Infection of the Fascial spaces
2Infections of spaces in relation to the upper jaw
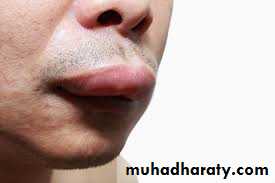
• Upper lip infectionInfections of the upper incisors and canines can spread to the upper lip usually on the oral side of Orbicularis Oris muscle and points in the vestibule.
Infection of the upper lip can lead to serious complications like orbital cellulitis or cavernous sinus thrombosis by extension of infection through the superior labial vein to anterior facial vein to ophthalmic vein to cavernous sinus. Incision for drainage is made near the vestibule intraorally.
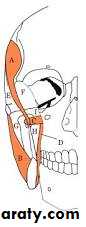
• Canine fossa infections
Anatomic boundaries it lies between the canine fossa and the muscles of the facial expression.Source of infection: mostly is the canine and first premolar but the infection can spread from upper incisor teeth.
Infection occurs when it spreads in the area above the origin of the Levator Anguli Oris and is directed toward the medial edge of the Levator Labii Superioris.
The swelling is lateral to the nose leading to obliteration of the nasolabial fold and may lead to periorbital cellulitis, there is risk of cavernous sinus thrombosis.

Site of incision and drainage: intraoral horizontal incision in the buccal vestibule.

• Buccal space infections
Infections spread from infected upper molar teeth where it spreads buccally above the attachment of Buccinator muscle. This space is already discussed.


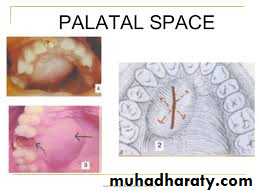
• Sub periosteal abscess in the palate:
This potential space lies between the palatal mucoperiosteum and the underlying bone, the mucoperiosteum is strongly attached in the midline and at the gingival margin, pus may accumulate beneath the mucoperiosteum leading to its separation from the underlying bone.
Source of infection :it may spread from the apex of the lateral incisor which is close to the palatal bone. Also infection can spread from the palatal root of multi-rooted upper molars. It can also originate from palatal periodontal pocket.
The swelling causes palatal bulge between the gingival margin and the midline, confined to one side.
Site of incision and drainage: anteroposterior incision parallel to greater palatine vessels.
• Maxillary antrum :
Infection from upper molars and less frequently premolars may spread to the maxillary antrum, this depends on the size of the maxillary antrum and the length of the root.It causes acute sinusitis with facial pain that worsens on bending or leaning forward, the infection may lead a chronic course leading to mucosal thickening and polyps. Occipito-mental radiograph shows opaque maxillary sinus or fluid level.
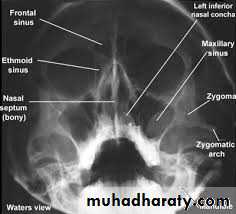

Pus may drain partially through the sinus osteum, extraction of the causative tooth leads to drainage of pus but it may leave a defect in the floor of the sinus and cause oro-antral fistula. If the defect is small and with antibiotic treatment the socket may heal uneventfully, but larger defects may require further management.
• Infratemporal space infection :
Anatomic boundaries :this space is bounded laterally by the ramus of the mandible and the Temporalis muscle, medially by lateral pterygoid plate, superiorly by infratemporal surface of the greater wing of the sphenoid. It is traversed by the maxillary artery and contains pterygoid venous plexus. It represents the upper extremity of the pterygomandibular space.
Source of infection: directly from upper molar teeth or through contaminated needle from the pterygomandibular space. Infection may spread to the temporal space.
.

Sign and symptoms:
moderate swelling in the temporal region.trismus,
patient is toxic with high temperature.
can spread through the pterygoid venous plexus to the cavernous sinus through emissary vein or it can spread to the middle cranial fossa with headache, photophobia, irritability, vomiting and drowsiness
Site of incision and drainage:
intraorally: through an incision buccal to the upper third molar following the medial surface of the corronoid upward and backward, but with the presence of trismus this approach is difficult.Extraorally through an incision in the upper and posterior edges of the Temporalis muscle within the hair line passing downward, forward and medially.
Cavernous sinus thrombosis
It is a very serious ascending infection, although not a fascial space infection but it can be caused by odontogenic infections especially of upper teeth. It can also result from upper lip, nasal and orbital infections.Infection can spread to the cavernous sinus through two routes:
• Anterior route; through the valveless angular vein and inferior ophthalmic vein.
• Posterior route; through the pterygoid venous plexus and transverse facial vein.
This infection has a high mortality rate.
Clinical features:
• Marked edema and congestion of the eyelids and conjunctiva which can be bilateral due to the spread of infection to the other side.• Proptosis (exophthalmos) and ptosis.
• Ophthalmoplegia and dilated pupil.
• Papilloedema with multiple retinal hemorrhage.
• Fever.
• Depressed level of consciousness.
•

Treatment:
It is an emergency that requires a neurosurgical consultation, the lines of treatment include:
• Antibiotic treatment
• Heparinization to prevent extension of thrombosis.
• Treatment of the odontogenic cause.
Principles of treatment of odontogenic infections
• In treating odontogenic infections, the clinicians need to identify the presence of infection through the presence of the local and systemic signs and symptoms of the infection and whether it is cellulitis or abscess, also to determine the state of the host defenses, as these can be depressed by many factors such as; physiologic factors, disease related factors, immune-system related factors and drug suppression related factors.• Treatment of odontogenic infections requires medical, surgical or dental therapy or a combination.
• Dental treatment; it aims to eliminate the source of infection through endodontic treatment, periodontal treatment or extraction of the offending tooth. These factors should be taken in consideration:
• The extent of infection.
• Patient general health status.
• Degree of trismus.
• Biomechanical necessity of retaining the tooth.
• Surgical treatment; it aims to drain the accumulated pus to rid the body of the toxic purulent material and to relieve and decompress the tissues allowing better perfusion of blood to the infected area.
Methods of drainage:
1. Through the root canal after access opening.2. Through the socket by extraction of the offending tooth.
3. Through fenestration of alveolar bone using surgical hand piece and bur made at the level of the root apex, to drain periapical abscess, after reflection of a semilunar mucoperiosteal flap.
4. Through incision and drainage of an abscess.
Incision and drainage:
Is one of the oldest surgical procedures, it requires a thorough knowledge of facial and neck anatomy which is necessary particularly in draining deep tissue abscesses, on the other hand drainage of vestibular and dentoalveolar abscess is easily carried out.
Indications of incision and drainage:
When there are signs of accumulation of pus, ideally abscess should be drained when fluctuant, prior to spontaneous rupture and drainage.
Principles of incision and drainage:
• incisions should be placed in an area of maximum fluctuation in a dependent position to encourage drainage by gravity.• Incise in healthy skin and mucosa as possible Incisions made in areas where the tissue is necrotic or beginning to perforate may leave unaesthetic scars.
• It should be placed in an esthetically acceptable area, in a natural skin crease or fold.
• Incision in the skin of face and neck should include only the skin and subcutaneous tissues and the dissection through deeper tissues is continued bluntly using closed sinus or artery forceps which are advanced by controlled pressure to the pus containing tissue space and ,opened inside the cavity, then the forceps are drawn open then closed again and reinserted. The process is repeated until all the pus is evacuated. This is termed Hilton's method (after john Hilton, an English surgeon 1804-1878).
• The forceps should not be closed inside the tissue to avoid damage to vital structures.
• Intraorally, in vestibular abscess, the pus accumulates under the mucosa with no intervening vital structures, so incision and drainage is made by the scalpel through the abscess cavity, here scalpel blade no. 11 is preferably used.
• Generally all portions of the abscess cavity should be explored to ensure evacuation of all compartments, sometimes through and through drainage is necessary.
• After incision and evacuation of pus a drain is inserted into the abscess cavity and is stabilized with suture. Corrugated drains or Iodoform ribbon gauze can be used for this purpose. Drains should not be left for long periods, they should be removed when the drainage is minimal.


• Wound margins should be cleaned daily to remove clots and debris. a sample of pus should be obtained and sent to the laboratory for culture and sensitivity, sometimes this can be achieved by aspiration with a syringe and needle prior to incision and drainage.

Medical treatment; it consists of supportive care which include hydration, soft diet, analgesics and good oral hygiene, and antibiotic therapy. It is essential to say that medical treatment is not a substitute for surgical treatment if indicated.
In treatment of odontogenic infections, antibiotics are indicated therapeutically in the following cases:
1. Acute cellulitis.
2. Acute pericoronitis with elevated temperature and trismus.
3. Deep fascial space infections.
4. Dental infections in the compromised host.
