ORAL CANCERDR ASMAA
O
• Definition of cancer





• Uncoordinated and uncontrolled growth of the tissue, resulting from multiplication of its cells and the condition persists even after the stimulus or the initiating factor is removed.

Types of Intraoral Malignancies


















• Tumors originate from surface epithelium:
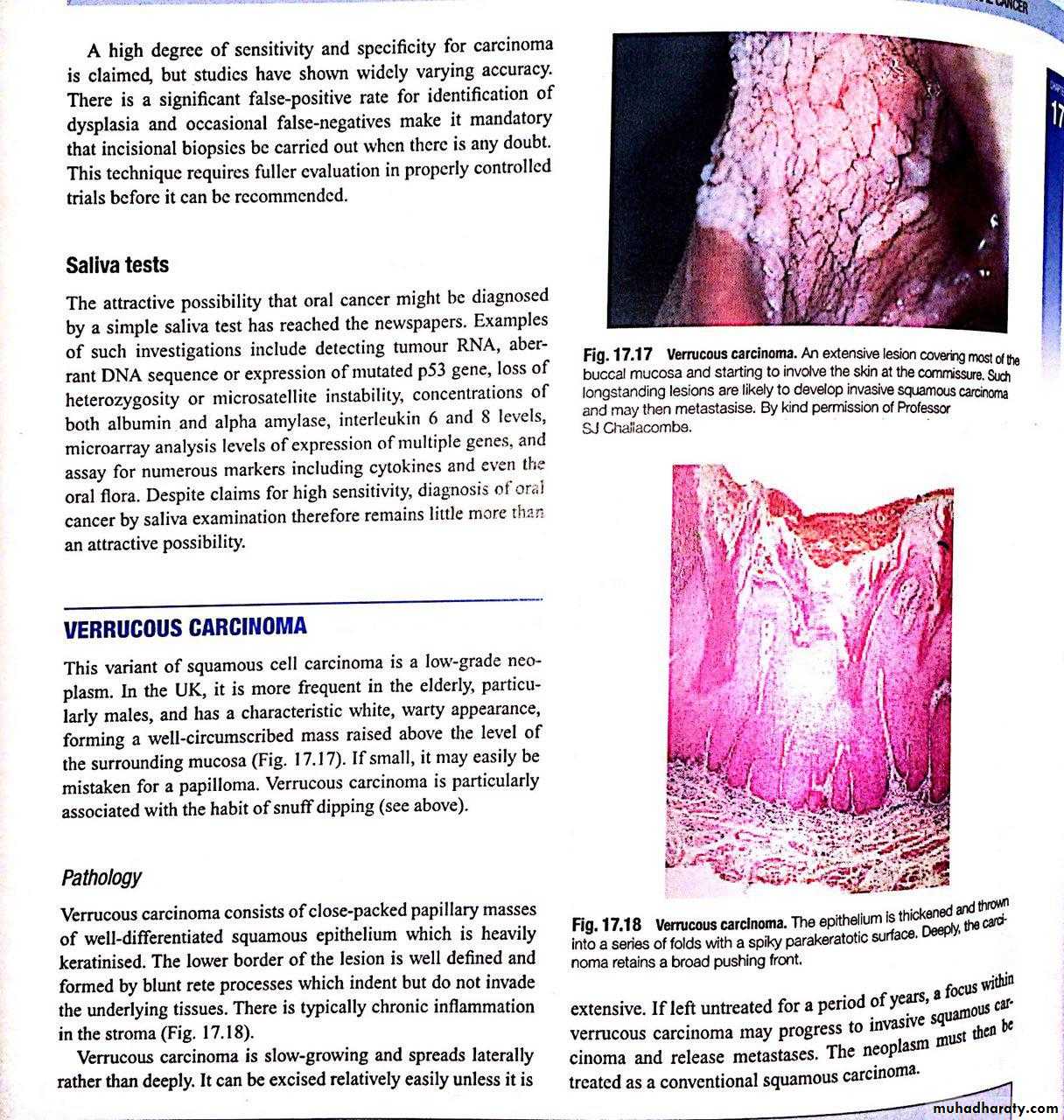
• Squamous cell carcinoma. Most common type (90-95 % )• Melanoma
• Tumors originate from glandular tissues (salivary glands , metastatic cancer from breast,prostate, lung ) :
• a.adenocarcinoma b.adenocystic carcinoma c.mucoepidermoid carcinoma
• Tumors originate from mesenchymal tissues :
• Sarcoma (osteosarcoma ,chondrosarcoma . fibrosarcoma,Ewing sarcoma )
• Lymphoma



















• Poor Dental Hygiene and Constant Chronic Trauma to Mucosa Due to Dental Cause Poor oral and dental hygiene, sharp teeth, ill fitting dentures, sharp crown and bridges, etc…
• Radiation (x-ray ,sunlight,UV light)
• Heriditary syndroms ( basal cell nevus syndrome , xeroderma pigmentosa )• Premalignant conditions (lichen plannus,teriary syphilis,leukoplakia, chronic candidiasis, Plumer –Venson syndrome)
• Malnutrition (vitamin deficiency )



• Spread of Squamous Cell Carcinomas of the Oral Cavity












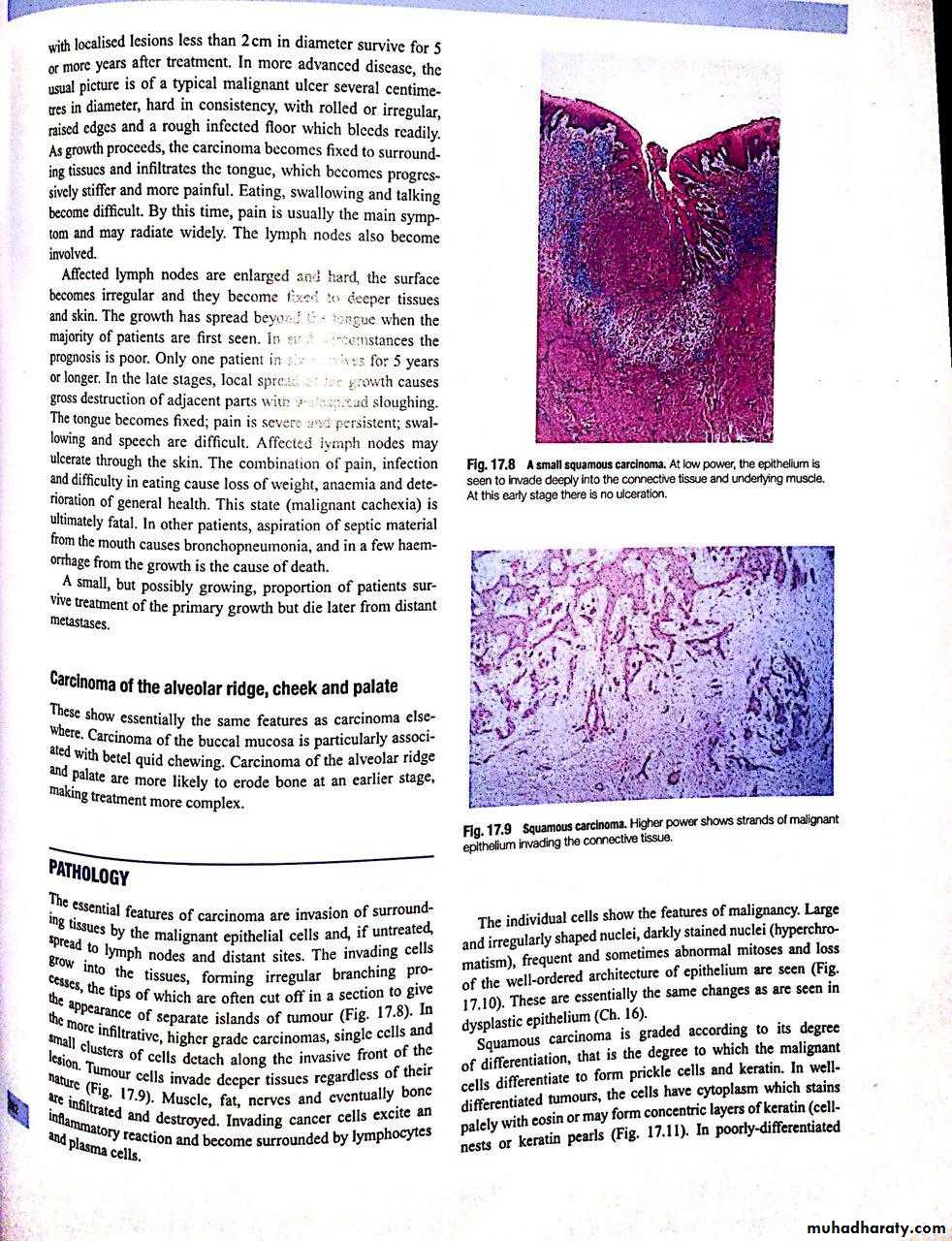
• A. Local infiltration
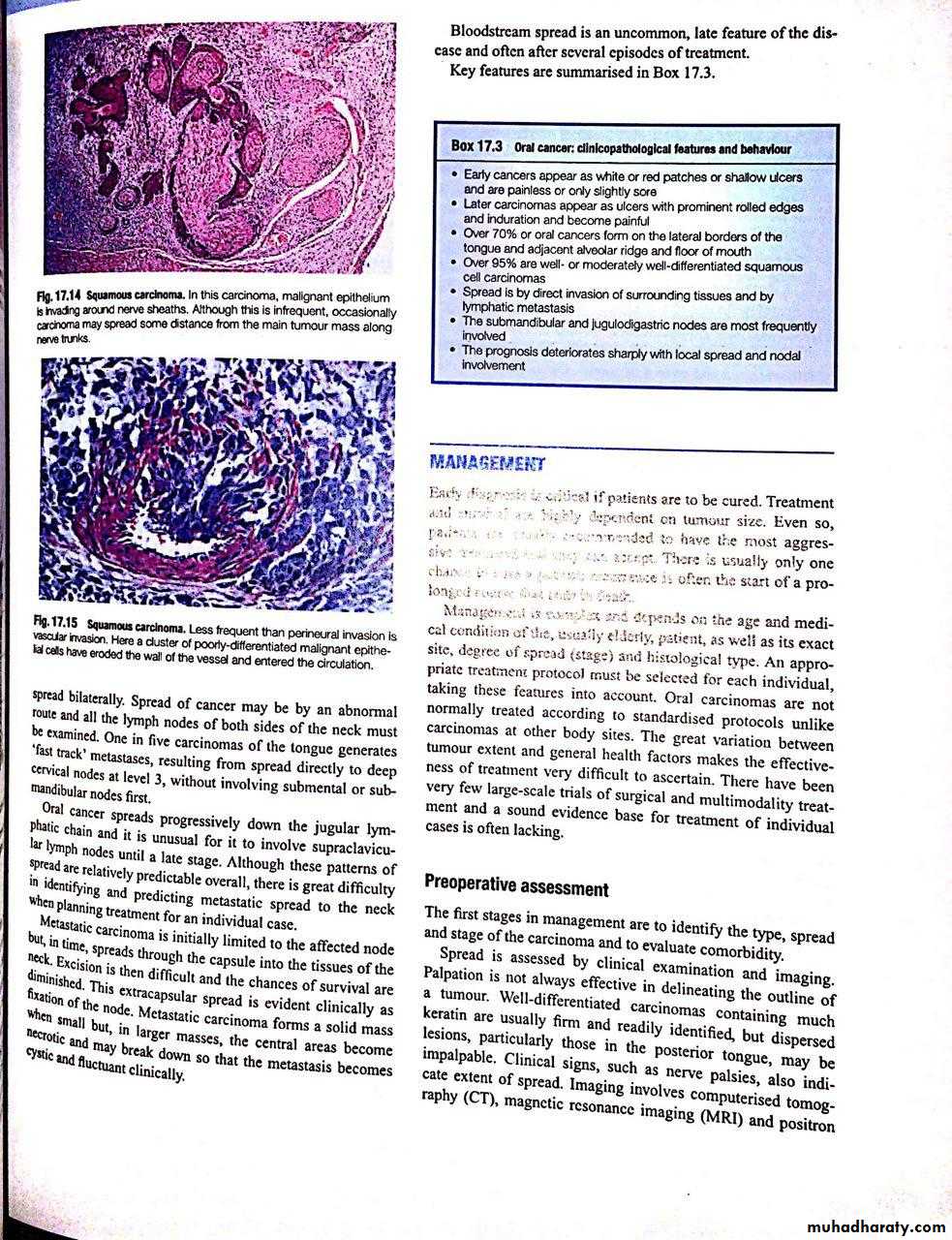
• 1. Invasion of local soft tissues.• 2. Invasion of perineural spaces.
• 3. Invasion of bone.
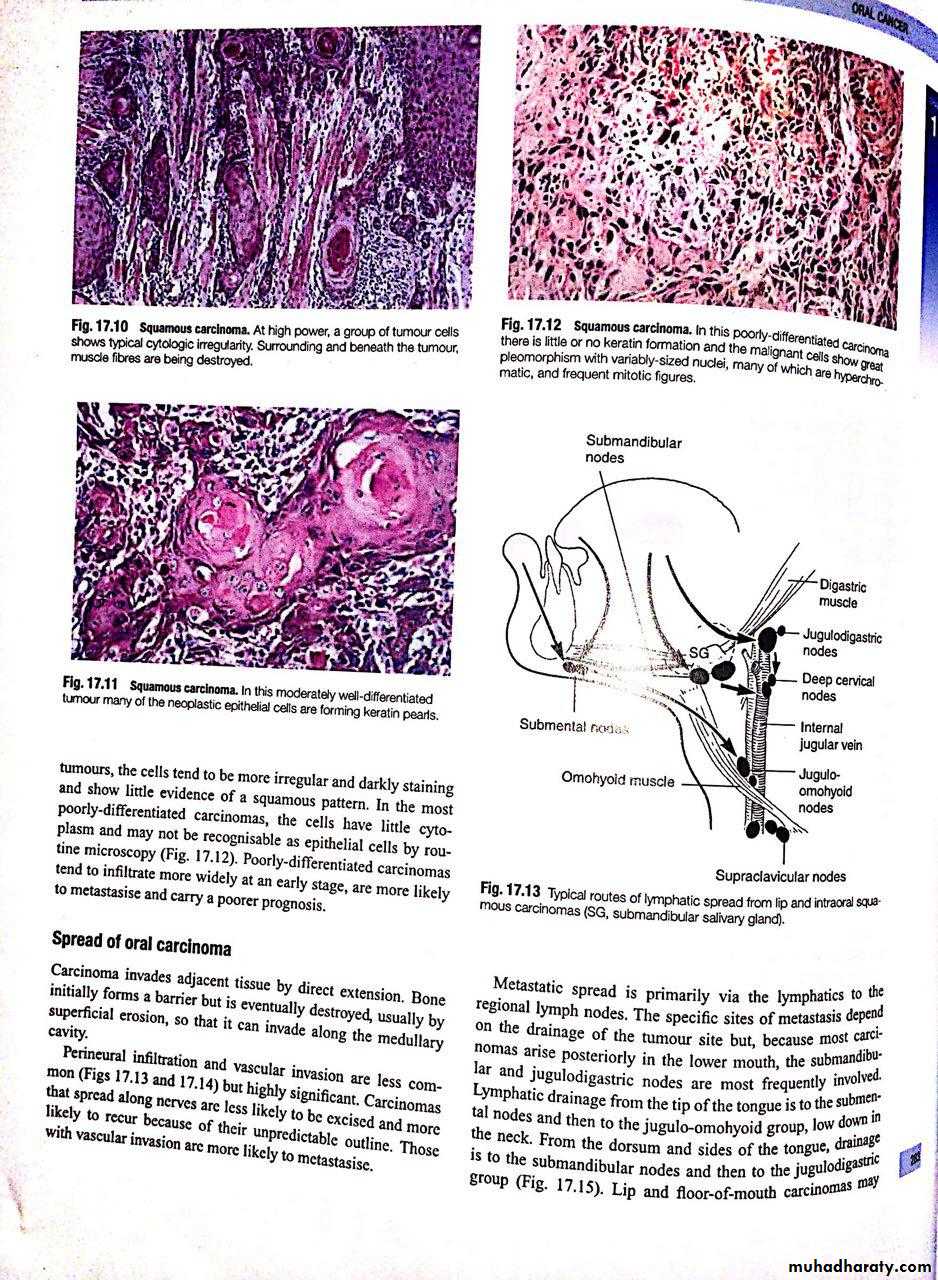
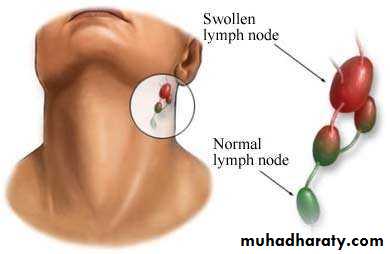
• Lymphatic Spread—Metastasis in regional lymph nodes.
• Blood borne metastasis (Distant spread)
Preoperative evaluation















• 1.History : include ;
• a.history of general health; chest pain, limited exercise tolerance• ,shortness of breath, anemia…
• b.history of the lesion(mass or ulcer ); onset of occurrence,duration, pain ….
• 2.Clinical examinations: a.extraoral examination ;
• inspection of head ,face ,neck for any asymmetry or changes in the color of the skin
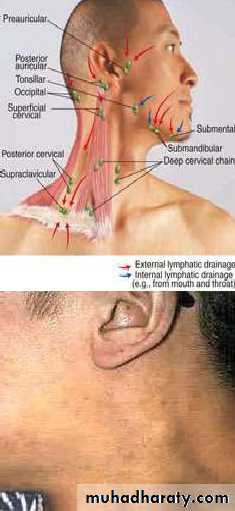
• examination of the regional lymph nodes bilaterally .
• b.intraoral examination; inspection and palpation of the tumor for checking borders, shape ,size , tenderness .














• radiographical examination; OPG, CT scan ,MRI for evaluation of primary site and regional lymph nodes (some times we need chest x-ray to exclude metastasis to the lung)..
• better imaging to assess bony involvement and extension are CT scan
• , while Imaging to assess extent of soft tissue spread and recurrent tumors are MRI .
• Laboratory investigations ;blood (Hb,Blood sugar, blood urea) ,
enzymes(liver function tests) ,electrolytes• 5.biopsy ;





















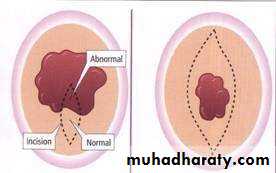
• a.Excision Biopsy ;When the lesion is small, it should be totally excised.
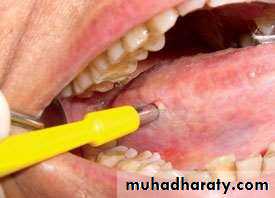
• b. Incision Biopsy;indicated in the large lesions or when complete excision is not possible• c. Aspiration Biopsy;If the lesion is deep seated, cystic or hemorrhagic aspiration biopsy should be done.In oral cancer its mostly usful in evaluation of enlarged lymph nodes
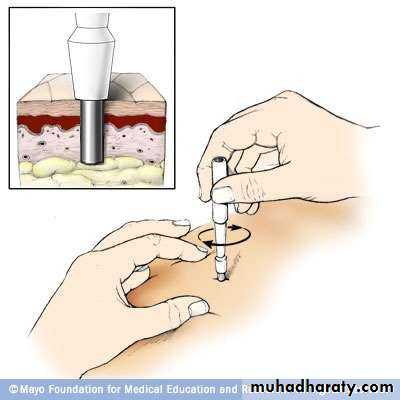
• d. Punch Biopsy;It is of limited value in the oral cavity. It is useful when small tissue specimen is to be taken from inaccessible areas e.g. the maxillary sinus, the lateral or posterior pharyngeal walls.
• Punch Biopsy
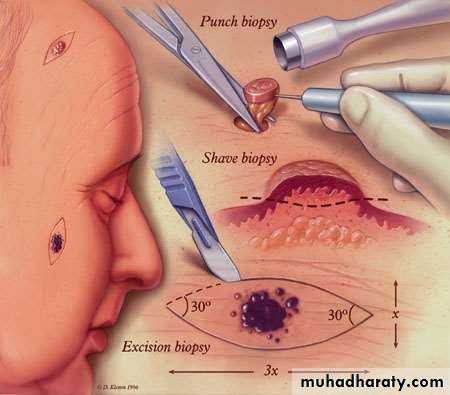
• Excisional biopsy


• Incisional biopsy

• Clinical Features of Oral Cavity Cancer














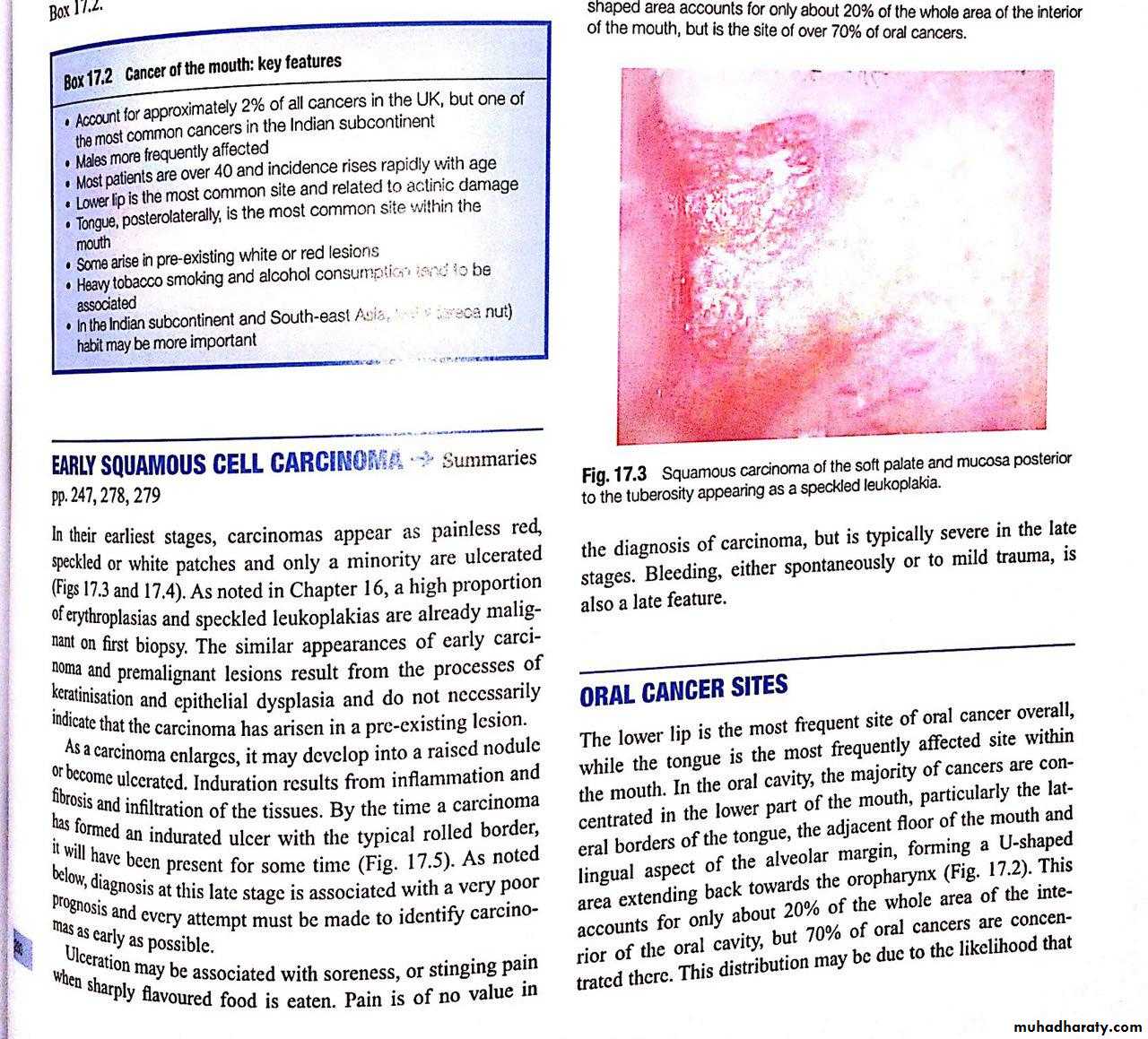
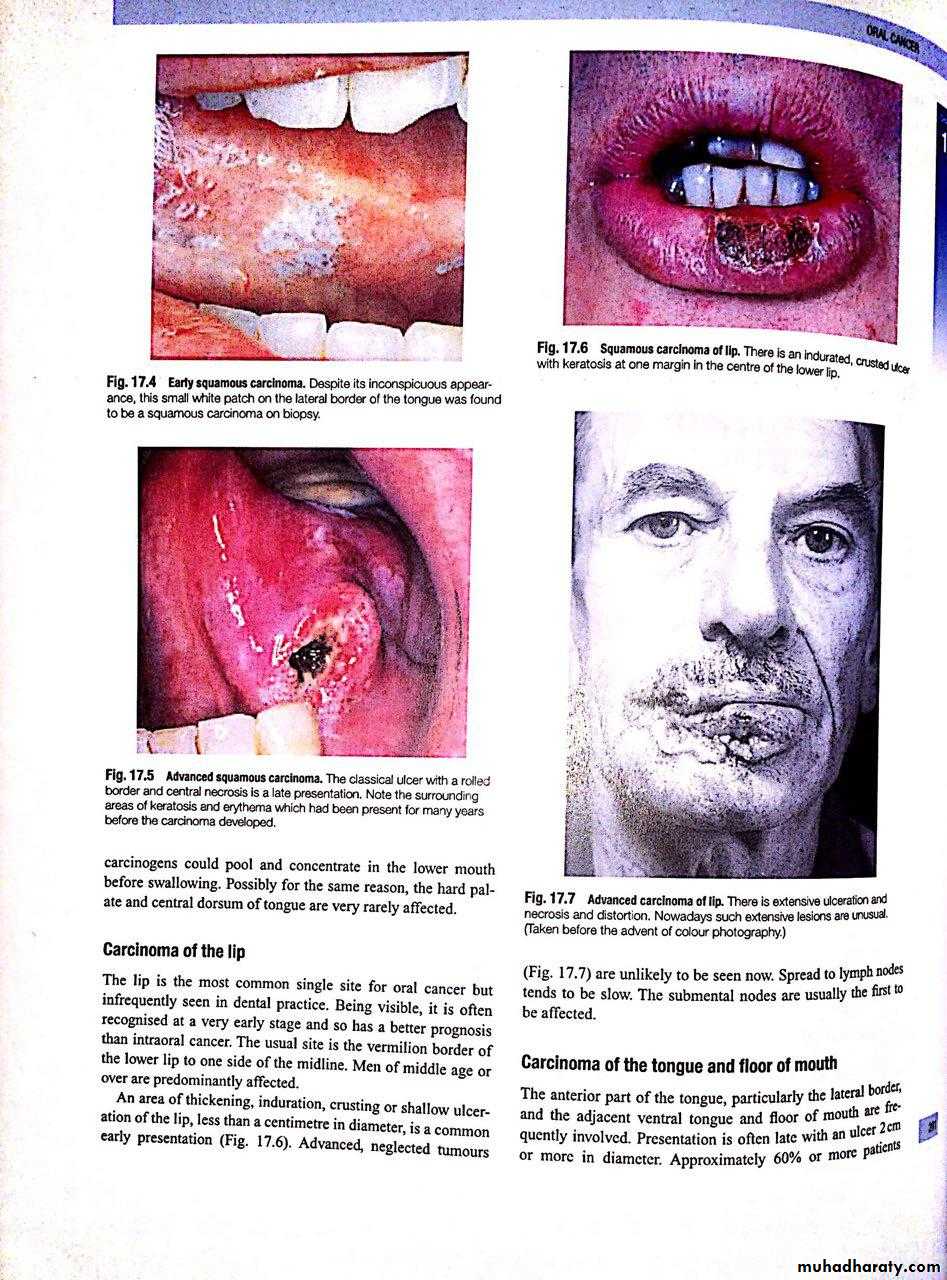
• Classically they present either as a non healing ulcer, with varying degrees of pain and occasional episodes of bleeding from the lesion usually have an irregular edge and induration of the underlying soft tissues.
• exophytic growth of duration may be several weeks to a few months before patient seeks treatment. Exophytic growth may present as a cauliflower like irregular growth or may be flat.
• More advanced lesions can present with pain, bleeding or fixity to surrounding structures.

















• Cancers that involve the infratemporal fossa present with recent onset of trismus. This must be distinguished from long standing trismus, which is a sign of oral submucous fibrosis.
• Lesions can also present with metastatic disease to the regional draining cervical nodes.
• It is important to remember that occasionally lesions of the alveolus in and around the non healing tooth extraction sockets can manifest with unexplained loosening of the involved teeth.
• Clinical Features of Oral Cavity Cancer
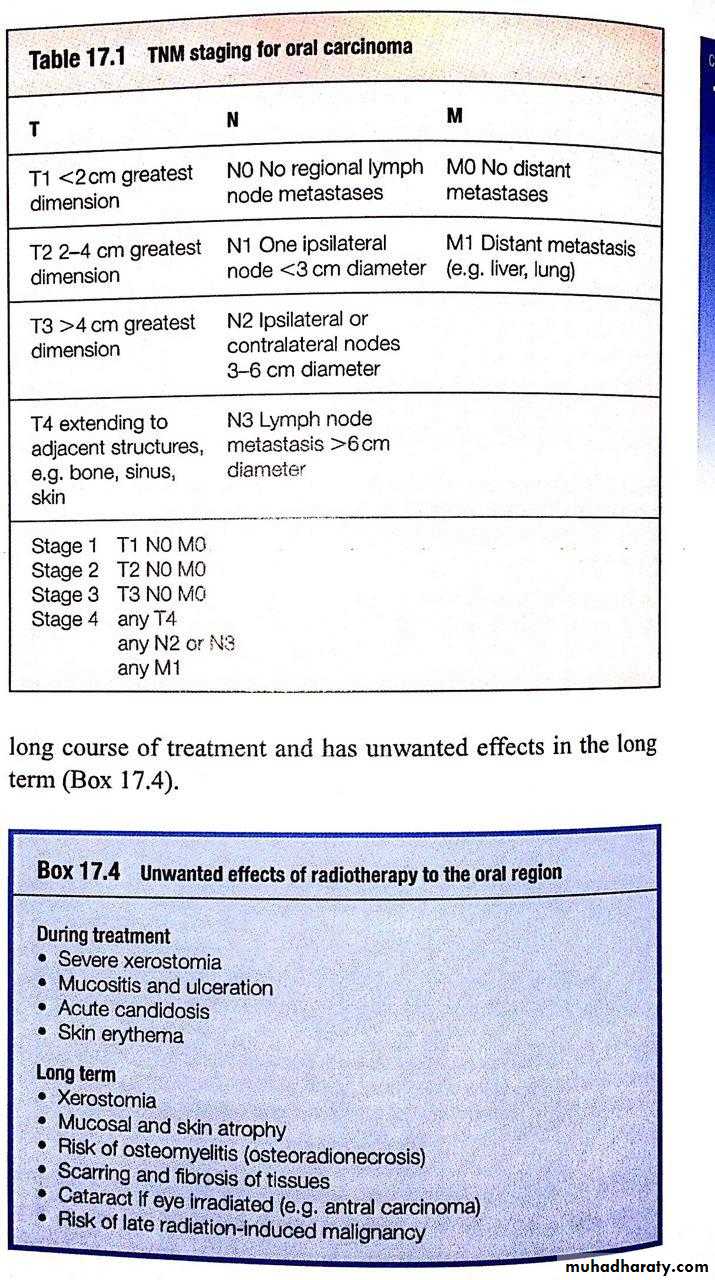
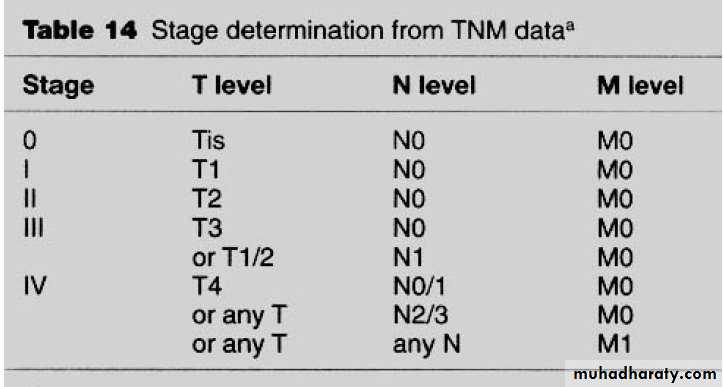
• TNM Staging













• Clinical staging system designed to express the severity, or extent, of the disease. It is meant to facilitate an estimation of prognosis and provide useful information for treatment decisions.
• T staging : tumor size (length and width but not depth)
• T0 No evidence of primary lesion• Tis Carcinoma in situ
• T1 Lesion 2 cm or less in the greatest diameter
• T2 Lesion > 2 cm but < 4 cm in the greatest diameter
• T3 Lesion > 4 cm in the greatest diameter
• T4 lesion invades adjacent structures (muscle ,bone, maxillary sinus ….).




















• N Staging : assess regional lymph nodes involvement
• N0 No regional LN metastasis• N1 Metastasis to a single ipsilateral lymph node <3 cm in greatest dimension
• N2 Metastasis in (a) a single ipsilateral lymph node 3-6 cm or (b) multiple ipsilateral lymph nodes < 6 cm or (c) bilateral or contralateral lymph nodes, < 6 cm
• N3 Metastasis in a lymph node more than 6 cm
• M stage
• M0 no distant metastasis
• M1 distant metastasis present

• Histological grading :
• It represent the degree of resembles of tumor cells to the• original cells
• it determine the aggressiveness of tumor
• Well differentiated (have nearly same shape of normal cells
• ,produce keratine ,less mitotic activity) is the least aggressive one while undifferentiated (not resemble the original cells, high mitotic activity, not produce keratine) is the most aggressive tumor• Histologic grade (G)
• G1• Well differentiated
• G2
• Moderately differentiated
• G3
• Poorly differentiated
• G4
• Undifferentiated
• Management of oral cancer











• Treatment modalities for oral cancer involve :
• 1.surgery• 2.radiotherapy
• 3.chemotherapy
• 4.additional treatment modalities : immune therapy, photodynamic therapy
• Surgery is the preferred treatment of choice , radiotherapy is reserved for patients who are not willing for surgery or when surgery will cause significant cosmetic or functional defects or if patients are unfit for general anaesthesia.


















• Advantages of Surgery
• Fast
• Repeated procedures possible
• Cost effective Disadvantage of surgery
• Esthetic alteration
• Inability to precisely eliminate foci of microscopical lesion
• relatively high incidence of complications (infection,orocutanous fistula etc….)











• Advantage of Radiotherapy
• 1.minimal esthetic and functional alteration 2.ability to sterilize microscopical tumor cells• Disadvantages of Radiotherapy 1.Ineffective to ablate large tumor volume 2.Acute and chronic morbidity 3.Prolonged treatment
• 4. Not suitable for treatment if lesion involves or is close to the bone

















• Selection the modality depends upon the stage of cancer at
• diagnosis. The broad guidelines are as follows:• Early stage oral cancer (Stage I and II) can be treated with single modality treatment. Surgery or radiotherapy .
• advanced cancers (Stage III and IV) need to be treated with combined modality treatment (surgery and radiotherapy).
• Some cases tumor are consided inoperable(not indicated for surgery and should be treated palliatively (chemotherapy and /or radiotherapy)
• Criteria for considering tumor inoperable
• Recent onset of trismus (gross infratemporal fossa invasion)
• Base of skull involvement
• Distant metastasis

• Management of the Neck Lymph Nodes















• Involvement of regional lymph nodes by oral cancer is dependant on following factors:
• Site and location of primary lesion , tongue and floor of the mouth lesions show more increased risk of nodal metastasis than hard palate lesion• Size of primary site
• T stage ,increasing stage will increase the risk of nodal
• metastasis, irrespective to site.
• Histomorphologic feature, poorly differentiated carcinoma have increased risk of metastasis than well differentiated carcinoma.


• Surgical treatment ; neck dissection (radical ND, modified ND , Selective ND) for surgical clearance of all involved lymph nodes and those suscepected to be involved .
• Radiotherapy

• Management of the Neck Lymph Nodes

• Principles of Reconstruction










• Mucosal Defects can be Delt with Following Modalities :
• Leave raw areas, allow it to heal by granulation tissue (secondary intentions).• Primary closure
• Cover with skin graft
• Coverd with flap.

• Reconstruction of bony defects






• Bony defects can be reconstructed using external materials (alloplasts like plates, silastic implants etc.), allografts (cadaveric bone) or autografts.

• Survival and Prognosis :







• The stage of disease at presentation is the most important factor. Stage I and II disease has better prognosis( 5 yr. survival 31-100%) whereas advanced stages III, IV have poor prognosis( 5 yr. survival 7-41%)
• Role of Dental Practitioner in Oral Cancer Management













• Prevention and early detection—It is important for practicing dentists to examine the entire oral cavity when performing routine dental care to pick up suspicious lesions.
• Dental care prior to commencing radiation—this is very important and involves oral prophylaxis,fluoride application, extract hopeless teeth and restore carious teeth.
• Patient education post radiotherapy to maintain good oral health
• Maxillofacial prosthesis fabrication—both intra and extra- oral prosthesis can be fabricated to replace teeth, nose, ear and eye, etc.