
Extraoral appliances
• Extraoral appliances or orthopedic appliances
are used to modify the growth of maxilla and
mandible using extraoral forces. They are
appliance’s that provide a means of applying
anterior, posterior or vertcal directed forces
to the dentton and skeletal complex from an
extra-oral source
• There are essentally 3 alternatves for treatng
any skeletal malocclusion –
(i) growth modifcaton
(ii) dental camoufage
(iii) orthognathic surgery
• Growth modifcaton should be opted wherever
applicable because this precludes the need for
both tooth extracton and surgery.

• Goal of growth modifcaton is to alter the
unacceptable skeletal relatonships by
modifying the patents remaining facial growth
to favorably change the size or positon of the
jaws. • There are 2 types of orthodontc
appliances that can be used for modifying the
growth of maxilla/mandible-
(i) orthopedic appliances
(ii) functonal appliances

• There are 2 types of forces used in
orthodontcs- 1) orthodontc force – when
applied brings about dental change. They are
light forces ( 50-100 gm) bringing about tooth
movement. 2) orthopedic force – when
applied brings about the skeletal changes.
They are heavy forces ( 300-500gm) that bring
about changes in the magnitude & directon of
bone growth.

• Basis of orthopedic appliance therapy resides
in the use of intermitent forces of very high
magnitude . Such heavy forces when directed
to the basal bone via teeth tend to alter the
magnitude & directon of the jaws by
modifying the patern of bone appositon at
periosteal sutures & growth sites

• 1) Magnitude of force
• Extra oral forces of much greater magnitude,
in excess of 400gms per side is required to
bring about skeletal changes.
• Most orthopedic appliances employ forces in
the range of 400-600 gm per side to maximize
skeletal efect

2) Duraton of force
• Orthopedic changes are best produced by
employing intermitent heavy forces.
• Intermitent forces of 12-14 hours duraton per
day appear to be efectve in producing
orthopedic changes.
• An intermitent heavy force is less damaging to
the teeth and periodontum than a contnuous
heavy force.

3) Directon of force
• Orthopedic force should be applied in the
appropriate directon to have a maximum skeletal
efect.
• The desired changes are best achieved when the
line of force passes through the center of
resistance of the skeletal structures to be moved.
• The force directon or force vector should be
decided depending on the clinical needs

• 4) Age of the patent
• It is advisable to begin orthopedic appliance
therapy while patent is stll in the mixed dentton
period, to make most of the actve growth occurring
prepubertal growth spurt. Treatment may have to
be contnued untl the completon of adolescent
growth, so as to prevent relapse caused by the re-
expression of patents fundamental growth patern
afer cessaton of orthopedic therapy

• The following are the commonly used
orthopeadic appliances.
1. Head gear
2. Reverse pull facial mask
3. Chin cup
Headgear
Headgear
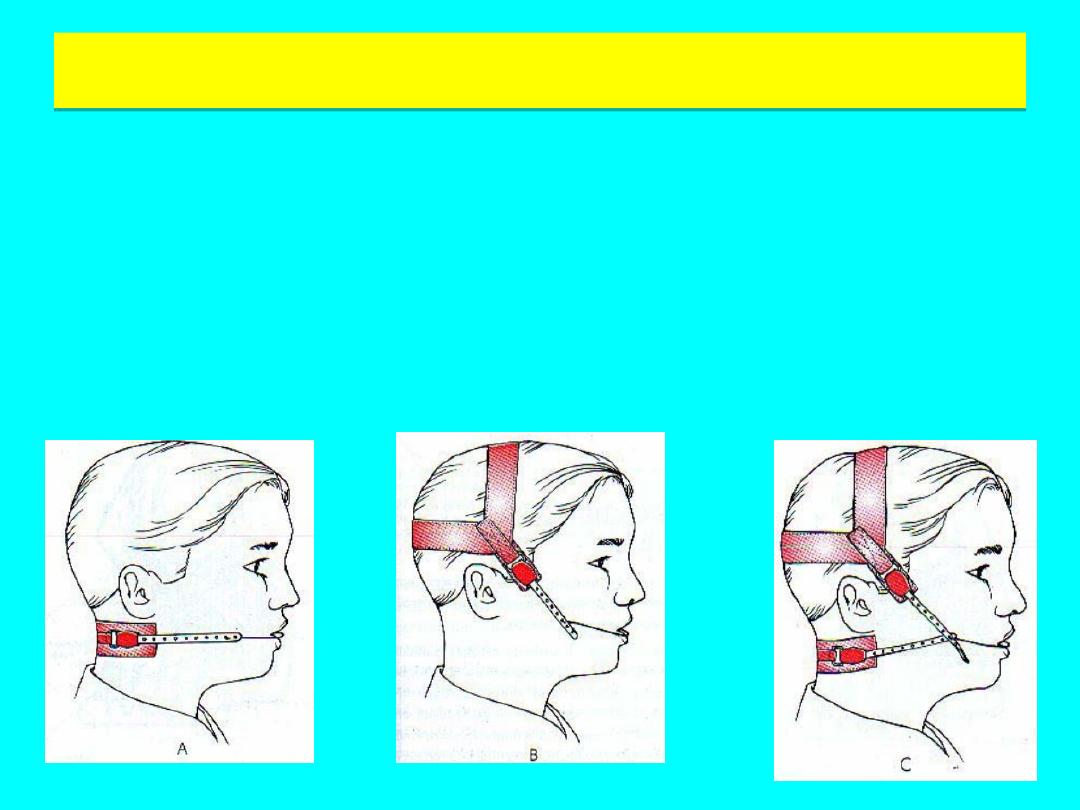
Classifcaton of Headgear
• Cervical headgear (Cervical pull)
• Occipital headgear (High pull)
• Combinaton

• Basic element
1. Force delivering unit
i.e facebow , ‘j- hooks’
2. Force generatng unit
i.e. Elastc, springs
3. Anchor unit i.e. Head
cap, neck pad
• Face bows: are Inner-
outer bow type
• Commonly used with fxed
or functonal/removable
appliance.
• Inner bow is available in
either: 0.045 inch – 0.051
inch
• Outer bow diameter is :
0.072 inch
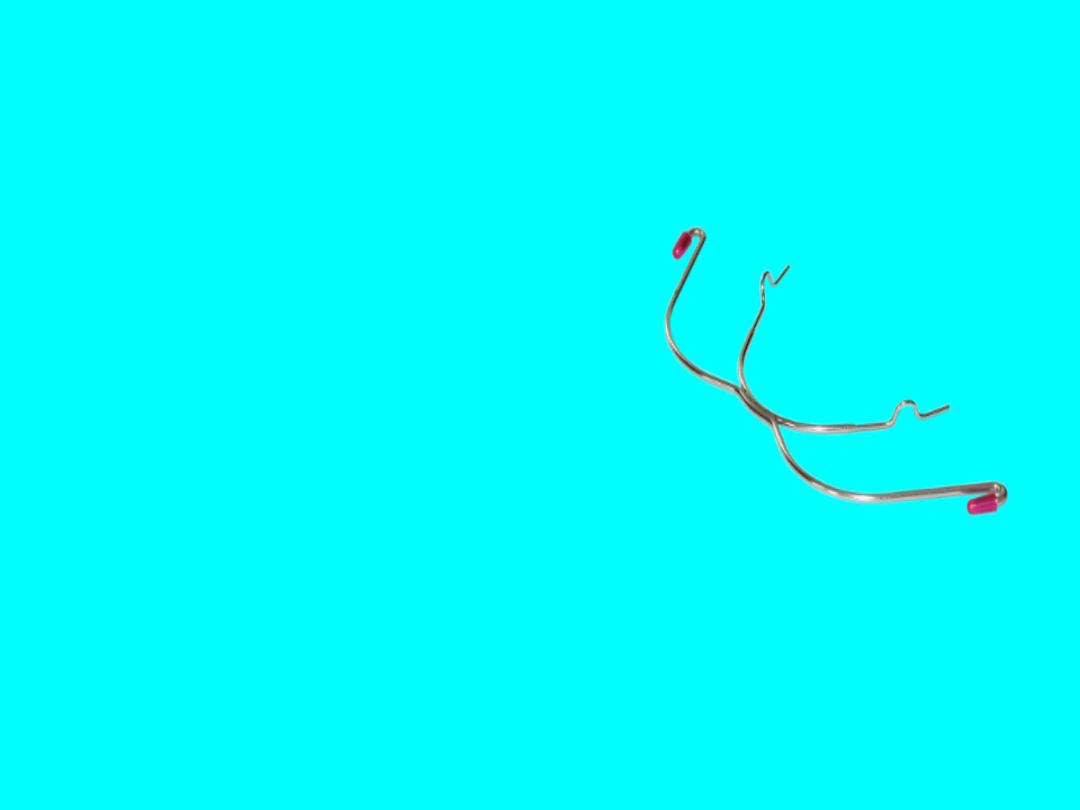
• J-hook type
• An alternatve method
of applying extra-oral
forces to a fxed
appliance.
• The hooks are termed
‘J’ hook on account of
their shape and are
atached directly to the
arch wire usually in the
incisor region

• Each J-hook consist of a 0.072 inch wire
contoured so as to ft over a small soldered
stop on the arch wire.

• Springs: calibrated tension springs are
available. These have the advantage that the
applied force can be varied.
Elastcs: serve
as force elements and are available in the
following forms neck bands with
strong/medium pull extra-oral plastc
chains with length 119mm

• Cervical headgear: it obtained anchorage from
the nape of neck. It cause extrusion for
maxillary molars leading to an increase to
lower facial height. It also move the maxillary
dentton and maxilla distally. Its indicated in
low mandibular angle cases. As an increase in
lower facial height is benefcial in such
patents.

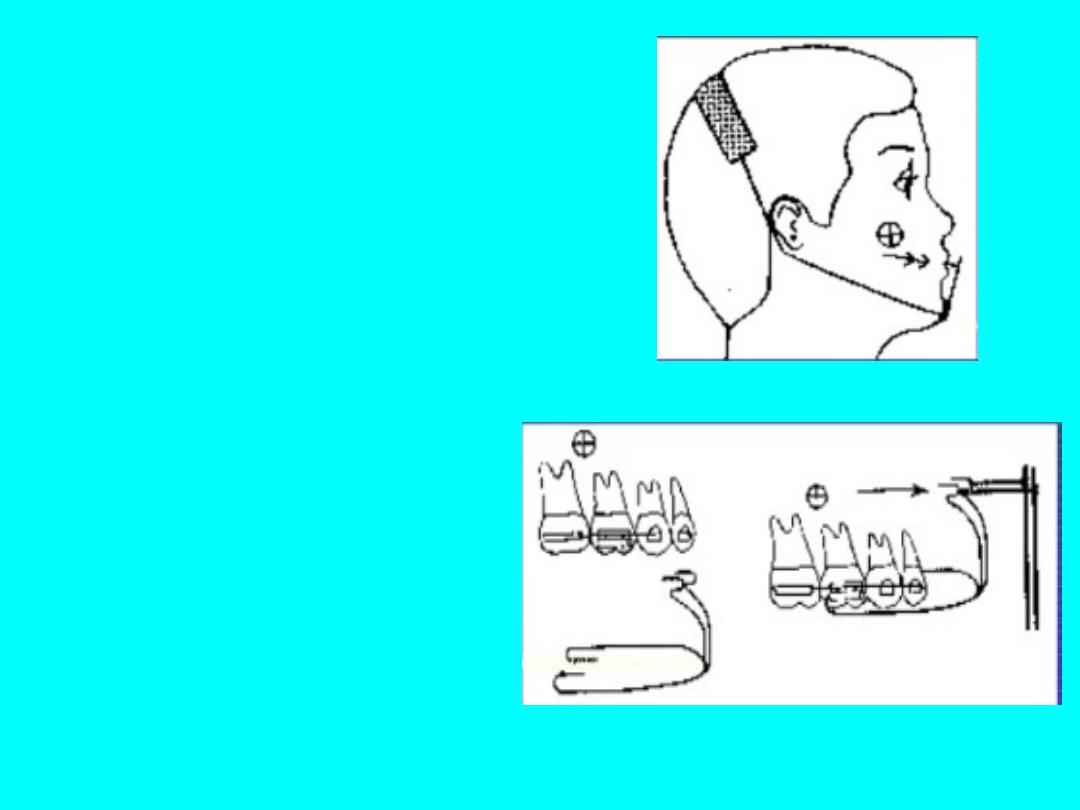
• Occipital headgear: it derives anchorage from
the back of head. It produces a distal and
superiorly directed force on the maxillary
teeth and maxilla.

• Treatment efects of the high-pull headgear
include
• intrusion and distalizaton of maxillary molars
• Ant-clockwise mandibular rotaton
• Decreased lower facial height

• Combinaton headgear: in this type of
headgear, occipital and cervical anchorage are
combined. when the forces exerted by both
are equel, a distal and slight upward force is
exerted on maxillary dentton and maxilla.

Other uses of headgear
1. Anchorage augmentaton: anchorage
reinforcement to prevent mesial movement
of maxillary molars.
2. Distalizaton of molars : for the correcton of
molar relatons or to gain space for correcton
of crowding or retracton of anteriors ( 300gm
perside). Also Unilateral molar distalizaton in
unilateral class II can be achieved by
asymmetric cervical headgear.

3. Molar rotaton
4. Space maintenance: the mesial movement of
molars is prevented to preserve the arch
length
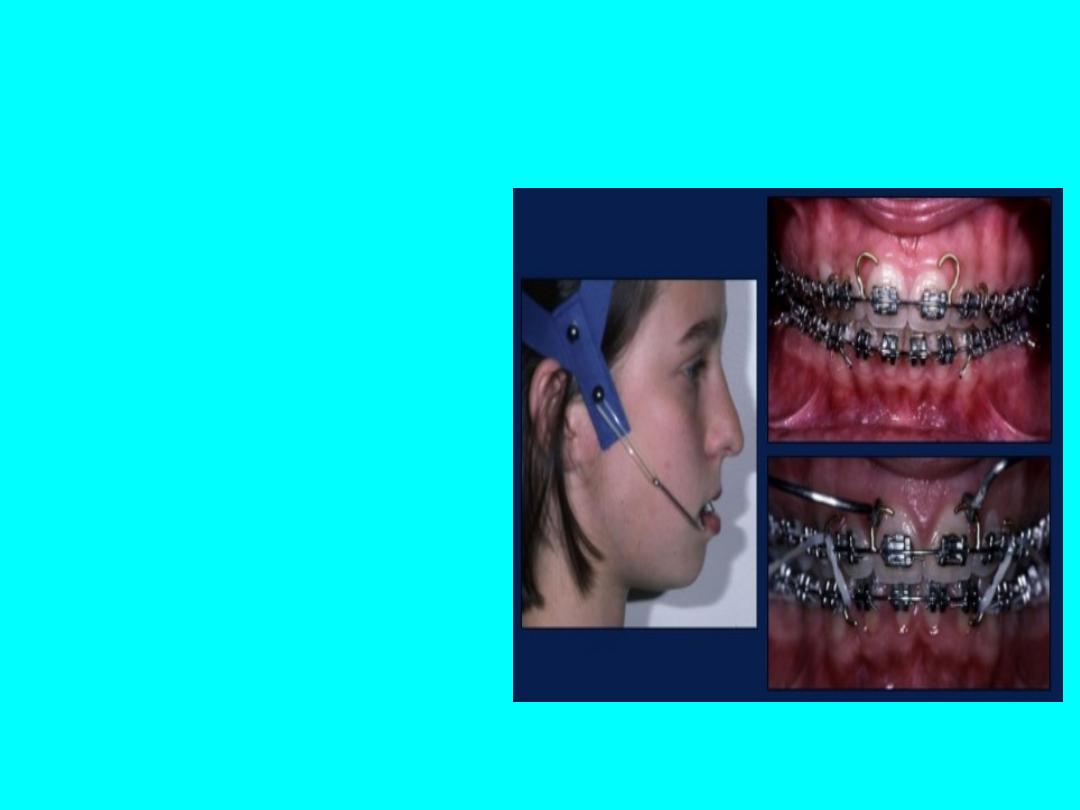
J hook headgear
J hook headgear
• The forces produced by
extraoral tracton also can
be atached anteriorly by
means of j-hooks to the
archwire or the hooks
soldered to the archwire.
Flared maxillary incisors can
be retracted using either a
high pull or a straight-pull
headgear combined with j-
hooks that are atached to
the arch wire anteriorly.

• J hooks can be applied to the maxillary teeth
in a variety of force vectors to retract and
intrude the maxillary incisor teeth.Usually
done in edgewise mechanotherapy
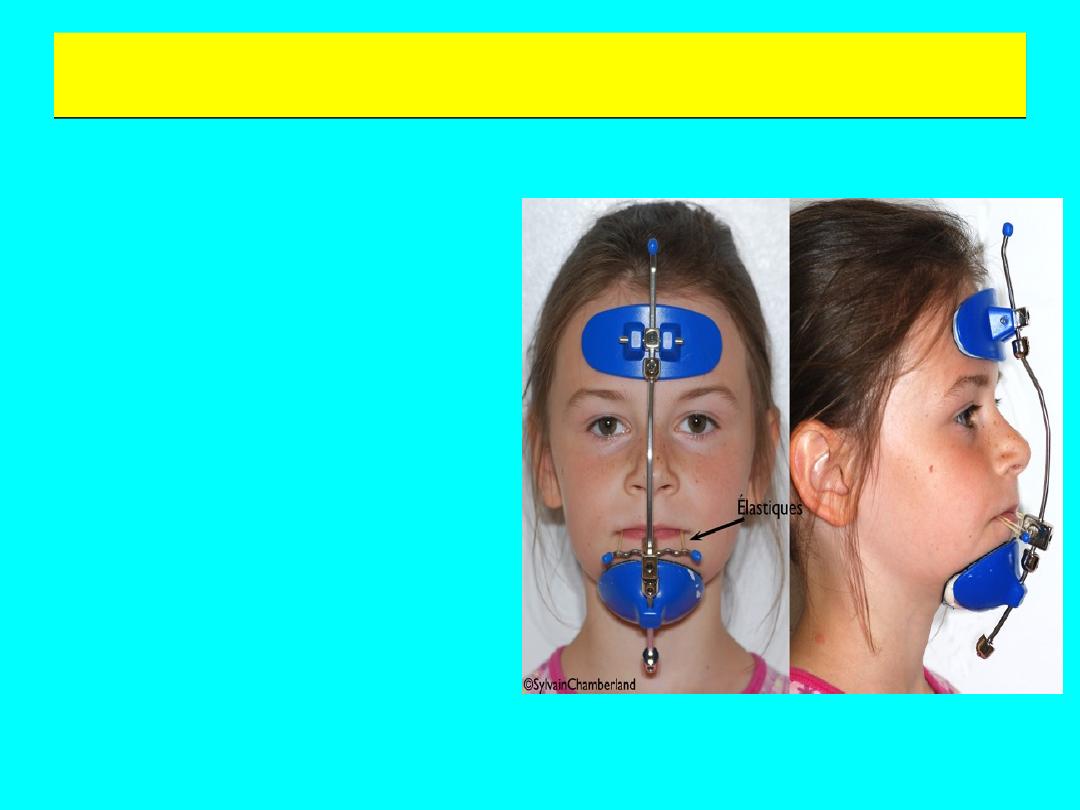
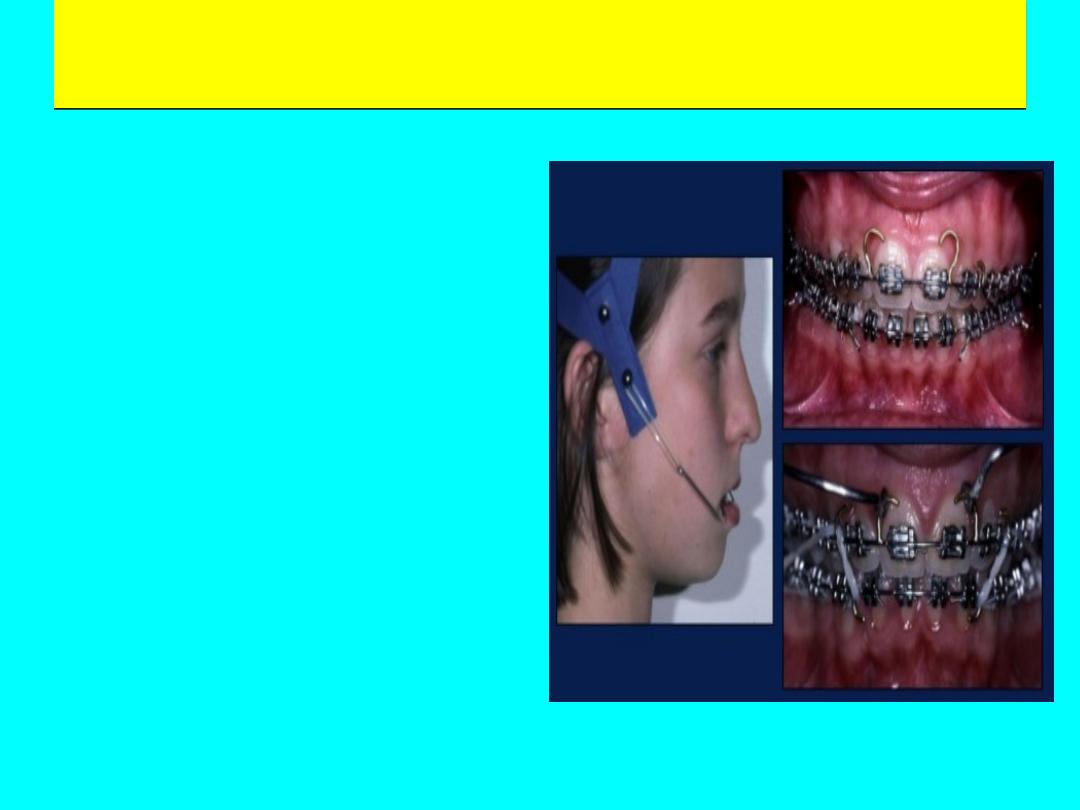
Reverse pull facial mask
Reverse pull facial mask
• Indicatons
1. Growing patents
having a prognathic
mandible and a
retrusive maxilla
( class III malocclusion)
2. For selectve
rearrangement of the
palatal shelves in clef
patents.

• Anchorage from chin & forehead : no
excessive force is exerted onto the condyler
growth cartlage. Disadvantage is difculty in
speech& compromise in aesthetcs & comfort.

• 1. Amount of force- the amount of force
required to bring about skeletal changes is
about 1 pound or 450 gms per side. 2.
Directon of force- 15 – 20 degree downward
pull to the occlusal plane to produce a pure
forward translatory moton of the maxilla. If
the line of force is parallel to the occlusal
plane, a forward translaton as well as an
upward rotaton takes place.

• 3. Duraton of force- tme taken to achieve
desired results is proportonal to the amount
of force utlized. 4. Frequency of use- 12 to 14
hours of wear a day

Parts of a reverse pull headgear
• 1.Chin cup : is used to take anchorage from the chin area. It can
be ready made or can be fabricated from an impression of the
patents gonial region. It is connected to the rest of the face
mask assembly by means of metal rods. 2. Forehead cap : use to
derive anchorage from the forehead. 3. Elastcs : used to apply a
forward tracton on the upper arch. Vertcal posts of the chin cup
are used to atach the elastcs onto the molar tubes or hook
soldered on the arch wire. It is purely for tooth movement. 4.
Intraoral appliance : tracton hooks are placed either in the
molar or premolar region. 5. Metal frame : It connects the
various components such as the chin cup and forehead cap. It
also has provision to receive elastcs from intraoral appliance.
• Also called as “protracton headgear”
• When an anterior protractory force is required, a
protracton headgear is used.
• Principle – pulling force on the maxillary structures with
reciprocal pushing force on the forehead or mandible
through facial anchorage.
• A reverse pull headgear basically consists of a rigid
framework, which takes anchorage from chin or forehead
or both for anterior tracton of maxilla using extra oral
elastcs that generate large amounts of force up to 1 kg or
more.
• 1. Protracton headgear by
Hickham : Uses the chin and top
of the head for anchorage. Force
distributon is – 15% head, 85%
chin. Consists of 2 short arms in
front of the mouth to engage
maxillary protracton elastcs. 2
long arms run parallel to the
lower border of the mandible &
go vertcally up from the angle of
the mandible and end behind
the ears. An elastc strap is
atached to the end of the long
arms to encircle the head.
Advantages – 1) beter aesthetcs
2) comfort 3) opton of unilateral
force applicability.

2. Face mask of Delaire:
Uses the chin and
forehead for support.
Appliance is made up of a
rigid wire framework,
which is squarish& kept
away from the face. It has
a forehead cap and a chin
cup with a wire running in
front of the mouth used
for elastc atachment.
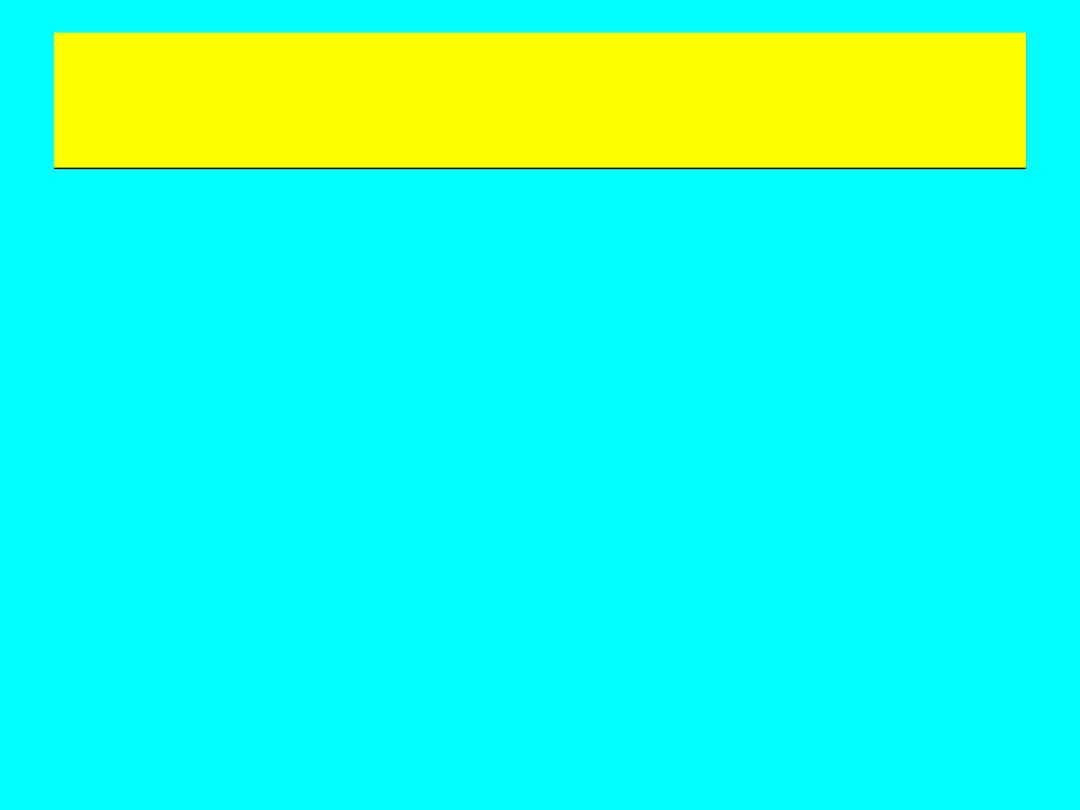
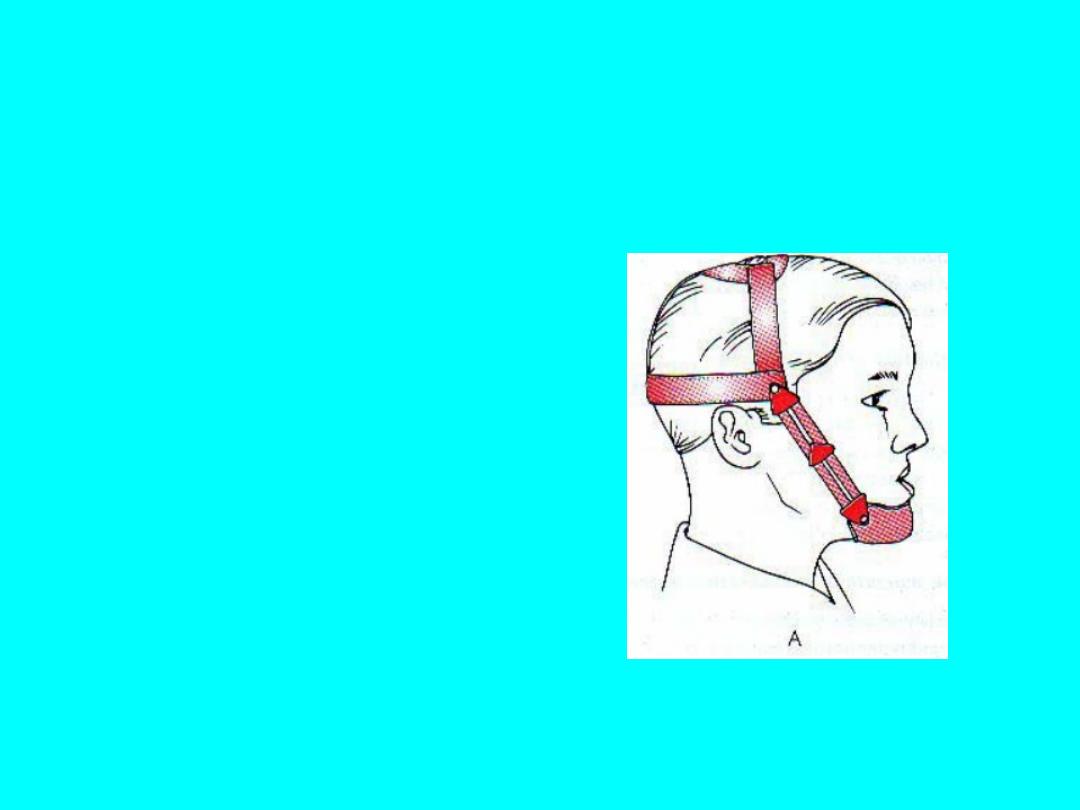
chin cap
chin cap
• It is an extra oral
orthopedic device that
covers the chin and is
connected to a head
gear. Used to restrict
the forward and
downward growth of
the mandible.
• 1) Occipital pull chin cup
• Derives anchorage from the
occipital and parietal region.
• Used in class III
malocclusions associated with
mild to moderate mandibular
prognathism.
• Also indicated in patents
with slightly protrusive lower
incisors as they invariably
produce lingual tpping of the
lower incisors.
• 2) Vertcal pull chin cup
• Indicated in patents
with steep mandibular
plane angle and
excessive anterior facial
height.
• These patents usually
exhibit an anterior open
bite.

• At the tme of appliance delivery a force of
150-300 grams per side is used. Over the next
2 months the force is gradually increased to
450-700 grams per side. The patent is asked
to wear the appliance for 12-14 hours a day to
achieve the desired results

Indicaton
• 1) Patents with mild skeletal prognathism of
the mandible.
• 2) In case of increased facial height.
• 3) Patents who has well aligned or protrusive,
but not retroclined mandibular incisors.