د.اشرف مزاحم الشاكر
كلية طب نينوى
lec:2
1
General and specific Perioperative Care of the Surgical
Patient
5. Diabetes mellitus.
Diabetic patients are at increased risk of morbidity and mortality.
Vascular disease is common in diabetics, and MI, often with an atypical presentation, is the
leading cause of perioperative death among diabetic patients.
a. Preoperative evaluation. All diabetic patients should have their blood glucose measured
in pre-op holding and intraoperatively to prevent unrecognized hyperglycemia or
hypoglycemia.
(1) Patients with diet-controlled diabetes mellitus can be maintained safely without food or
glucose infusion before surgery.
(2) Oral hypoglycemic agents should be discontinued the evening before scheduled
surgery. Long-acting agents such as chlorpropamide or glyburide should be discontinued 2 to
3 days prior.
(3) Insulin-dependent diabetics require insulin and glucose preoperatively to prevent
ketosis and catabolism. Patients undergoing major surgery should receive one-half of their
morning insulin dose and 5% dextrose intravenously. Subsequent insulin administration by
either subcutaneous (SC) sliding-scale or insulin infusion is guided by frequent blood
glucose determinations. SC insulin pumps should be inactivated the morning of surgery.
6. Anticoagulation.
The most common indications for warfarin therapy are atrial fibrillation,
venous thromboembolism (VTE), and mechanical heart valves. Warfarin's anticoagulant
effect endures for several days following cessation of the drug. Recommendations for the
management of anticoagulation in the perioperative period require weighing the risks of
thromboembolic events against the risk of perioperative bleeding.
a. Preoperative anticoagulation. Surgery is generally safe when the international
normalized ratio (INR) value is below 1.5. Patients whose INRs are maintained between 2.0
and 3.0 normally require withholding of the medication for 5 days preoperatively.
b. Patients with high risk of thrombotic complications should be managed with bridging
anticoagulation. This can consist of transitioning as an outpatient with low-molecular-
weight heparin (LMWH, stopped 24 hours prior to surgery) or as an inpatient with an
unfractionated heparin (UFH, stopped 4 to 6 hours prior to surgery) infusion when
Coumadin is stopped.
c. Postoperative anticoagulation. Coumadin requires several days to reach therapeutic
levels, so therapy can be resumed on postoperative days 1 or 2. High-risk patients should be
bridged with therapeutically dosed SC LMWH or IV UFH until their INR is therapeutic;
د.اشرف مزاحم الشاكر
كلية طب نينوى
lec:2
2
moderate-risk patients can be bridged with therapeutically dosed SC LMWH, therapeutically
dosed IV UFH, or prophylactically dosed SC LMWH. Low-risk patients do not need to be
bridged.
d. Emergent procedures. In urgent or emergent situations in which there is no time to
reverse anticoagulation before surgery, plasma products, such as fresh frozen plasma (FFP),
must be administered. Vitamin K can be administered, but its effects will not be seen for 8
hours if given orally and it will continue to counteract Coumadin given postoperatively.
II. INTRAOPERATIVE MONITORING OF THE PATIENT
What parameters must be monitored in all anaesthetized patients?
Respiratory: inspired O2 (Fi O2), pulse oximetry, end-tidal CO2.
Cardiovascular: heart rate, blood pressure, ECG, invasive blood pressure monitoring
(usually only in major surgery) and central venous pressure (usually only in major
surgery).
Temperature.
III. POSTOPERATIVE CARE OF THE PATIENT
1. Intravenous fluids
. The intravascular volume of surgical patients is depleted by both
insensible fluid losses and redistribution into the third space. As a general rule, patients
should be maintained on IV fluids until they are tolerating oral intake. Extensive open
abdominal procedures are associated with a loss of 500 to 1,000 mL/hour and require
aggressive resuscitation.
2. Deep venous thrombosis prophylaxis
. It is important to provide prophylactic therapy to
nonambulatory patients to reduce the risk of deep venous thrombosis (DVT) and pulmonary
embolism (PE). Risk of DVT development depends on both patient and procedure risk
factors. Surgery for major trauma, hip or leg fractures, spinal cord injury, intra-abdominal
cancer, joint replacement, and bariatric surgery are particularly of high risk. The most
significant patient risk factor is a prior history of DVT. Other patient risk factors include
malignancy, thrombophilias, oral contraceptive therapy, obesity, immobility, and indwelling
central venous lines. Prophylaxis should be started preoperatively in patients undergoing
major procedures because of venous stasis and relative hypercoagulability occur during the
operation.
3. Pulmonary toilet.
Pain and immobilization in the postoperative patient decrease the
clearance of pulmonary secretions and the recruitment of alveoli. Patients with inadequate
pulmonary toilet can develop fevers, hypoxemia, and pneumonia. Early mobilization,
incentive spirometry, and cough and deep breathing exercises are indispensable to avoid
these complications.
د.اشرف مزاحم الشاكر
كلية طب نينوى
lec:2
3
4. Pain management:
Pain; An unpleasant sensory and/or emotional experience associated with actual or potential
tissue damage.
What are the principles of post-operative pain management?
Pre-operative:
_ pre-emptive analgesia, e.g. NSAIDs or nerve blocks, patient education.
Intra-operative:
_ use of opioid analgesics, regional nerve blocks, wound infiltration with local anaesthetics.
Post-operative:
_ pharmacological therapy, regional anaesthetic blocks, alternative methods.
What are the alternative methods of pain relief?
Good patient education, Relaxation techniques, Acupuncture, Trans-cutaneous electrical
nerve stimulation (TENS)
What are the systemic effects of post-operative pain?
Cardiovascular: enhanced myocardial O2 demand, myocardial ischaemia, increased
sympathetic stimulation
⇒increased cardiac output⇒reduced renal and splanchnic
perfusion.
Respiratory:decrease cough
⇒sputum retention⇒chest infection, hypoxia.
Gastrointestinal:reduced G.I. motility
⇒constipation, ileus.
Genitourinary: urinary retention.
Metabolic: hyperglycaemia, hypernatraemia.
Psychological: stress, depression.
General: increase hospital in-stay.
some commonly used analgesics in the post-operative period:
Drug
Mode of action
Route
Adverse effects
Paracetamol
Modulates PGE2
in the central
nervous system
po, pr, iv
Rare: unless in
overdose causes
liver failure
NSAIDs (e.g.
ibuprofen,
diclofenac)
inhibits
cyclo-oxygenase
po, pr, iv, im
gastritis, peptic
ulceration, renal
failure,
د.اشرف مزاحم الشاكر
كلية طب نينوى
lec:2
4
bronchospasm in
asthmatics, bleeding
Weak opiates
(e.g. codeine
phosphate)
Act onMu 1
receptors in the
central nervous
system
po, sc, iv, im, pca
Sedation, CNS
depression,
respiratory
depression, nausea,
vomiting, itching,
constipation
Strong
opiates (e.g.
pethidine,
morphine,
fentanyl)
Inhibit ascending
pain pathway
Epidural, spinal
po, sc, iv, im
Respiratory
depression,addiction
Constipation,withdrawal
syndrome.
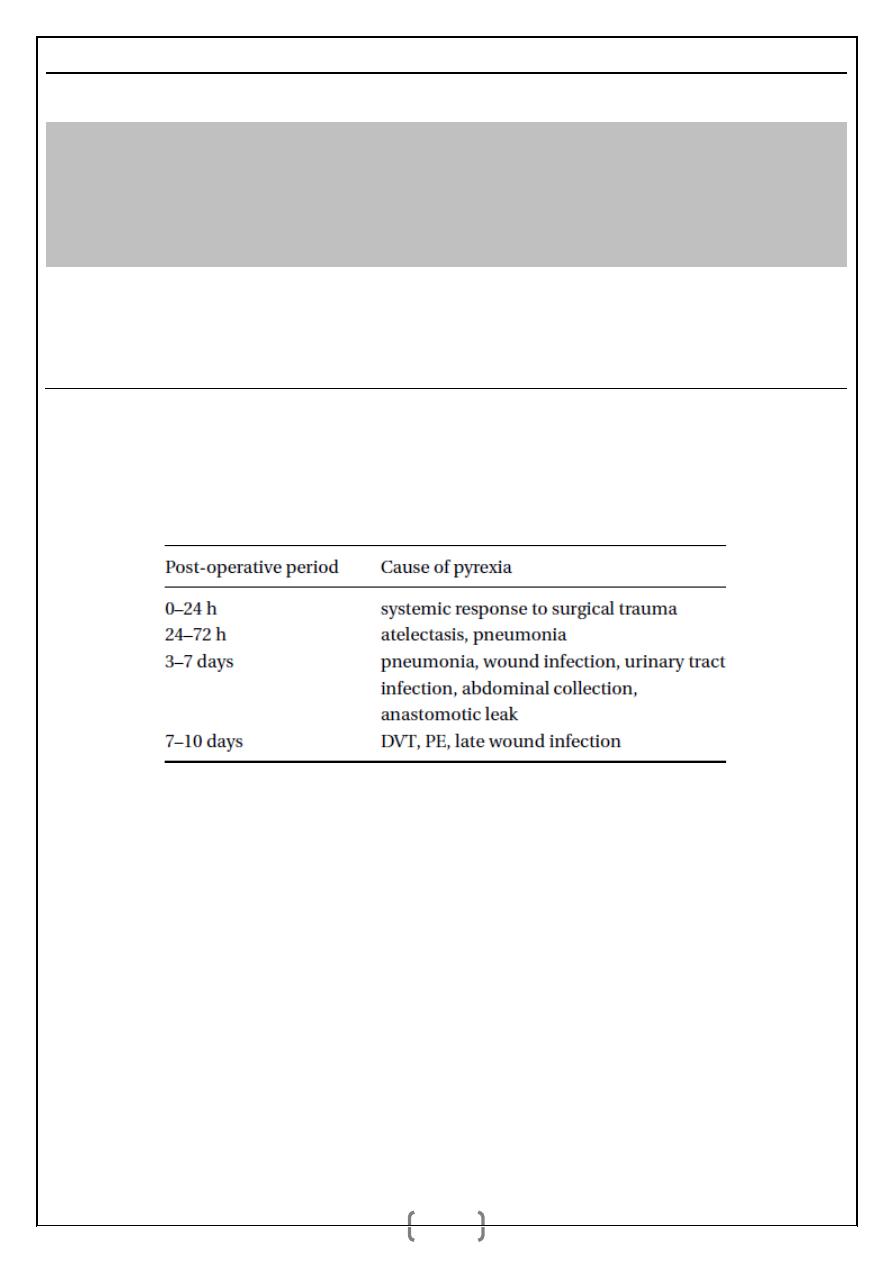
5. Stratification and management of postoperative pyrexia:
They can be summarised according to the post-operative time period in which they
occur.
What is the management of the patient with post-operative pyrexia?
Obtain detailed history: cough, sputum, dysuria, calf pain, abdominal pain,
Thorough clinical examination:
cardiovascular: heart rate, blood pressure.
Respiratory: elevated respiratory rate, breathlessness, crepitations.
Abdominal: distension, signs of ileus.
wound: erythema, swelling, warmth, tenderness, discharge, dehiscence.
calves: swelling, erythema, warmth, tenderness.
Check vital signs:
Temperature (check trend, e.g. persistently elevated, spikes).
cardiovascular: heart rate, blood pressure, urine output.
respiratory: respiratory rate, oxygen saturation.
central nervous system: GCS.
د.اشرف مزاحم الشاكر
كلية طب نينوى
lec:2
5
Investigations:
ECG.
bloods:WCC, U and Es, CRP, ESR, blood cultures.
mid stream urine: dipstick (should also be sent for microscopy and culture).
chest X-ray.
arterial blood gases: metabolic acidosis, hypoxemia.
doppler scan if DVT suspected.
abdominal ultrasound or CT if abdominal collection suspected.
spiral CT or ventilation–perfusion scan if PE suspected.
Treatment: All patients should receive adequate oxygenation and fluid resuscitation.
Specific treatment is outlined below.
Condition
Treatment
Response to trauma
analgesics including paracetamol
Atelectasis
intensive chest physiotherapy, nebulised
bronchodilators, antibiotics should only be
given for associated infections
Pneumonia
chest physiotherapy, antibiotics as per
hospital protocol
Wound infection
antibiotics only once wound swab taken
Urinary tract infection
antibiotics only once MSU sample taken
Abdominal collection
broad spectrum antibiotics including
anaerobic cover; collections should be
drained
Anastomotic leak
radiologically or surgically; anastomotic
leaks may require further surgery
DVT/PE
anticoagulants should be commenced as soon
as possible and must not be delayed until
appropriate investigations are performed