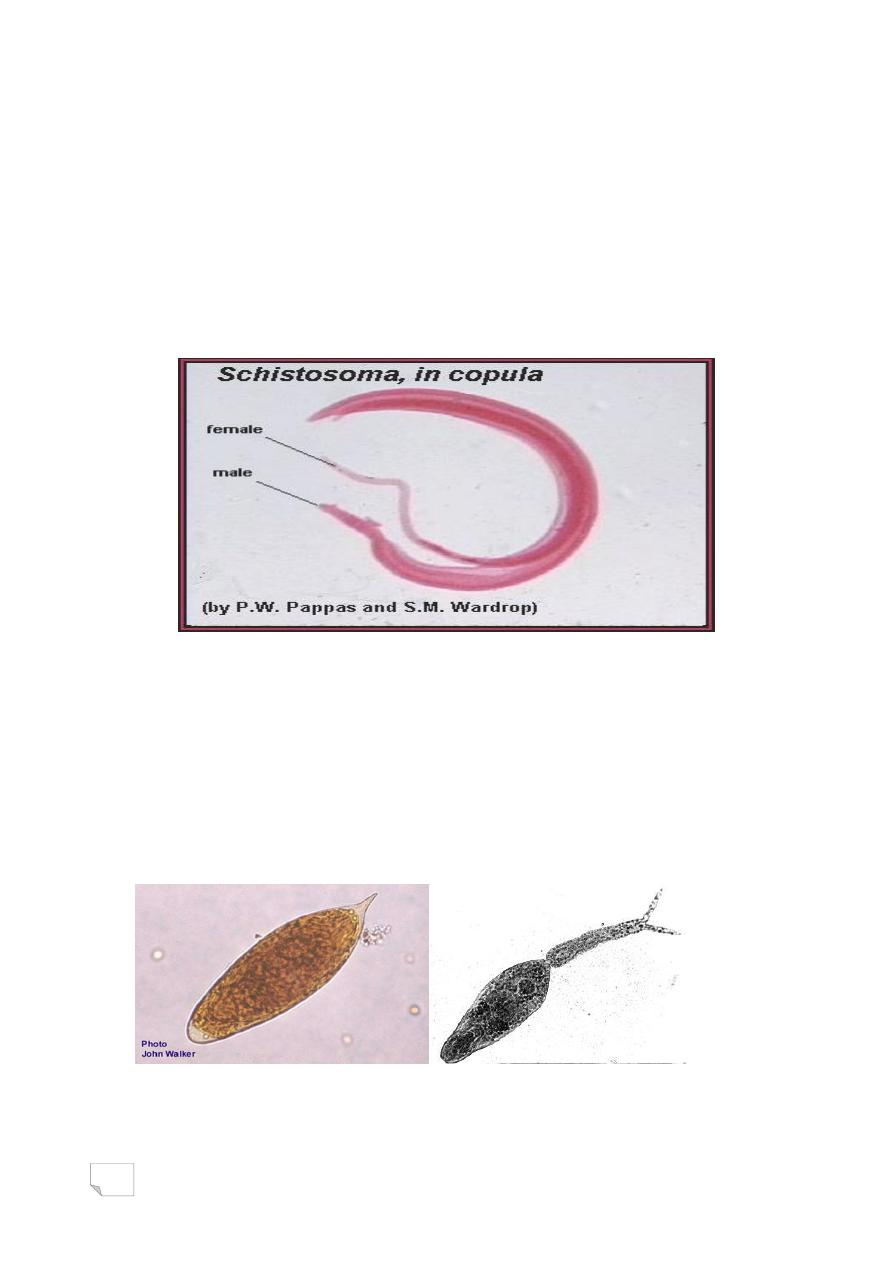
6. They are hermaphrodite. Sexes are not separate,
except Schistosomes are unisexual.
7. The eggs are all operculated except
those of schistosomes.
Morphology
Adult, larva and egg
These are the important morphological forms of the
helminthes.
Adult
Most adult worms are macroscopic in size and often visible
to the naked eye.
Morphology
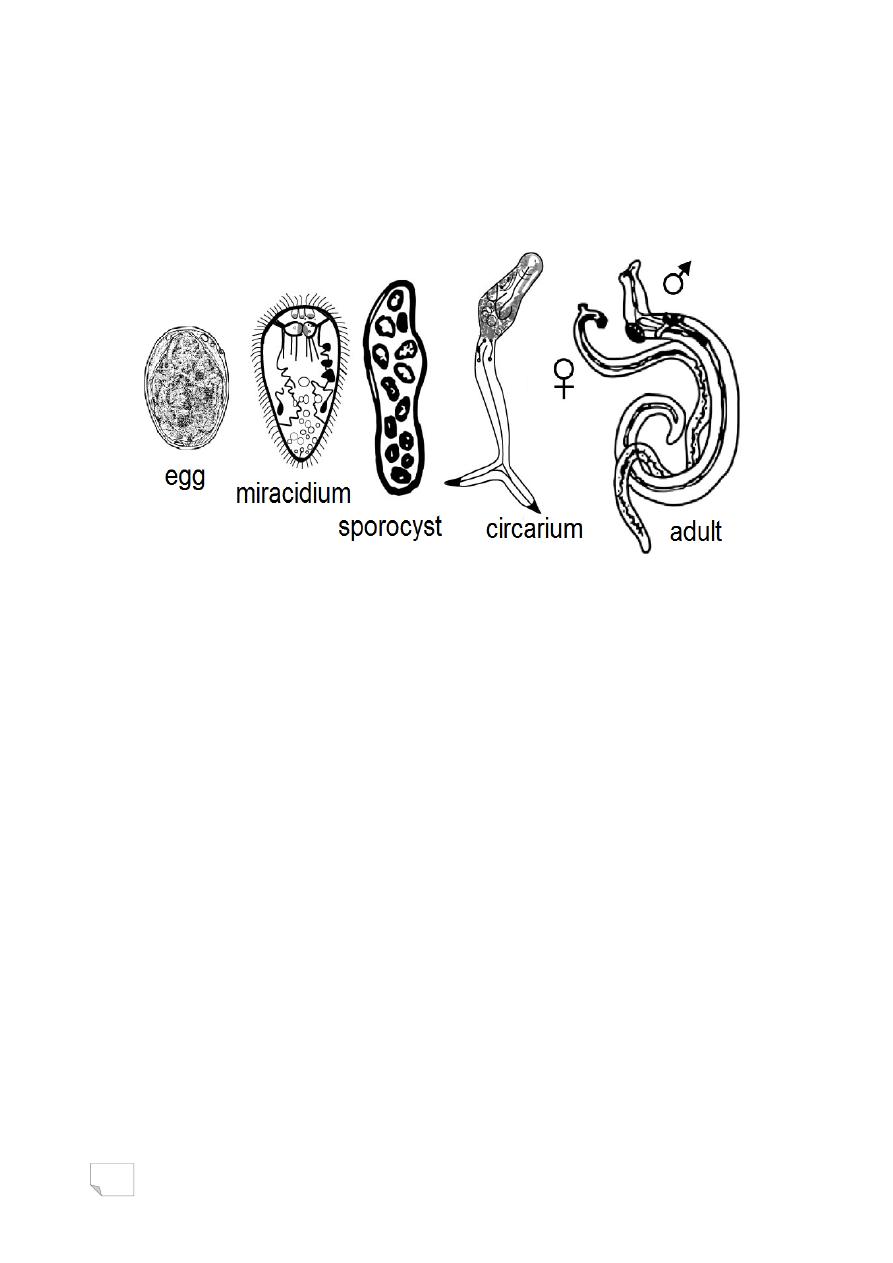
Larva: various larval forms of helminthes found in man and
other hosts. These are:
Miracidium, sporocyst, redia, cercaria and metacercaria in
trematodes.
4
Egg
All the helminthes with a few exceptions produce eggs. These
are excreted out in different excretions or secretions
of the body.
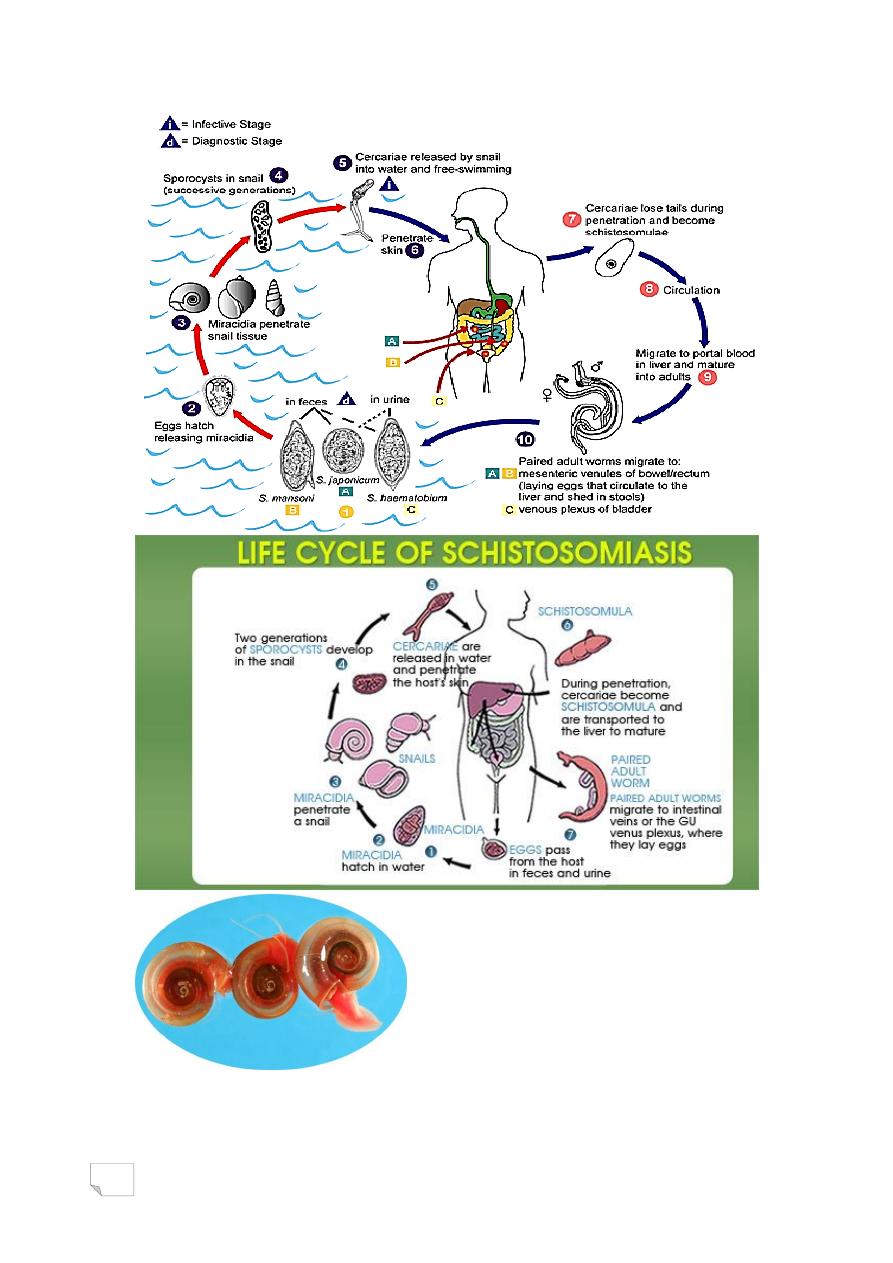
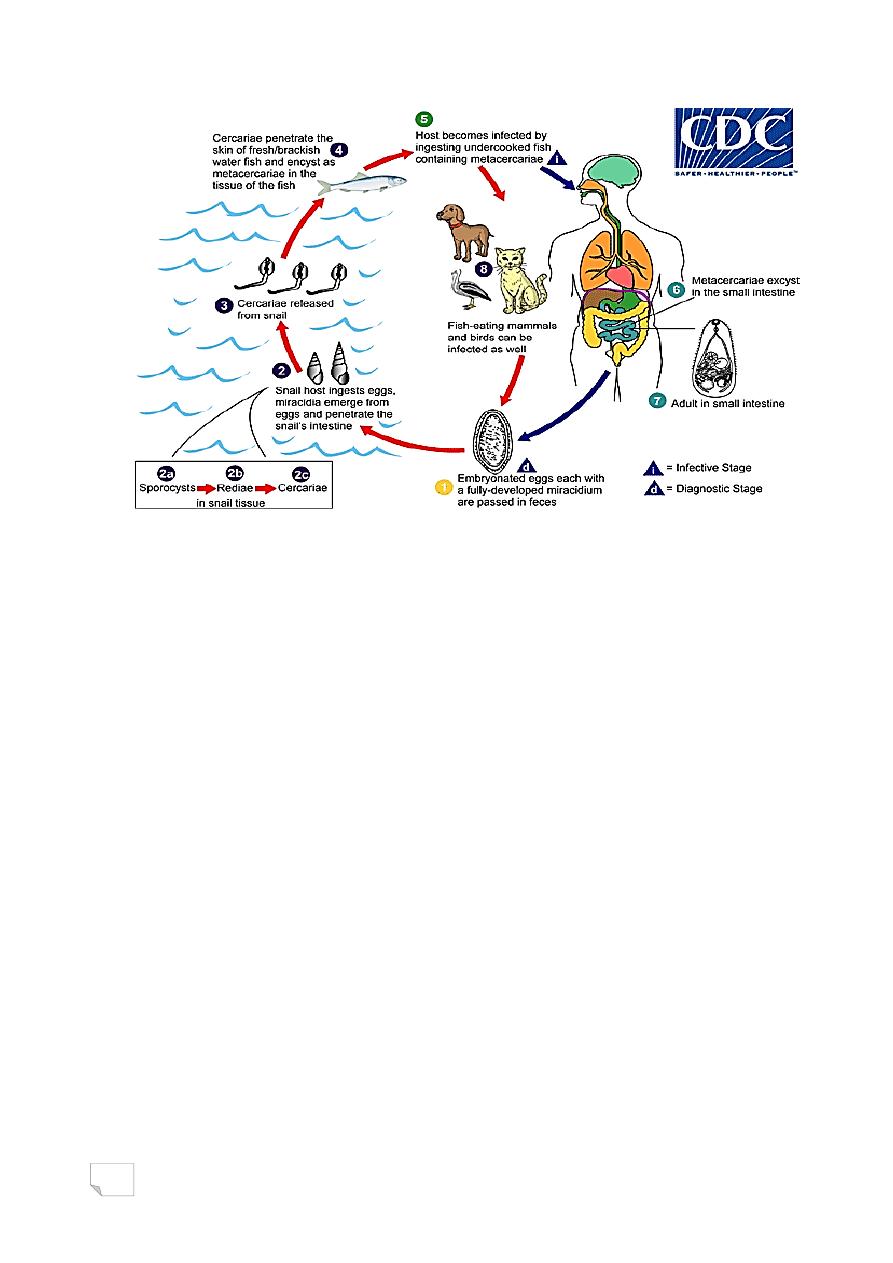
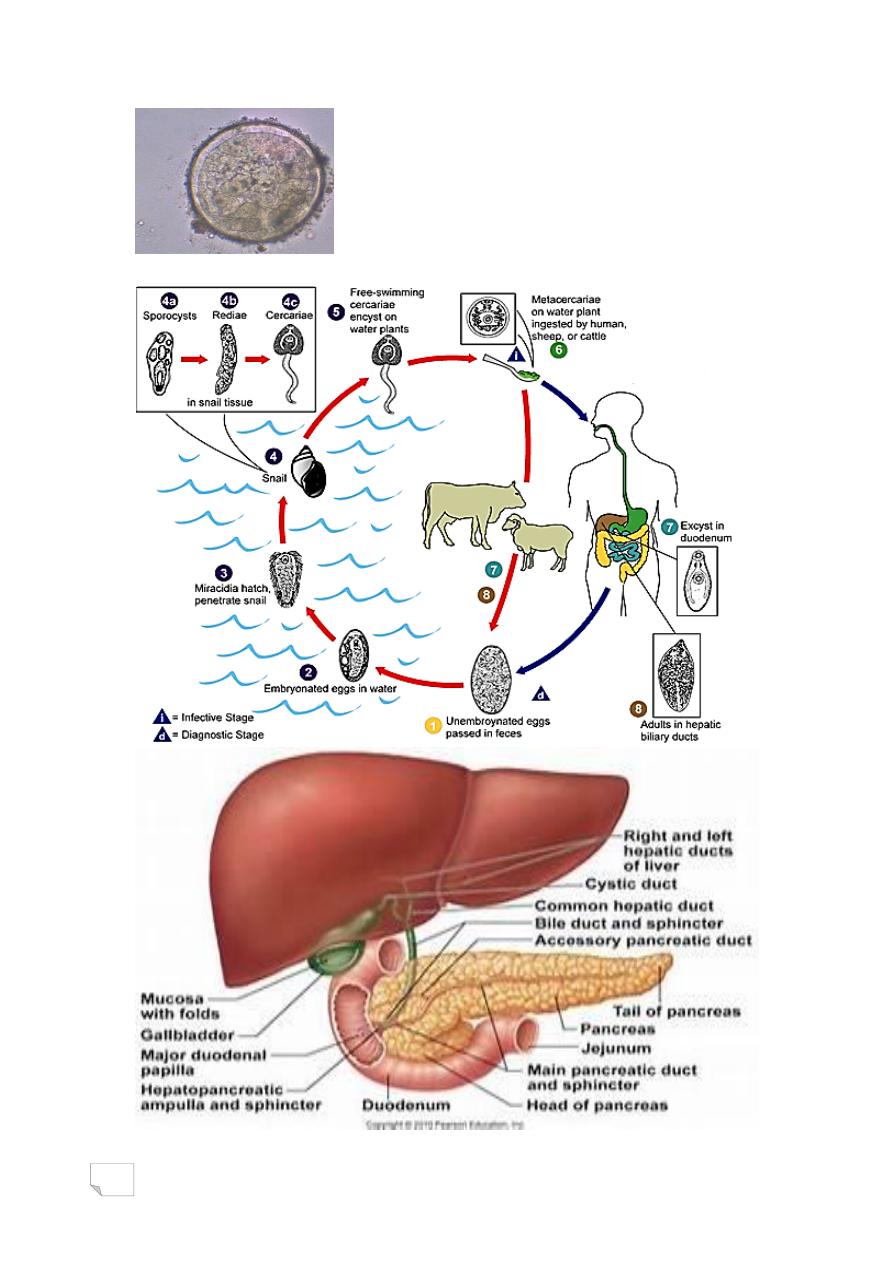
Life cycle:
Trematodes complete their life cycles in two different hosts.
Man always is the definitive host. Fresh water snail or mollusc
is the first intermediate host and the fish or crab is the second
intermediate host.
Pathogenesis and pathology
The pathological lesions in helminthic diseases are mainly due
to:
Direct damage caused by helminthes
Indirect damage from host response
Host immunity
The host resistance in helminthic infections involves a complex
interaction of:
• Non-specific factors
• Cellular immunity
• Humoral immunity

5
Host immunity
The helminthes escape from defence mechanisms of the host immunity,
occur in many ways. These are
a) antigenic variation
b) masked antigens
c) shared host antigens.
Clinical manifestations
Clinical manifestations of helminthic diseases are variable. These may be
acute or chronic. The onset of the disease may be sudden or slow.
Allergic symptoms are important. eg., Wuchereria in the lymphatics
produce a variety of allergic manifestations such as filarial fever,
lymphangitis.
Diagnosis
The clinical diagnosis of helminthic infections is frequently difficult.
The laboratory diagnosis is important. This plays an important role in
establishing the specific diagnosis of helminthic diseases and is usually
based on the morphological recognition of helminthes.
Treatment
Chemotherapy is the method of choice for treatment of helminthic
diseases. Surgery is indicated in few helminthic infections.
Prevention and control
These consist of:
1. Chemotherapy and isolation
2. Control of infection in animal reservoir
3. Personal prophylaxis
Summary or Conclusion:
• The helminthes are multicellular and bilaterally symmetrical
elongated, flat.
• They vary in size.
6
• all other flukes are hermaphrodites.
• Body surface of trematodes is covered with integument (plasma
membrane), .
• Adult, larva and egg are the important morphological forms of the
helminthes.
• The life cycle of a parasite may be simple or complex.
Genus: Schistosoma
Class: Trematoda

7
List of Contents:
› Objectives
› Introduction
› Schistosoma haematobium
i.
Morphology & Life cycle
ii.
Pathogenesis and pathology & Clinical manifestaion
iii.
Reservoir, source and transmission of infection
iv.
Laboratory diagnosis
› Schistosoma mansoni
› Schistosoma japonicum
› Summary or conclusion
› Question
Objectives:
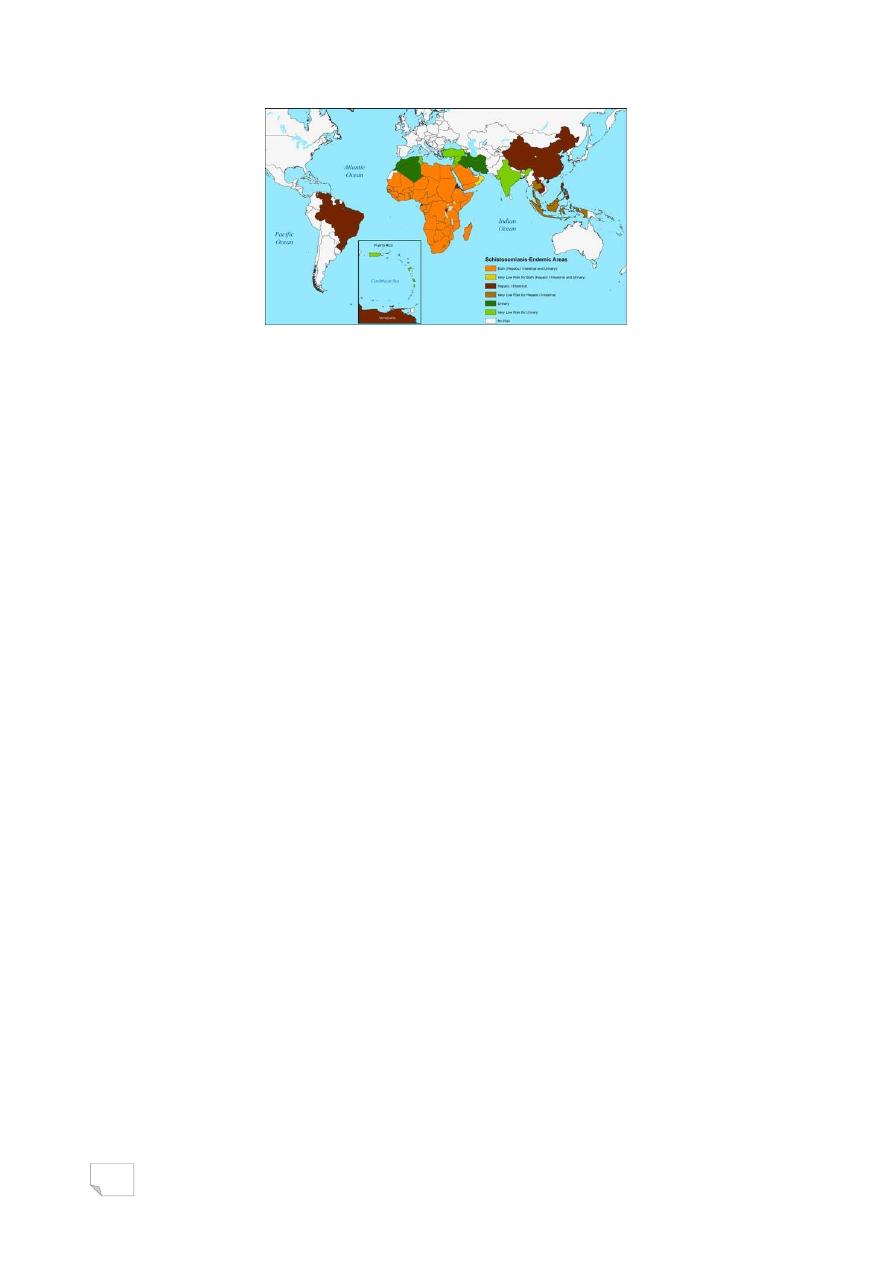
WHO reports show that, 250 million people are infected in the world.
Learn students:
› General characteristics of Schistosoma sp.
› Common name and habitat of Schistosoma sp.
› Infective stage and diagnostic stage
› How is transmit to human.
› The disease and diagnosis.
› Pathogenesity of Schistosoma sp.
8
Introduction
Class: Trematoda
Trematodes also called flukes causing a variety of infections in humans.
can be classified in the following ways:
1. Systematic classification.
2. Classification according to the habitat. flukes can be classified as:
blood flukes, liver flukes, lung flukes and intestinal flukes.
Introduction
Genus: Schistosoma
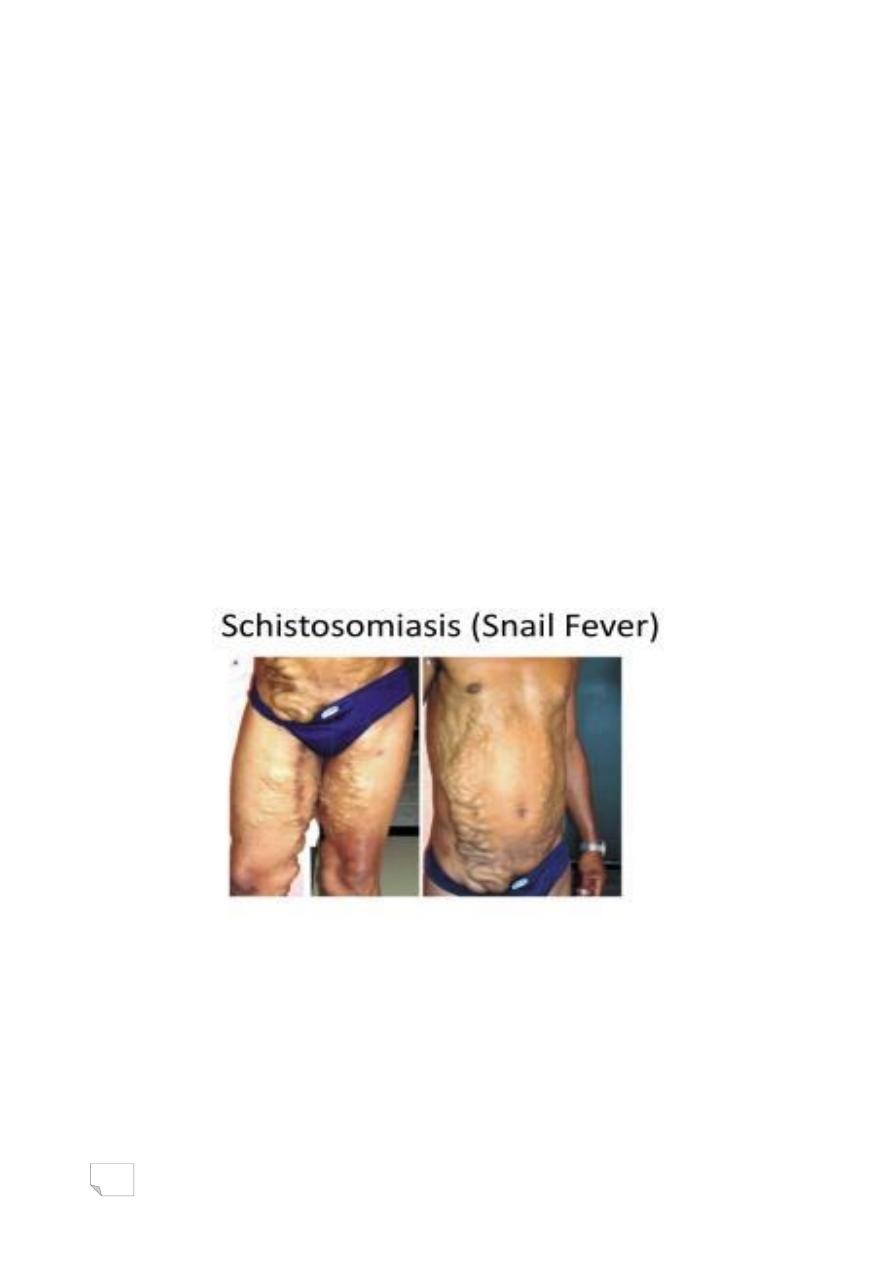
Schistosomes are known blood flukes because they live in the
vascular system of humans and other vertebrates. They cause
schistosomiasis.
Schistosoma haematobium
Schistosoma mansoni
Schistosoma japonicum
Schistosoma haematobium
(Bilharz, 1852) Weinland,1858
Schistosoma haematobium is the major blood fluke which parasitizes
man. It is causative agent of vesical or urinary schistosomiasis.
Male and female flukes are found together in the venous
plexus of the venacava system that drains the urinary bladder,
pelvis and ureter.
9
Morphology
Morphologically, the males and females are similar to those of
other human schistosomes.
Adult worm
Sexes are separate. Body surface is covered with
integument. Male is short and stout. While the
female is longer and cylinder. A fertilized female can lay 20-200
terminal spine eggs/day.
Morphology
Adult worm (male and female)
Morphology
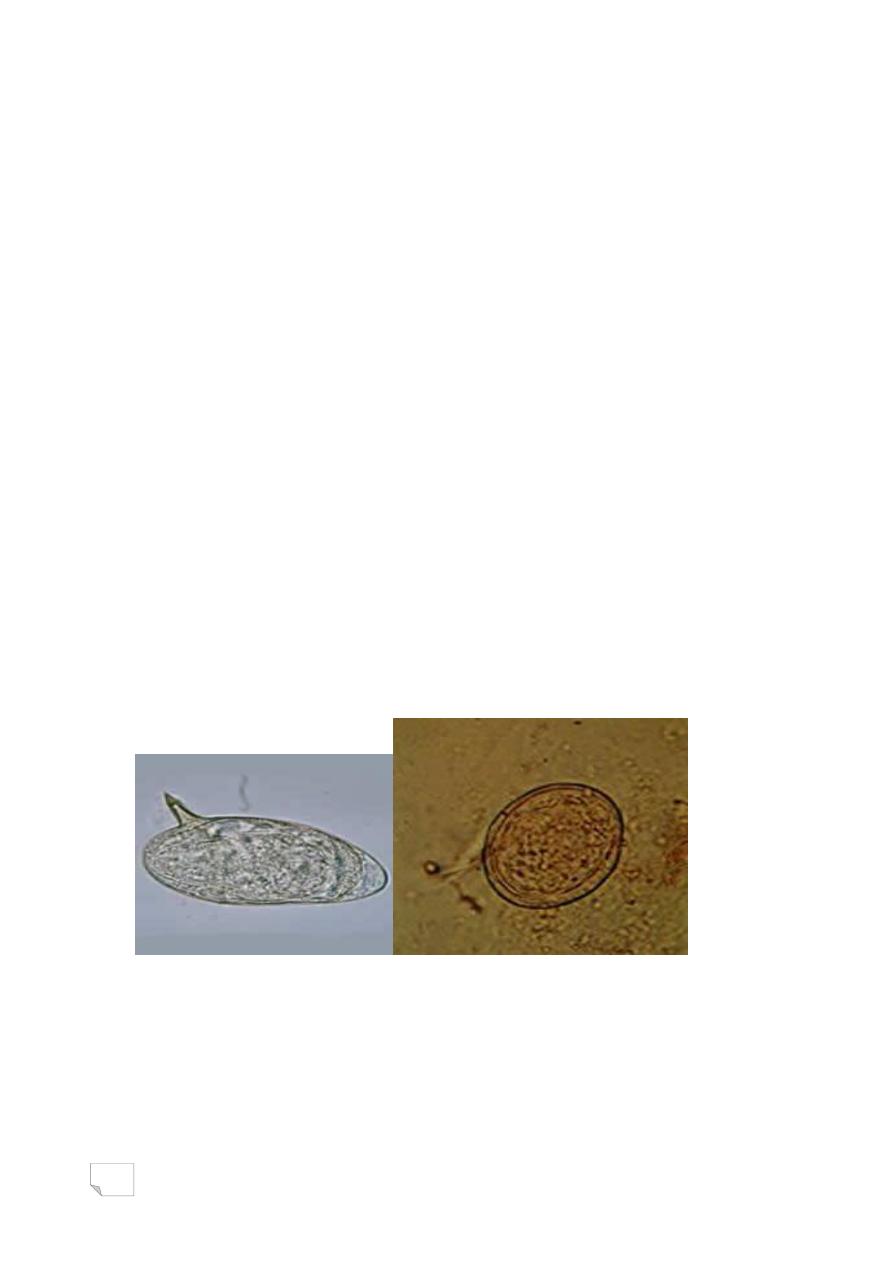
The eggs are elongated, oval-shaped, yellowish brown and
non-operculated. The presence of a terminal spine at the
posterior end is identifying feature of the egg.
Infective stage (Cercaria): It has an elongated oval
body, bifurcated elongated tail and two suckers.
Morphology
Egg of Infective stage (Cercaria) Schistosoma
haematobium
10
11
PATHOGENESIS AND PATHOLOGY
Cercariae and eggs of S. haematobium are pathogenic. Adult worms
are rarely pathogenic.
Pathogenicity due to cercariae
Invasion of the skin by cercariae produce an allergic
dermatitis at the site of penetration.
PATHOGENESIS AND PATHOLOGY
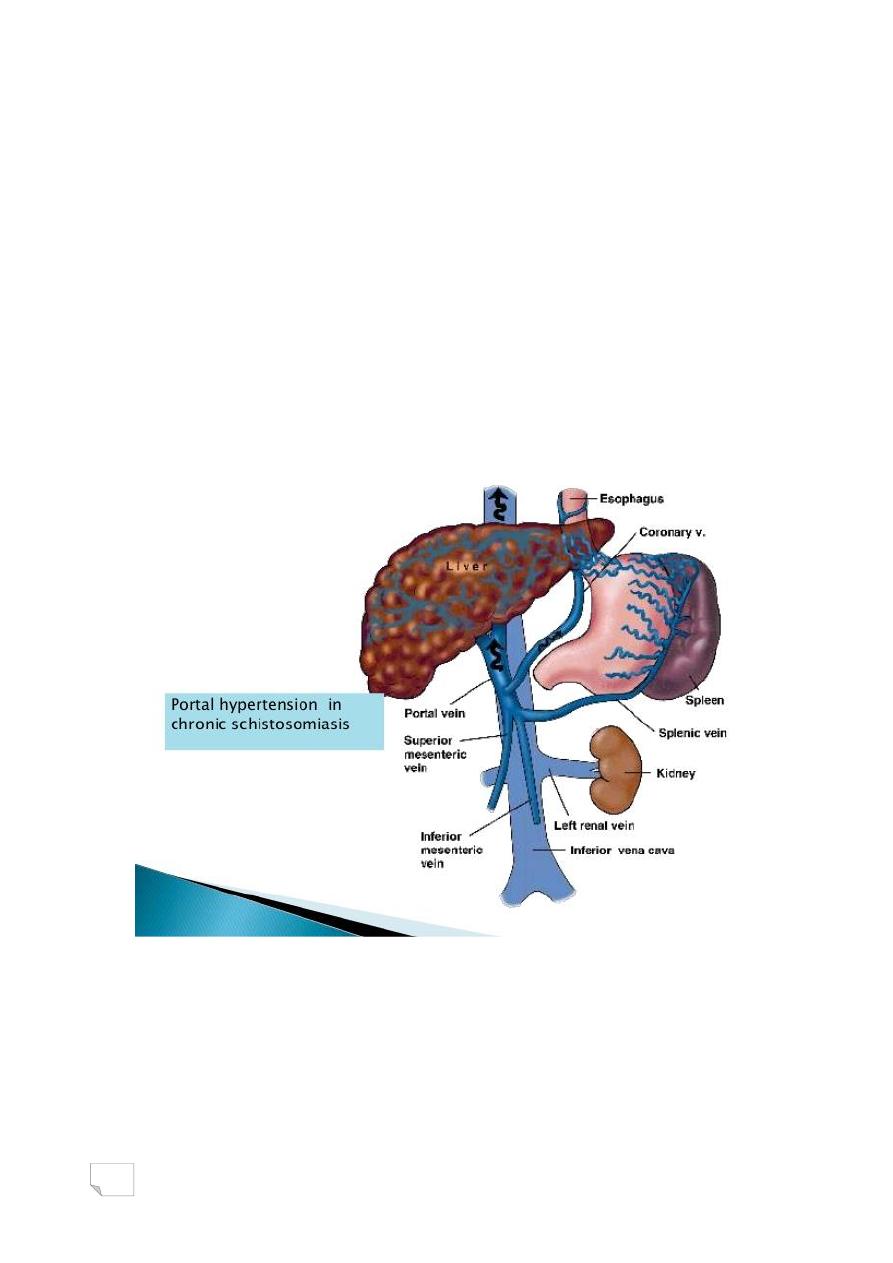
Pathogenicity due to eggs
Most of the morbidity and mortality associated with schistosomiasis
are caused by the eggs. Eggs induce a strong inflammatory and
granulomatous reaction leading to the development of granulomas. Egg
granulomas are found in the ureter and in the urinary bladder.
PATHOGENESIS AND PATHOLOGY
The eggs during their passage from venules into the lumen of
urinary bladder cause traumatic lesions, thereby producing
haemorrhage.
Continuous toxic and mechanical irritation of the eggs in the tissues
are an important factors for the development of malignant tumorous
condition in the urinary bladder.
12
CLINICAL MANIFESTATION
Vesical or urinary schistosomiasis is of two types: acute
schistosomiasis and chronic schistosomiasis.
Acute schistosomiasis
The condition is characterized by cercarial dermatitis, itching and
pruritic papular lesion in the skin within 24 hrs. of invasion by the
cercariae.
CLINICAL MANIFESTATION
Chronic schistosomiasis
The condition is characterized by haematuria, dysuria and frequent
urination are the main clinical symptoms.
Hydroureter, hydronephrosis, secondary microbial infections and
uraemia are the main complications of the disease. These can lead to
renal failure.
Reservoir, source and transmission of infection
Human is the important reservoir. Urine from infected Human is the
main source of infection to the snails. Human acquires infection through
skin, by penetration of the cercariae, on coming
in contact with contaminated water.

13
Reservoir, source and transmission of infection
S. haematobium infection occurs much frequently in:
1. Children and young adults between the age of 5-25 years.
2. Labourers working in the irrigated fields.
3. Fisher men working in fish culture ponds and rivers.
4. Women who wash utensils or clothes along the banks of canal or river.
LABORATORY DIAGNOSIS
Specific diagnosis is made by the microscopic demonstration of
eggs in urine specimens.
Urine is examined microscopically after concentration by
centrifugation or membrane filtration.
Urine egg count in a 24-hour collection is done to quantitate the
severity of the infection.
Egg viability test is carried out to assess the effectiveness of treatment.
The test is performed by mixing urine with distilled water and observing
for hatching miracidia.
LABORATORY DIAGNOSIS
Serodiagnosis: Detection of antibodies
Demonstrate specific circulating antibodies in the serum, by IHA, ELISA
and radio-immuno assay (RIA).
Disadvantages of the antibody-based tests are
Can not differentiate between active and past infection
Can not quantify egg burden.
LABORATORY DIAGNOSIS
Detection of antigens: in the serum and urine by ELISA and RIA.
This helps to detect acute infection and differentiate it from the past
infection.
Imaging methods: X-ray of the abdomen may show bladder and ureteral
calcifications. Ultrasound may show hydroureter, hydronephrosis and
obstructive nephropathy.
14
Schistosoma mansoni
Sambon,1907
Known as Manson's blood fluke, which produces intestinal
schistosomiasis or bilharziasis in humans.
Reside together in mesenteric venules of large intestine.
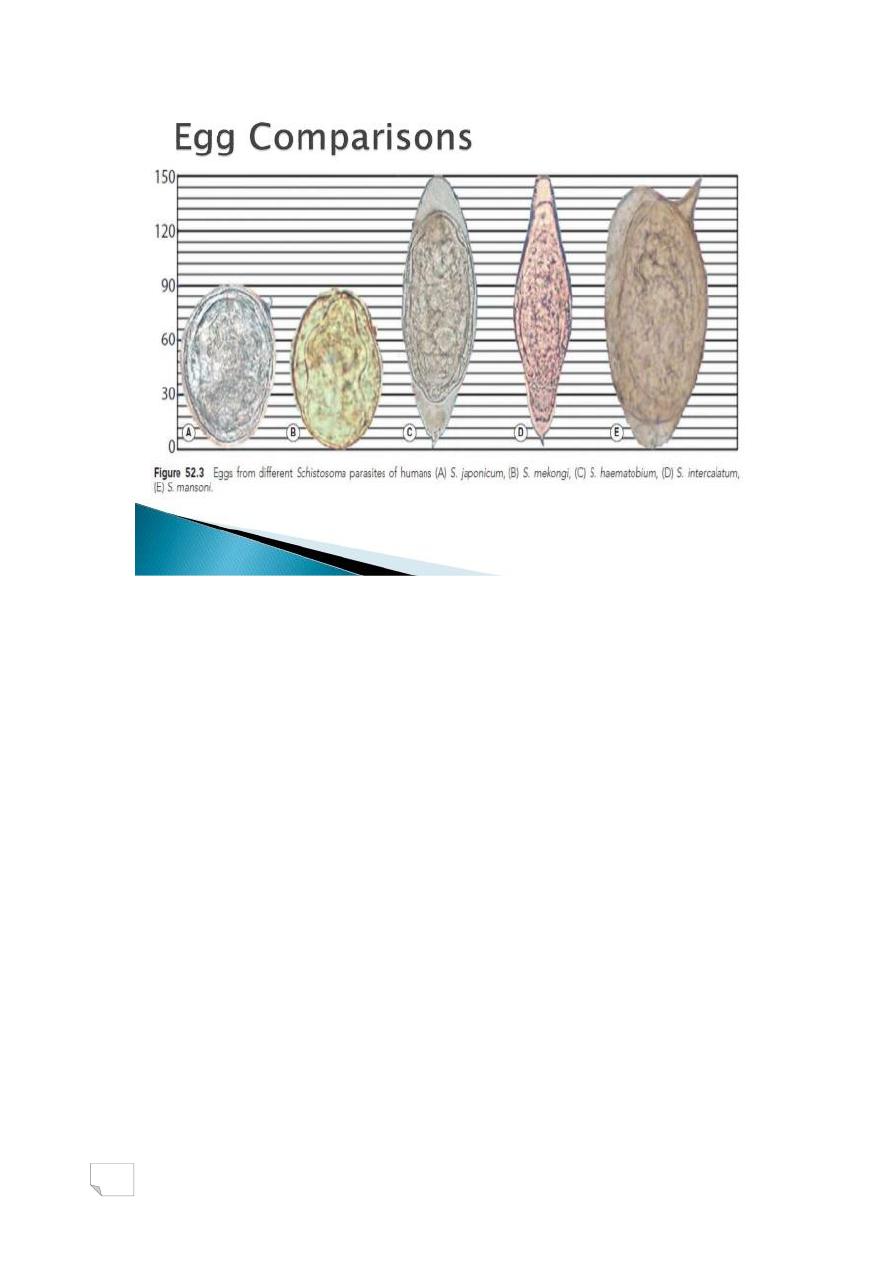
Eggs are oval, non-operculated and yellowish brown. have a
characteristic sharp lateral spine.
Life cycle of S. mansoni, It differs in the type of intermediate hosts,
and habitat of the fluke.
Schistosoma japonicum
Katsurada, 1904
known as japonica's blood fluke, which causes Oriental
schistosomiasis in human.
Found in the mesenteric venules of the small intestine.
Egg is subspherical, non-operculated and yellowish brown. It has a
lateral small spine or rudimentary knob.
Life cycle of S. japonicum is similar to that of S.mansoni.
Schistosoma sp.
Egg of
Schistosoma mansoni Schistosoma japonicum
15
Summary or Conclusion:
Schistosoma sp. is a major parasitic caused of mortality and
morbidity, next to malaria. Due to eggs.
Schistosomes are known blood flukes because they live in the
vascular system of humans.
Sexes are separate.
Infective stage is cercaria, diagnostic stage is egg.
Cercariae produce an allergic dermatitis in the skin.
Human acquires infection through skin, by penetration of the
cercariae, on coming in contact with contaminated water.
16
17
د. رؤى طفيليات
81
\
2
\
2181
( عدد االوراق
2
) م
\
3
\
موصل
lec: 3
Intestinal flukes
Introduction
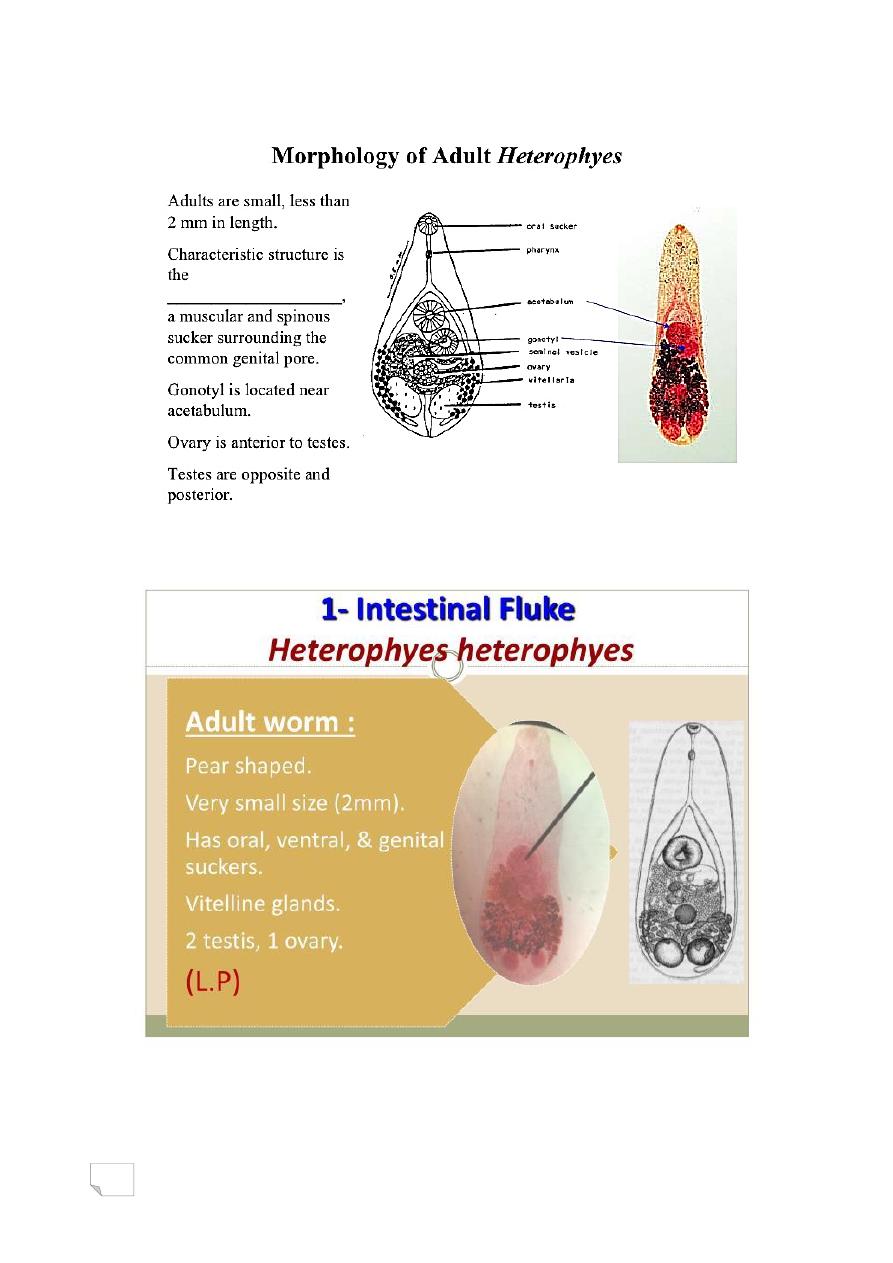
• Intestinal flukes (trematodes) are flat hermaphroditic worms that
vary in length from a few millimetres to many centimetres.
Approximately 70 species are known to colonise the human
intestine, but only a few species are known to cause actual
infection.
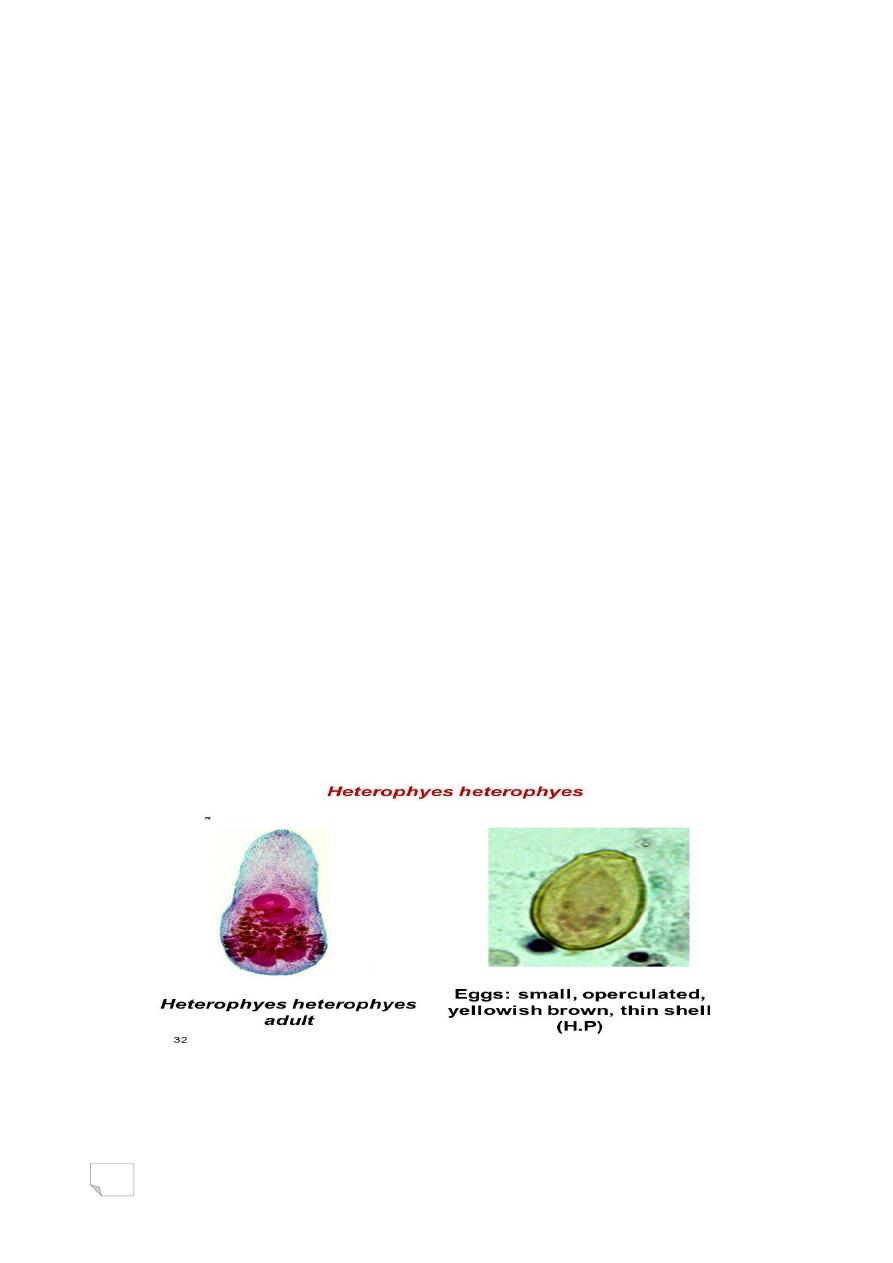
Hetrophyes hetrophyes
• The trematode Heterophyes heterophyes, a minute intestinal
fluke(Fish tape worm).
• Disease caused by Hetrophyes hetrophyes called: Hetrophyisiasis.
Heterophyes heterophyes
• Geographic Distribution
• Egypt, the Middle East, and Far East.
Heterophyes heterophyes
• Habitat:
• Small intestine of man, dog , cat & fox
18
19
Clinical presentation
• Symptoms of Heterophyiasis
• Asymptomatic
• Abdominal pain
• Diarrhea
• Intestinal hemorrhage
• Intestinal obstruction
• more symptoms...»
Diagnosis
• Laboratory Diagnosis
• The diagnosis is based on the microscopic identification of eggs in
the stool. However, the eggs are indistinguishable from those of
Metagonimus yokogawai and resemble those of Clonorchis and
Opisthorchis.
• Treatments for Heterophyiasis
• Praziquantel
• more treatments...(according to the severity of infection surgical
intervention may be needed).
Heterophyes heterophyes
• Prevention:
• Proper disposal of human sewage.
• Proper cooking and salting fish for many days.
• Not to eat undercooked fish.
20
د.رؤى طفيليات
22
\
2
\
2132
( عدد االوراق
2
) م
\
1
\
موصل
lec: 4+5
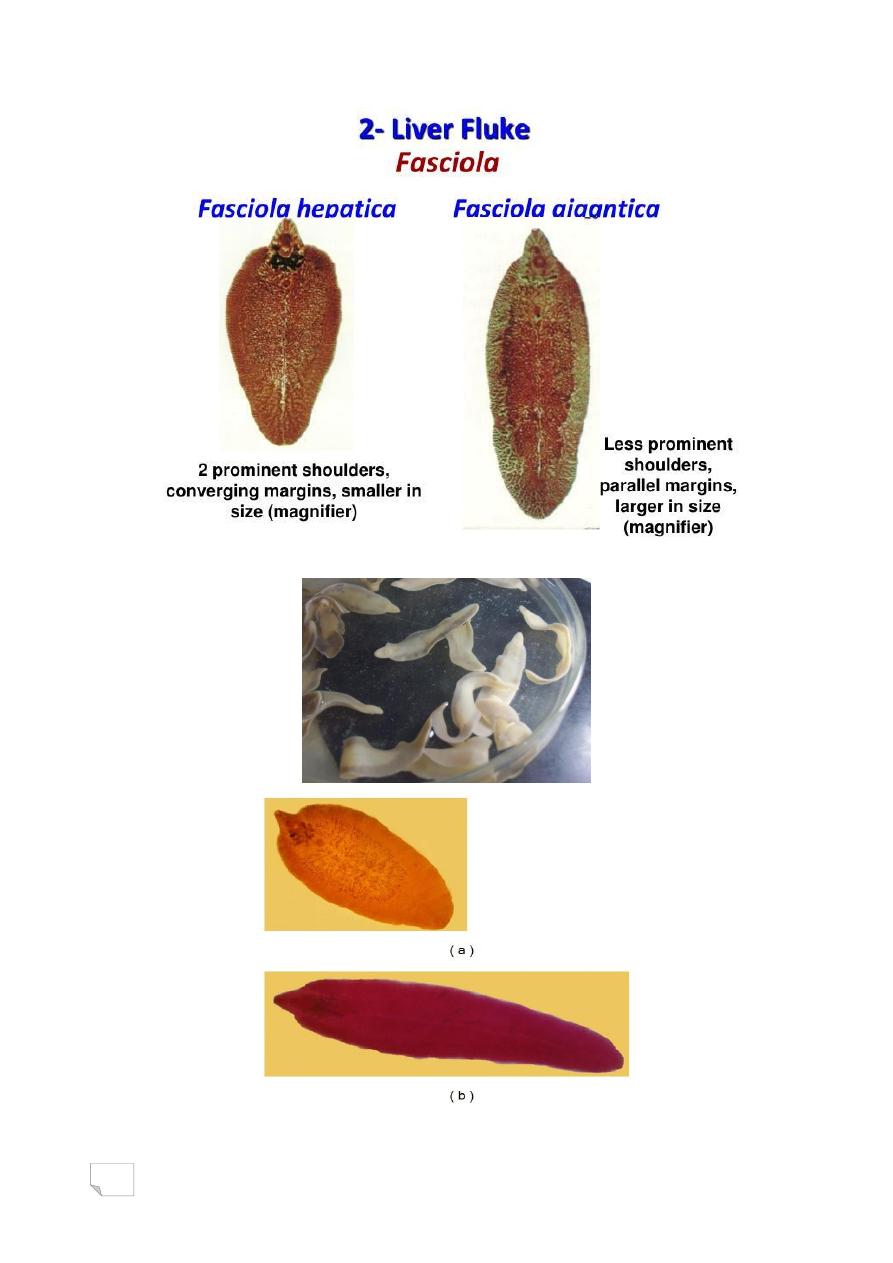
Liver fluke
• Fasciola hepatica.
• Fasciola gigantica.
•
Fasciola hepatica
Linnaeus, 1758
Lecture:
21
Objectives:
More than 2 million cases of human fascioliasis occur worldwide.
Learn students:
• General characteristics of Fasciola hepatica.
• Common name and habitat of Fasciola hepatica.
• Infective stage and diagnostic stage.
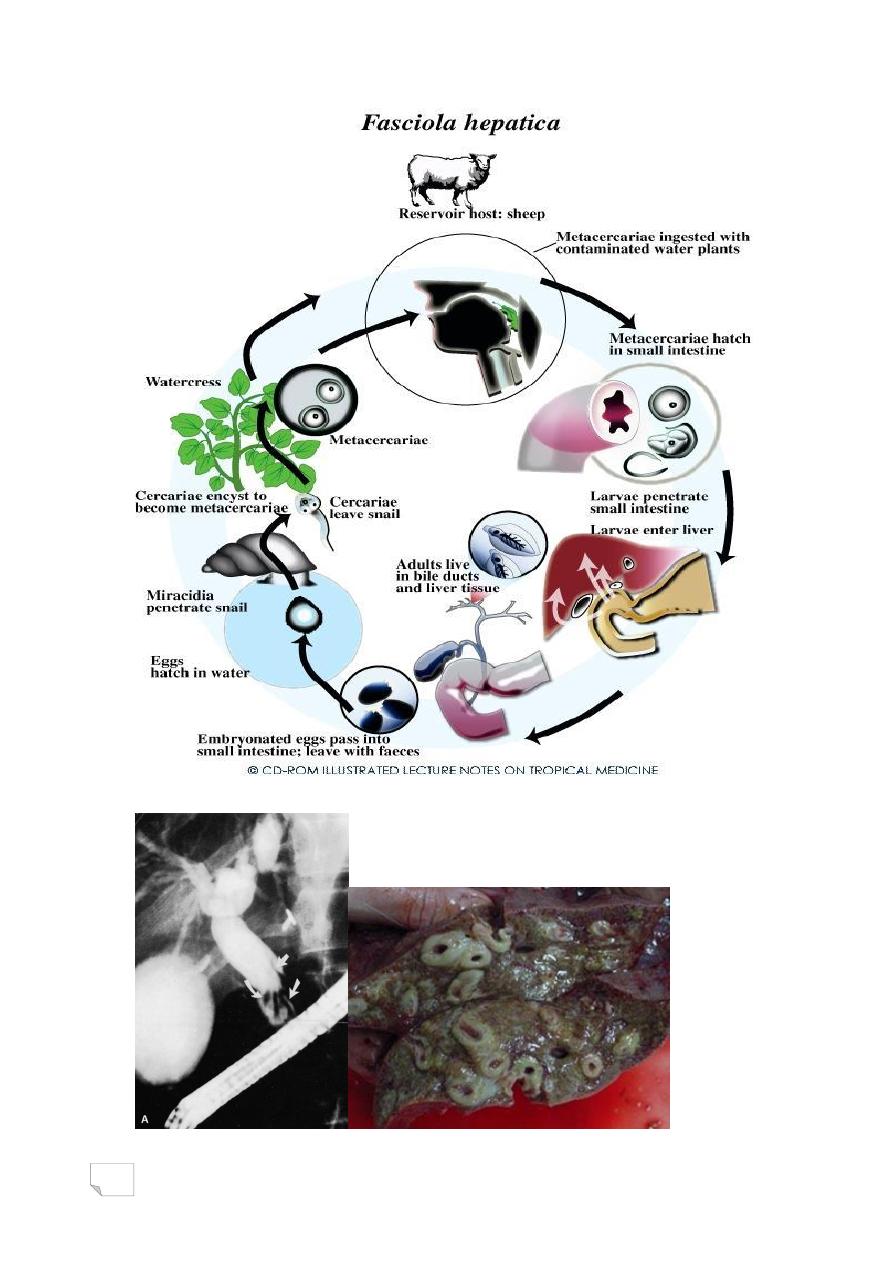
• Life cycle of Fasciola hepatica.
• Pathogenesity of Fasciola hepatica.
• How is transmit to human.
• The disease and diagnosis.
Introduction
Fasciola hepatica also called liver fluke,Causes human fascioliasis.
HABITAT
Adult flukes primarily live in the bile tract of infected domestic and
wild herbivorous animals and of humans.
MORPHOLOGY
Fasciola hepatica shows following features:
1. It is a large liver fluke.
2. It primarily infects liver of the sheep.
Humans are the incidental hosts.
22
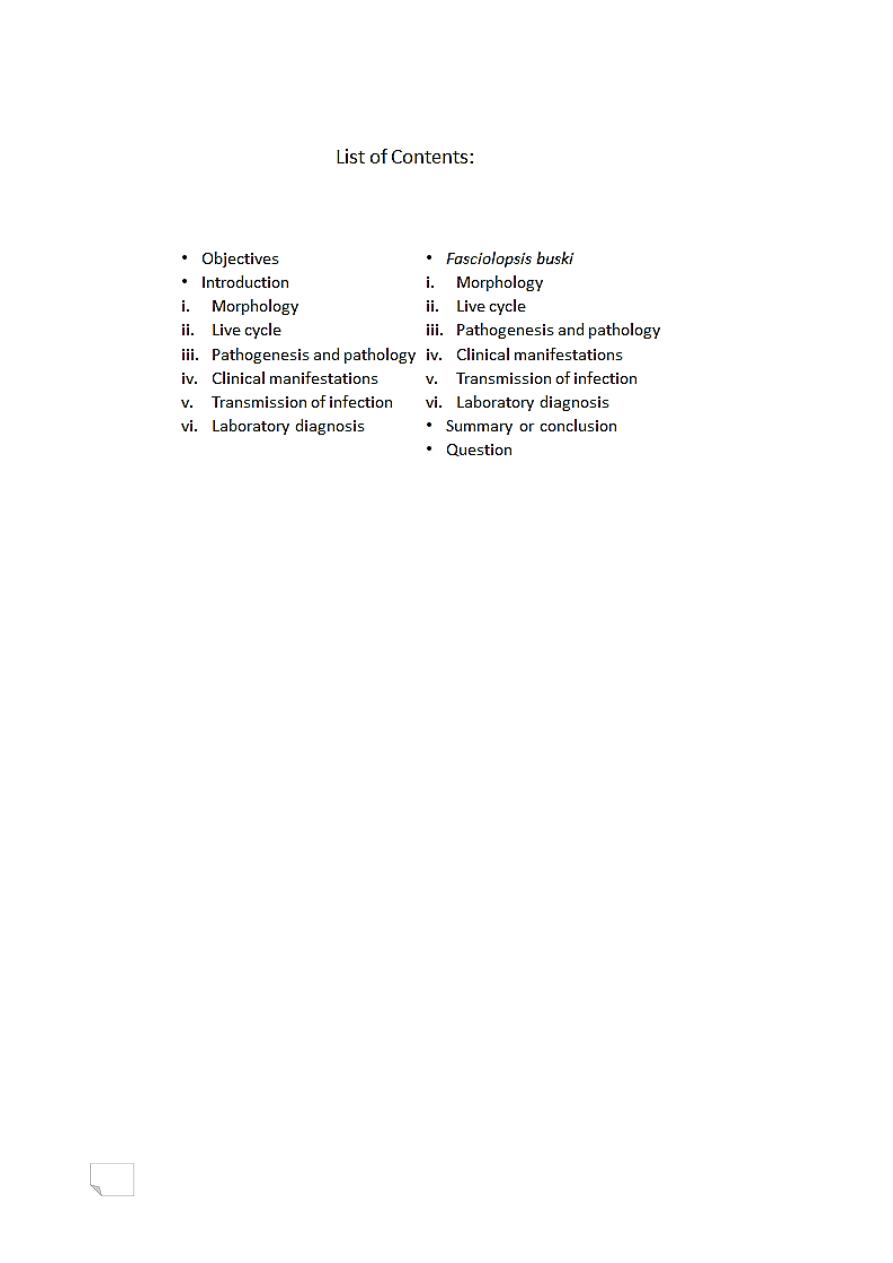
MORPHOLOGY
Adult worm
Relatively is large (measures 2.5-3cm length),flat and leaf-shaped, brown
coloured fluke.The anterior end shows a distinct conical projection while
the posterior end is rounded. It has two suckers, oral and ventral sucker.
The fluke is hermaphrodite.
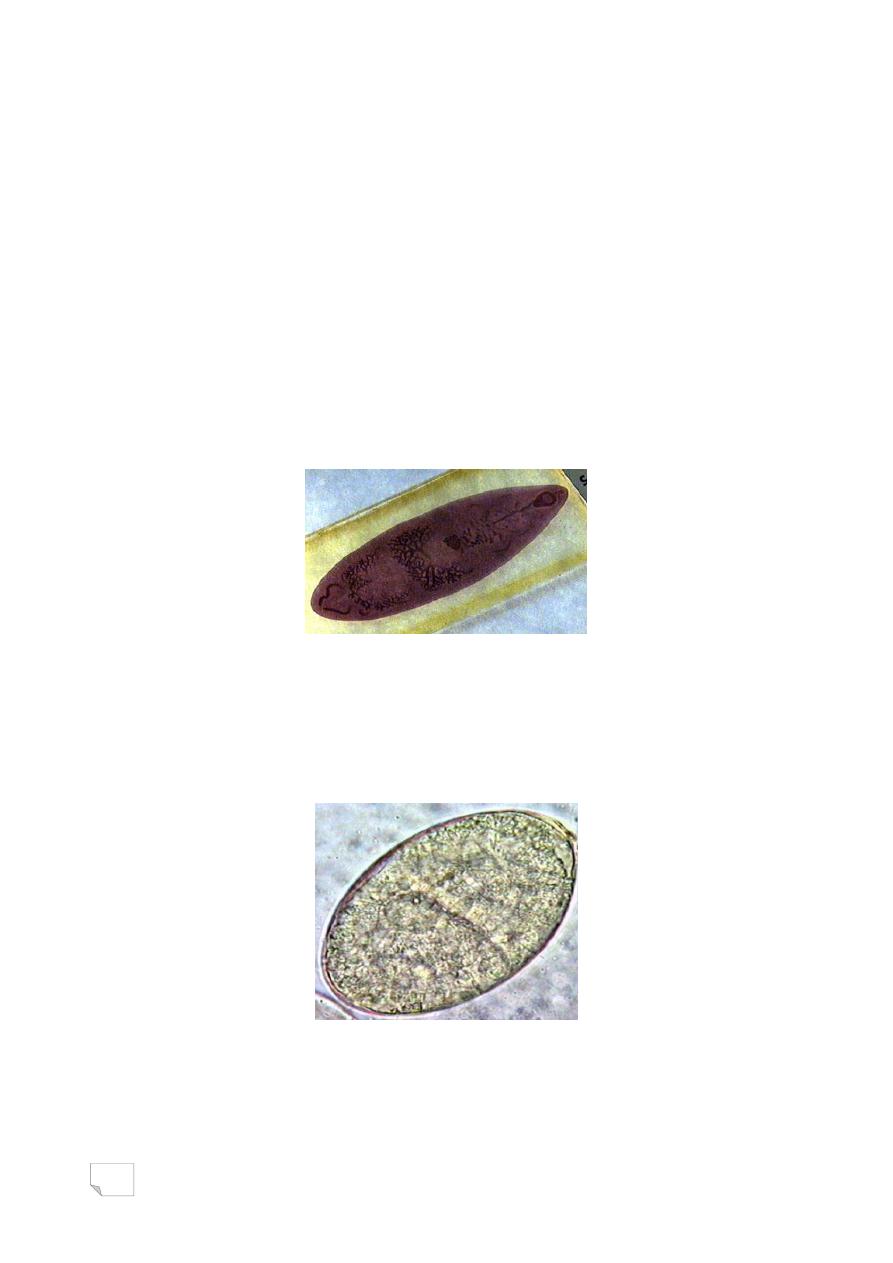
MORPHOLOGY
Adult worm Fasciola hepatica
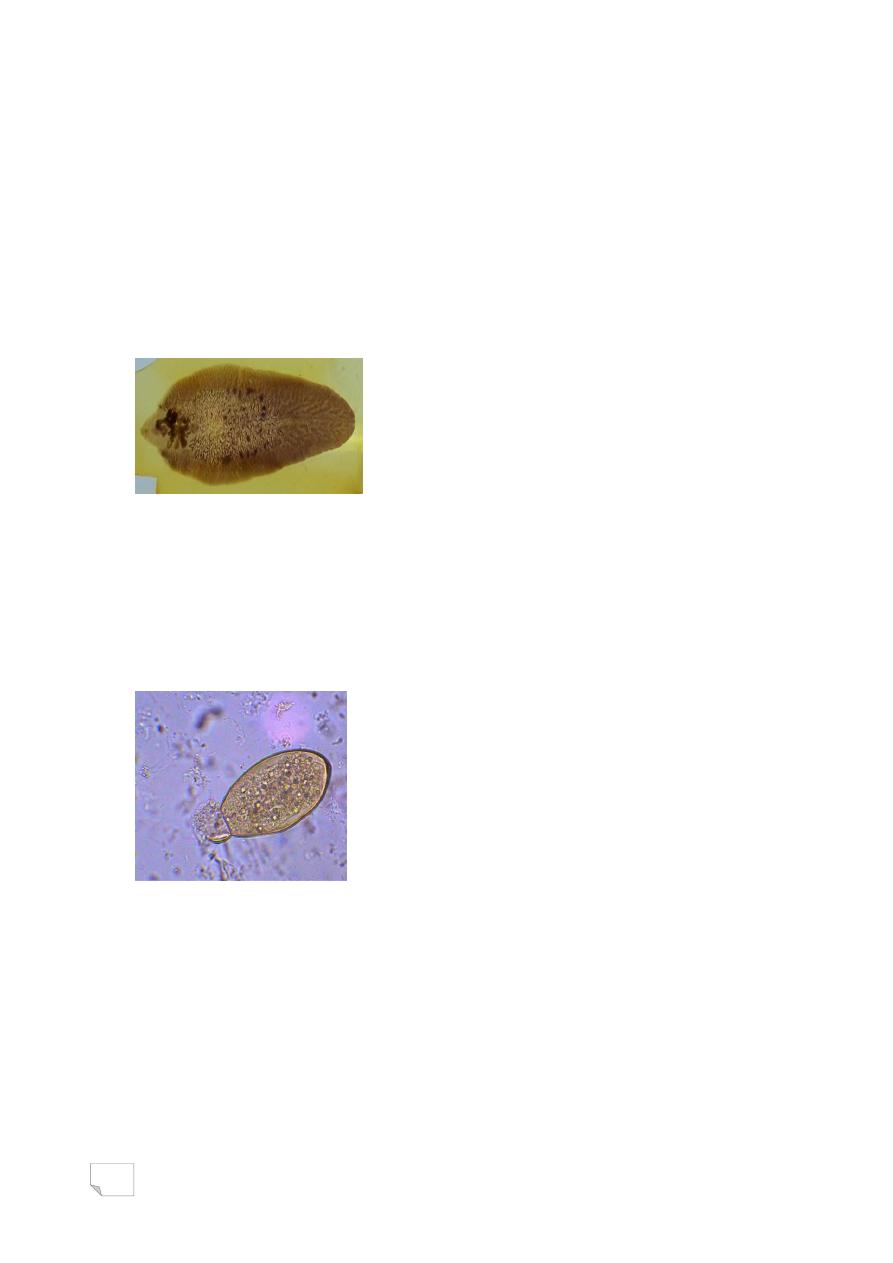
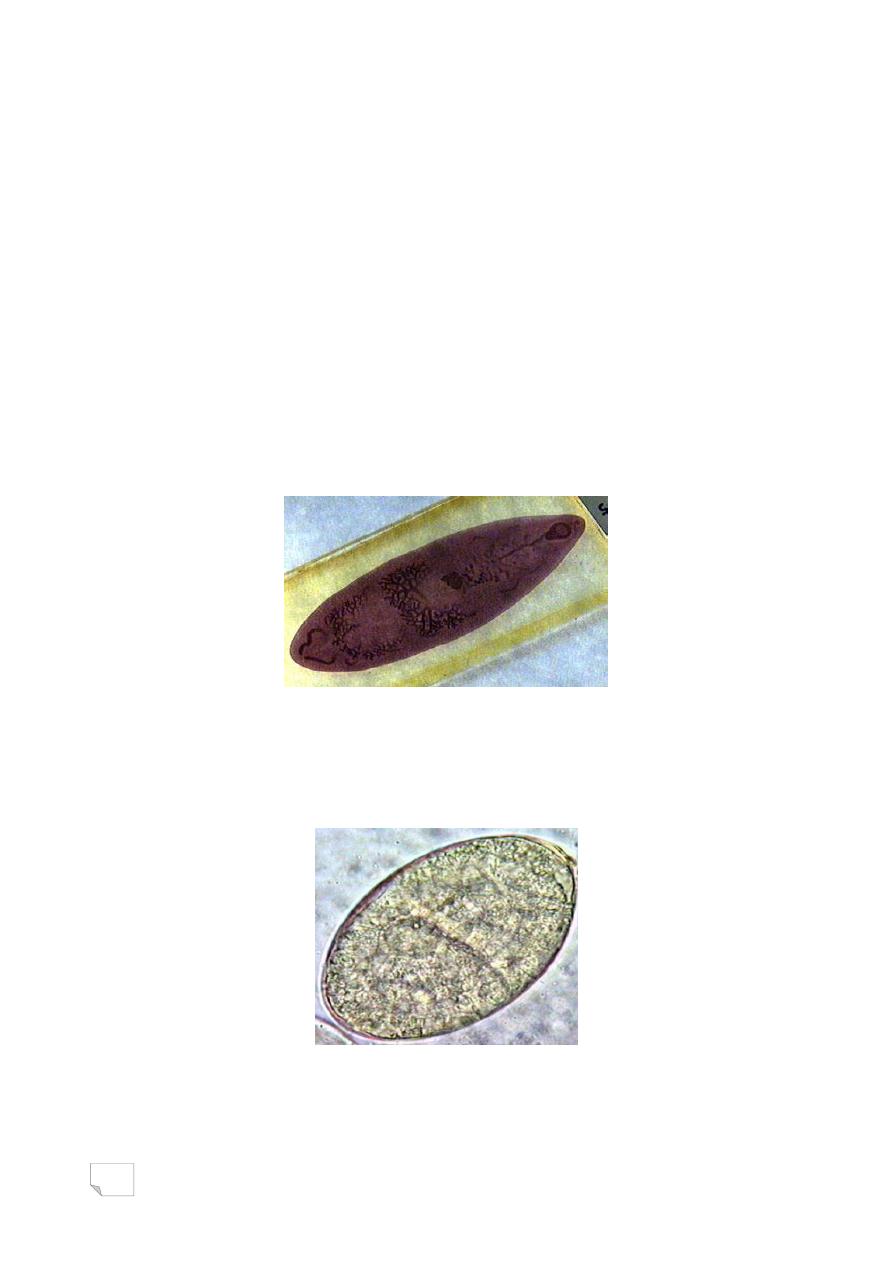
MORPHOLOGY
Egg
The eggs are large, ovoid, bile-stained and have a small operculum.
These are unembryonated when freshly passed.
MORPHOLOGY
Metacercaria (infective form)
Metacercaria is the infective form for man and other definitive hosts.
It is found on the surfaces of aquatic vegetations and water cress.
23
24
PATHOGENESIS AND PATHOLOGY
Both migrating larvae and adult worms produce pathogenic lesions.
Pathogenicity of larva
The migration of the larvae in the liver induce traumatic or necrotic
lesions, which characterize the acute phase of the disease.
PATHOGENESIS AND PATHOLOGY
Pathogenicity of adult fluke
The adult fluke causes biliary obstructive symptoms seen during
chronic phase of disease. Also adult Fasciola causes inflammation and
thickening of the wall of biliary tract.
CLINICAL MANIFESTATIONS
Acute fascioliasis: Most common clinical symptoms of acute
fascioliasis are:
• Fever
• Hepatomegaly
• Abdominal pain
• Eosinophilia
CLINICAL MANIFESTATIONS
Chronic fascioliasis
The clinical pictures of the chronic phase are:
• biliary obstruction

25
• Inflammation
• Jaundice
• Secondary bacterial infections
• The adults can live in the biliary ducts, causing symptoms for up to
10 years.
Halazoun
• Halzoun The condition commonly known as halzoun is a type of
Fasciola hepatica infection in which the worm settles in the
pharynx. This occurs when an individual consumes infected raw
liver. The young adult worms then attach themselves to the
pharyngeal mucosa which causes considerable pain, edema, and
bleeding that can interfere with respiration.
• Ectopic Infection Ectopic infections through normal transmission
are infrequent but can occur in the peritoneal cavity, intestinal wall,
lungs, subcutaneous tissue, and very rarely in other locations.
Reservoir, source and transmission of infection
Main source of infection are aquatic vegetations and water cress
contaminated with the metacercariae.
Sheep is the key reservoir.
Man is an accidental host.
Reservoir, source and transmission of infection
Infection is transmitted orally by:
1. Ingestion of contaminated water plants mainly, watercress and lettuce
that are eaten raw.
2. Drinking contaminated water from irrigated canals.
3. Consumption of raw infected sheep, goat or cow liver.
LABORATOEY DIAGNOSIS
1. Parasitic diagnosis: A) Stool microscopy:
It is based on the microscopy demonstration of eggs in the faeces.

26
Stool microscopy is very useful in the diagnosis of chronic
fascioliasis, but not useful in acute fascioliasis because eggs
seldom are excreted in the faeces in acute fascioliasis.
LABORATOEY DIAGNOSIS
b. Stool antigen detection:
Recently, ELISA has been evaluated to demonstrate Fasciola copro –
antigen in stool to diagnose chronic fascioliasis.
LABORATOEY DIAGNOSIS
2. Serological diagnosis:
Specific antibodies against Fasciola are detected in the serum. The
commonly used serological tests are the immunoelectrophoresis, indirect
haemagglutination assay, indirect immunoflourescence and enzyme-
linked immunosorbent assay (ELISA).
LABORATOEY DIAGNOSIS
Serological tests are useful in:
1. The early diagnosis of fascioliasis before the liver is damaged too
much.
2. The diagnosis of acute fascioliasis, in which the eggs are not found
in the faeces.
3. Ruling out " pseudofascioliasis" or false fascioliasis.
LABORATOEY DIAGNOSIS
3. Imaging methods
Ultrasound and CTSCAN may detect the fluke in the gallbladder or
bile duct.
MRI may reveal granulomata of the liver parenchyma in cases of
fascioliasis.
• Prevention
• Water-grown vegetables should be washed with 6% vinegar or
potassium permanganate for 5-10 minutes, which kills the encysted
metacercariae. This approach is more successful than attempts to
halt the consumption of raw vegetables.
• Cook water-grown vegetables thoroughly before eating.

27
Prevention
• Avoid sewage contamination of growing areas.
• Use of molluscicides is the most frequent public health
intervention, as it prevents the transmission of many other
trematodes, including Schistosoma spp.
• Treatment of animals to reduce the reservoir and reduce stock
losses has been used. Until the introduction of single-dose
triclabendazole, bithionol was the only available treatment, much
limited by expense and treatment duration.
• For the future, vaccination would seem to be a feasible option.
Fasciola gigantica
• Geographic Range
• Fasciola gigantica is found in tropical Africa, South and South-east
Asia, and the Far East. In the United States F. gigantica is found in
Hawaii.
Fasciola gigantica
• Habitat
• The habitat of Fasciola gigantica changes with the stage of its life
cycle. Adult F. gigantica live in the liver and bile ducts of its
definitive hosts (sheep, cattle, and other grazing ruminant
mammals).
Morphology
• Fasciola gigantica is leaf-shaped and tapers at both ends. An adult
can grow to 75 mm in length. With the use of a scanning electron
microscope the surface of F. gigantica appears very rough due to
abundant microscopic spines and surface folding.
28
29
30
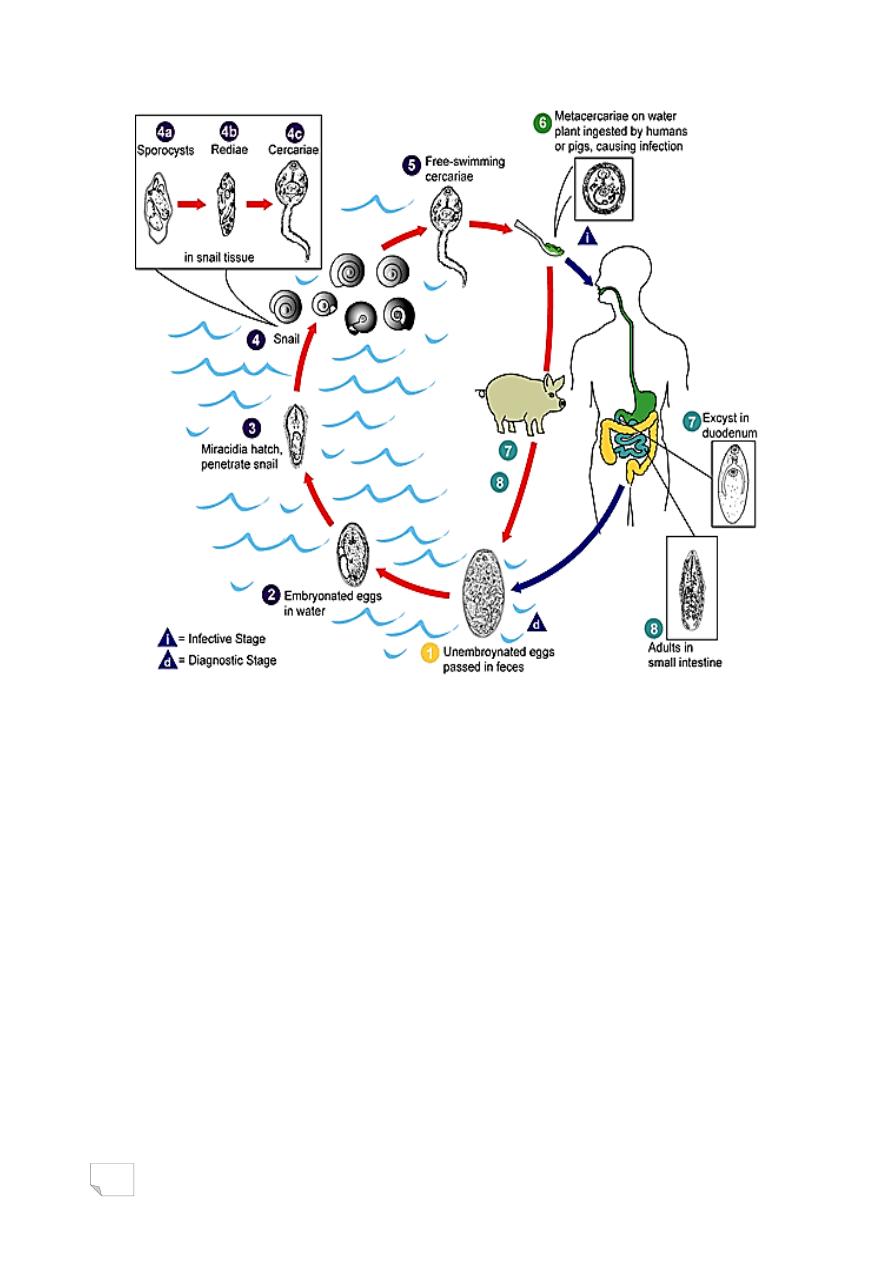
Fasciolopsis buski
(Lankester,1857)Odhner,1902
Fasciolopsis buski also known as intestinal fluke, which causes
fasciolopsiasis in humans.
HABITAT
It is found attached to the mucosa of the duodenum and jejunum of pig
and man.
MORPHOLOGY
Adult: Fasciolopsis buski is the largest intestinal fluke which parasitize
man. It measures 2-7.5cm in length. It is fleshly, and elongated with a
broadly rounded anterior end. Oral sucker is smaller
than ventral sucker.
MORPHOLOGY
Egg is large oval in shape, bile-stained and have operculum.
Metacercaria (Infective form)
Metacercariae are infective to man and pig.They are encysted form,
found on the fresh water plants.
31
PATHOGENESIS AND PATHOLOGY
At site of attachment in the intestine, adult fluke causes localized
haemorrhagic inflammation, ulceration and mucous secretion.
The flukes also cause malabsorption leading to hypoalbuminemia,
protein-losing enteropathy, impaired vitamin B12 absorption and
also cause toxaemia.
CLINICAL MANIFESTATIONS
• Fasciolopsis buski caused Fasciolopsiasis.
• The condition usually is asymptomatic.
• In heavy infections, the symptomatology consists of:
• epigastric pain
• nausea
• diarrhea
• severe anemia.
32
Reservoir, source and transmission of infection
The source of infection to man is aquatic plants infected with the
metacercariae.
Pig is a major reservoir host, also man is the reservoir of infection
for snails.
Infection occurs orally on ingestion of various parts of infected
water plants.
DIAGNOSIS
Definitive diagnosis of Fasciolopsis is based on the detection of large
operculated eggs in the faeces by microscopy.
Summary or Conclusion:
• Fasciola hepatica also called liver fluke, causes human
fascioliasis.
• Fascioliasis occur worldwide, particularly in countries where
intensive sheep or cattle rearing are carried out.
• It is large, flat and leaf-shaped.
• Egg is diagnostic stage, metacercaria is infective stage.
• Needs two intermediate hosts to completed their life cycle.
• Main source of infection are aquatic vegetations and water cress
contaminated with the metacercariae.
Lec: 5
33
Fasciolopsis buski
(Lankester,1857)Odhner,1902
Fasciolopsis buski also known as intestinal fluke, which causes
fasciolopsiasis in humans.
HABITAT
It is found attached to the mucosa of the duodenum and jejunum of
pig and man.
MORPHOLOGY
Adult: Fasciolopsis buski is the largest intestinal fluke which parasitize
man. It measures 2-7.5cm in length. It is fleshly, and elongated with a
broadly rounded anterior end. Oral sucker is smaller than ventral sucker.
MORPHOLOGY
Egg is large oval in shape, bile-stained and have
operculum.
Metacercaria (Infective form)
Metacercariae are infective to man and pig. They are encysted
form, found on the fresh water plants.

34
PATHOGENESIS AND PATHOLOGY
At site of attachment in the intestine, adult fluke
causes localized haemorrhagic inflammation, ulceration and
mucous secretion.
The flukes also cause malabsorption leading to hypoalbuminemia,
protein-losing enteropathy, impaired vitamin B12 absorption and
also cause toxaemia.
CLINICAL MANIFESTATIONS
› Fasciolopsis buski caused Fasciolopsiasis.
› The condition usually is asymptomatic.
› In heavy infections, the symptomatology consists of:
• epigastric pain
• nausea
• diarrhea
• severe anemia.

35
Reservoir, source and transmission of infection
The source of infection to man is aquatic plants infected
with the metacercariae.
Pig is a major reservoir host, also man is the
reservoir of infection for snails.
Infection occurs orally on ingestion of various parts of
infected water plants.
DIAGNOSIS
Definitive diagnosis of Fasciolopsis is based on the
detection of large operculated eggs in the faeces by
microscopy.
Questions?

36
د. رؤى طفيليات
25
\
3
\
2181
( عدد االوراق
4
) م
\
3
\
موصل
lec:6
Paragonimus westermani
List of Contents:
• Objectives
• Introduction
i.
Morphology
ii.
Life cycle
iii.
Pathogenesis and pathology
iv.
Clinical manifestation
v.
Reservoir, source and transmission of infection
vi.
Diagnosis
• Summary or conclusion
• Question
Objectives:
• General characteristics of Paragonimus westermani.
• Common name and the disease.
• Habitat of Paragonimus westermani.
• Infective stage and diagnostic stage.
• How is transmit to human.
• Pathogenesity of Paragonimus westermani.
• Diagnosis
37
Introduction
• Paragonimus westermani also known as lung fluke.
• Causes endemic haemoptysis or pulmonary paragonimiasis in man.
• Habitat
In man and other definitive hosts, the adult worm lives in lung tissue.
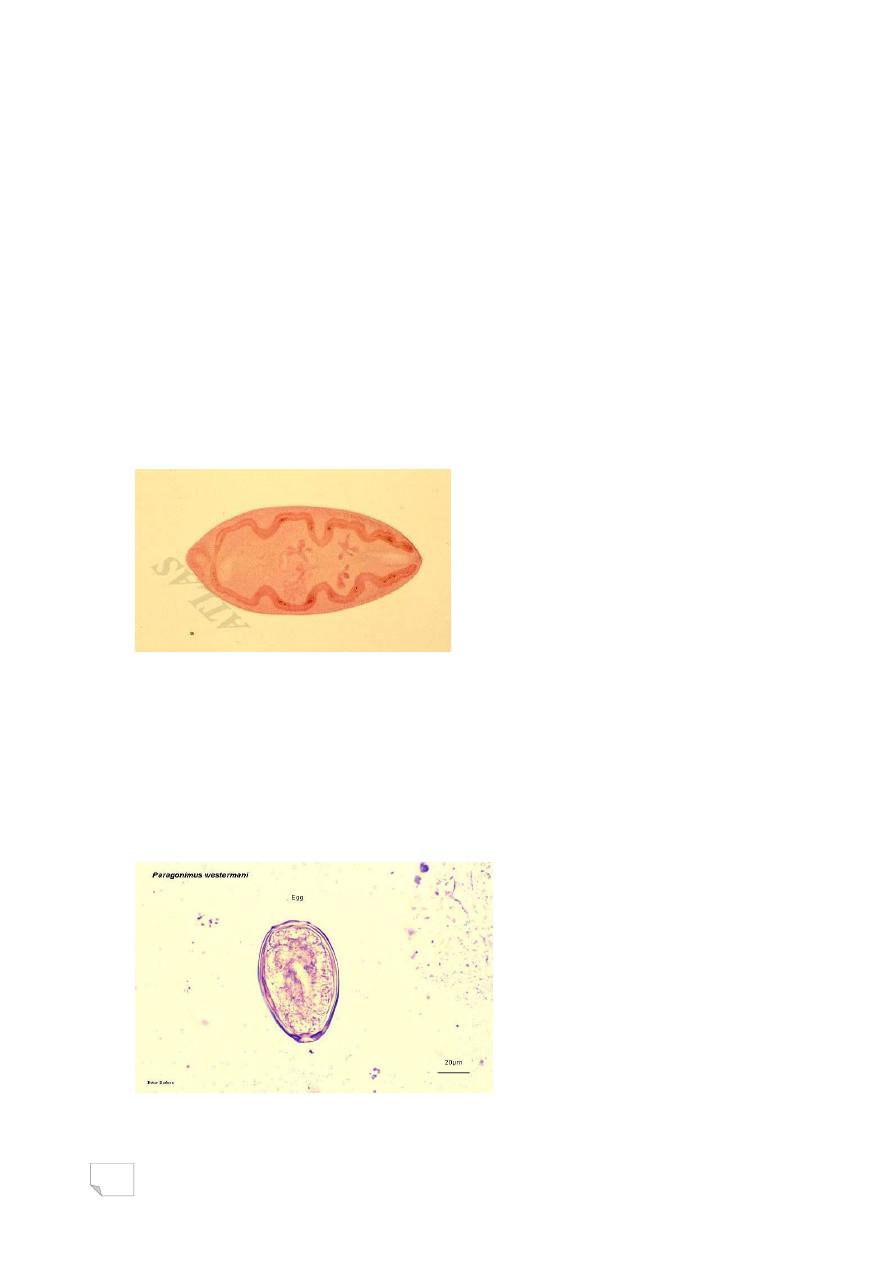
MORPHOLOGY
Adult worm
Adult P. westermani is thick, fleshly and when freshly passed, it is
reddish brown in colour. The fluke is egg-shaped, and has two suckers:
oral and ventral sucker (in equal size).
MORPHOLOGY
Egg
Golden-brown, oval in shape and operculated.
Eggs are excreted unembryonated in sputum or stool.
38
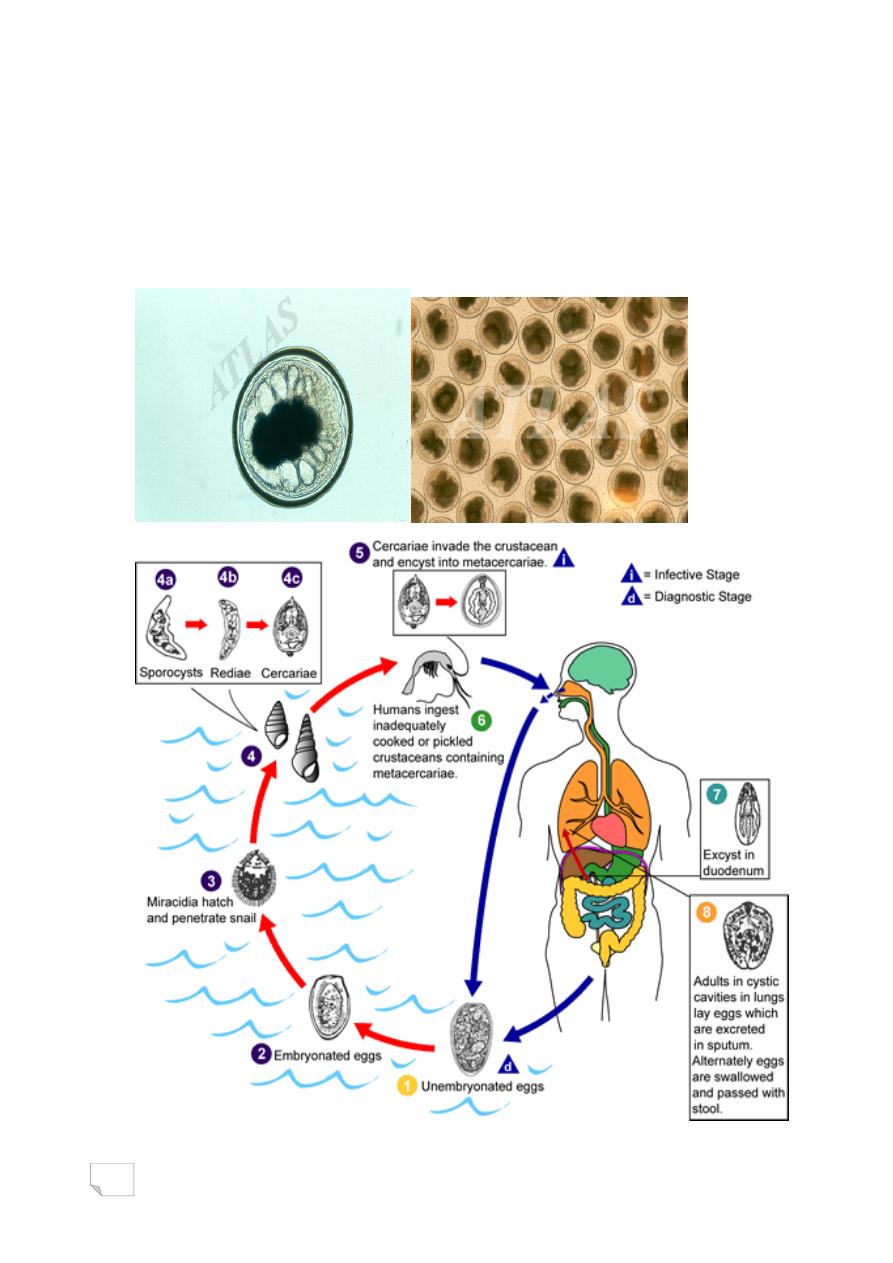
MORPHOLOGY
Metacercaria
Metacercaria is infective stage. It is the encysted form found in the
flesh of various crustaceans (fresh water crayfish and crabs).

39
PATHOGENESIS AND PATHOLOGY
Both live adult flukes and eggs are pathogenic. The larvae are not
pathogenic.
Pathogenicity of adult fluke
Adult fluke stimulate an encapsulating inflammatory reaction, in which
adult flukes are encapsulated by cysts. Each cyst contains 2-4 flukes.
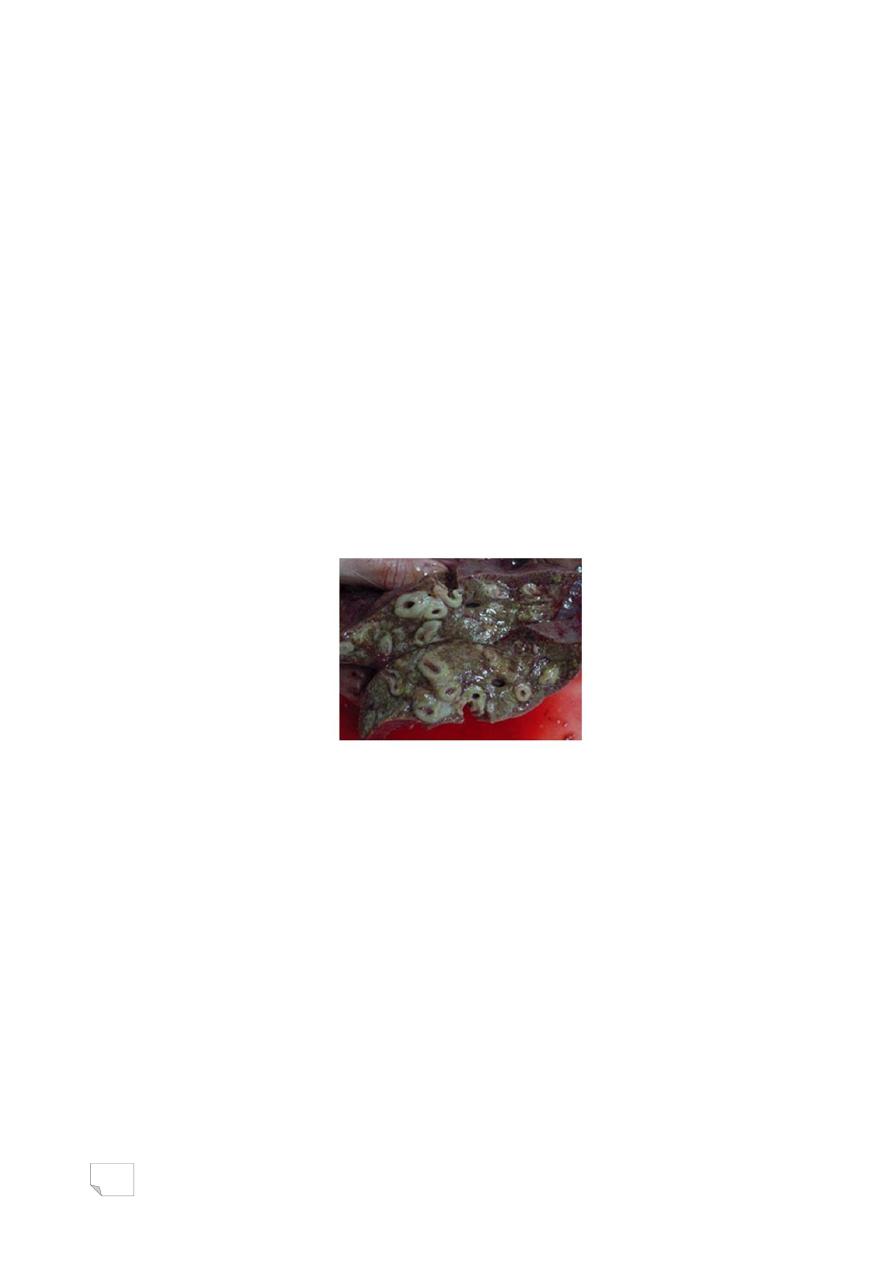
PATHOGENESIS AND PATHOLOGY
Lung infected by Paragonimus westermani
PATHOGENESIS AND PATHOLOGY
The eggs also stimulate an inflammatory reaction resulting in the
formation of cysts.
The cystic encapsulation of the eggs in the lung is the key pathological
feature of paragonimiasis.
PATHOGENESIS AND PATHOLOGY
During course of infection, these cysts rupture and open into
bronchioles. The eggs with blood are exudates out in the sputum or if
swallowed, are passed in the faeces.
Cysts may also occur in the intestinal wall, liver, spleen or abdominal
wall.

40
CLINICAL MANIFESTATION
Light infections are asymptomatic. In symptomatic infection,
paragonimiasis is characterized by
fever,
cough with golden brown sputum,
night sweat,
diarrhea,
chest pain and
haemoptysis.
Reservoir, source and transmission of infection
• Man, domestic and wild carnivores animals are the important
reservoirs of paragonimiasis.
• Fresh water crabs and crayfish containing metacercariae are the
main sources of infection.
Reservoir, source and transmission of infection
Human infection is acquired by:
1. Eating raw or partially cooked crab and crayfish.
2. Eating raw pork, from wild pigs, containing the larvae of paragonimus
species.
3. The hands and utensils that are contaminated, when the crayfish and
crab are prepared for the food.
DIAGNOSIS
Parasitic diagnosis
Definitive diagnosis depends on the microscopic demonstration of the
eggs in the sputum or faeces. Examination of stool very useful for the

41
diagnosis of ova-negative sputum cases particularly in children due to
their habit of swallowing the sputum.
DIAGNOSIS
Immunodiagnosis (Serological tests)
A number of serological tests including complement fixation, indirect
haemagglutination assay, immunoelectrophoresis and latex agglutination
test are available for the detection of serum antibodies in the infection.
DIAGNOSIS
The serodiagnositc methods are useful in:
1. Pre-patent period in which the eggs are difficult to demonstrate in
the stool or sputum.
2. Extra-pulmonary paragonimiasis (e.g., cerebral paragonimiasis)
because the eggs are not excreted either in the sputum or in the
stool.
DIAGNOSIS
Imaging studies
In pulmonary paragonimiasis, chest x-ray shows
abnormalities in lung tissue.
In cerebral paragonimiasis, CTscan or MRI of the head may show
cerebral calcification.
Imaging methods are very useful to differentiate paragonimiasis
from tuberculosis.
Summary or Conclusion:
P. westermani known as lung fluke, lives in lung.
Causes endemic haemoptysis or pulmonary paragonimiasis in man.
It is thick, and egg-shaped.
42
Egg is diagnostic stage, and excreted in sputum or stool.
Metacercaria is infective stage.
Needs two intermediate hosts to completed their life cycle.
Adult fluke and egg stimulate an encapsulating inflammatory
reaction in the lung.
Fresh water crabs and crayfish containing metacercariae are the
main sources of infection.