Group c
Tutorial
NO.1
د
.
ضياء
12/10/2017
Chest pain
Failure to recognize potentially serious conditions such as:
acute Ischemic heart disease.
aortic dissection.
tension pneumothorax.
pulmonary embolism .
can lead to serious complications, including death.
Conversely, overly conservative management of low-risk patients
leads to unnecessary hospital admissions,tests, procedures, and
anxiety .
Chest pain
a common presentation of:
cardiac disease.
respiratory dis.
musculoskeletal dis.
GIT problem.
a manifestation of anxiety .
Causes of chest pain:
Cardiac
• Myocardial ischaemia (angina) or MI.
• Pericarditis.
• Mitral valve prolapse.
Aortic
• Aortic dissection.
• Aortic aneurysm.

Oesophageal
• Oesophagitis.
• Oesophageal spasm.
• Mallory–Weiss syndrome.
Lungs/pleura
• Pulmonary embolism. Pulmonary infarct
• Tracheitis.
• Pneumonia
• Pneumothorax.
• Malignancy.
• Tuberculosis.
• Connective tissue disorders.
Musculoskeletal
• Osteoarthritis.
• Rib fracture/injury. Intercostal muscle injury
• Costochondritis (Tietze’s syndrome).
• Epidemic myalgia ,(Bornholm disease).
Neurological
• Prolapsed intervertebral disc
• Herpes zoster
• Thoracic outlet syndrome .
Anxiety/emotion
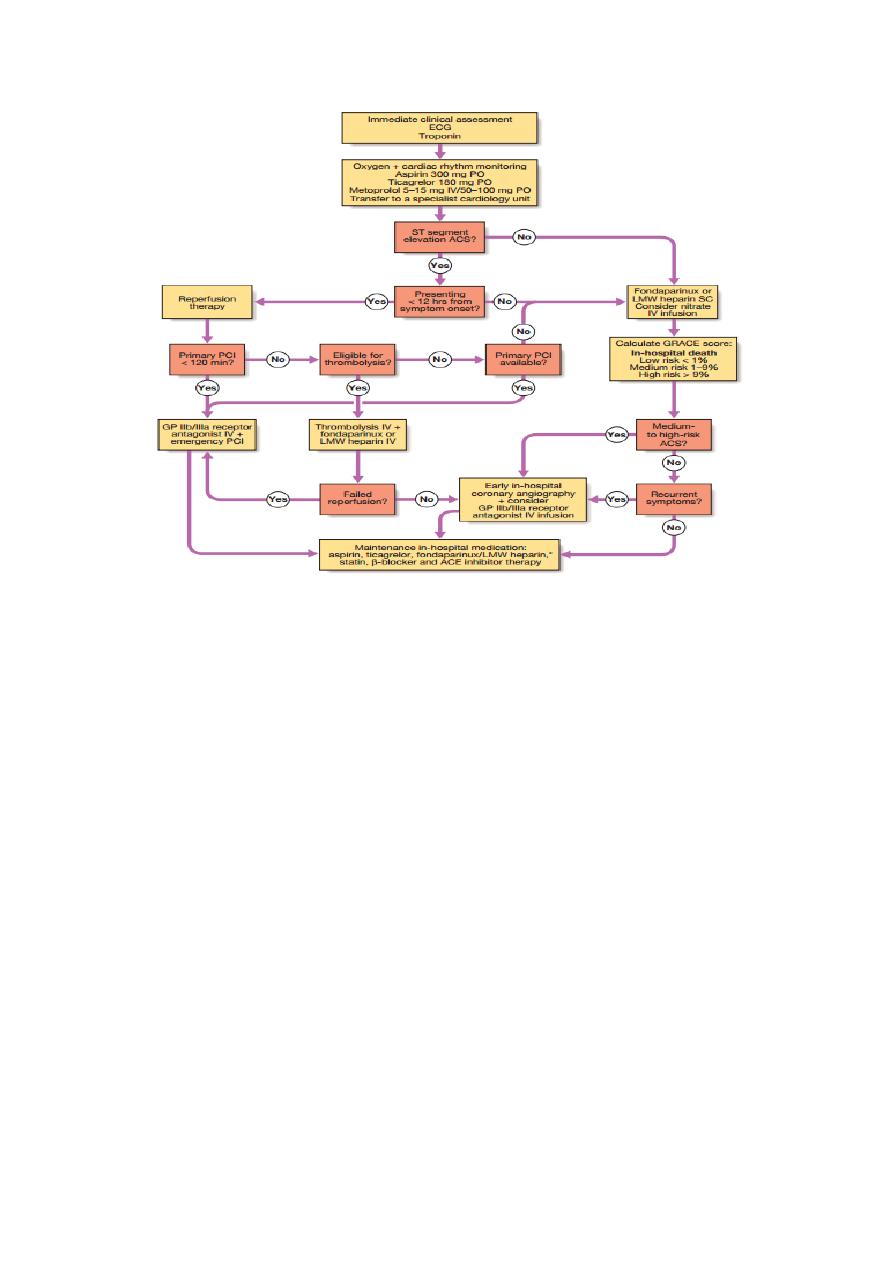
Initial evaluation of suspected cardiac pain
the evaluation of the patient with chest discomfort must
accommodate two goals
determining the diagnosis a
assessing the safety of the immediate management plan.
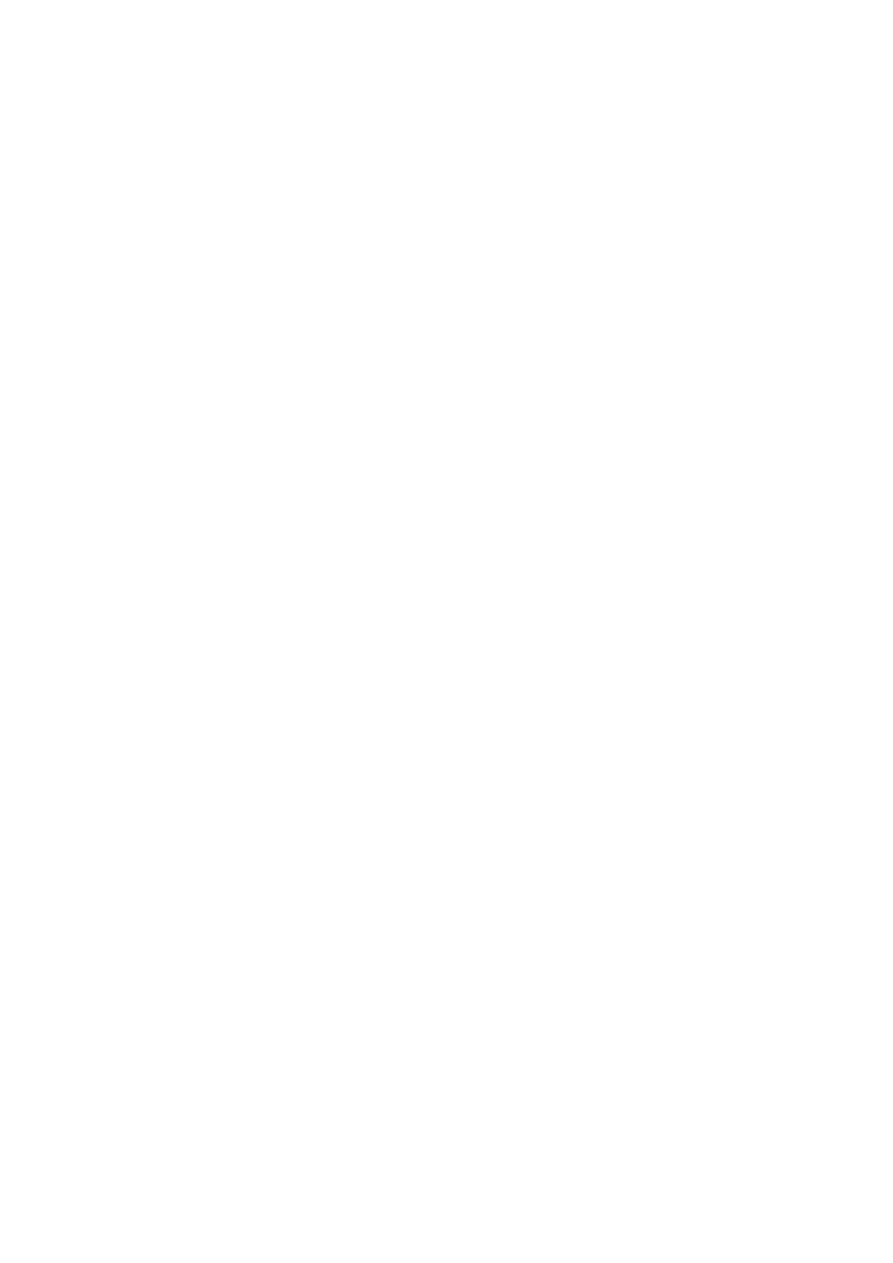
classification of chest pain:
typical,
atypical
non-cardiac chest pain,
based on the balance of evidence .
the clinician must focus first on identifying patients who require
aggressive interventions to diagnose or manage potentially life-
threatening conditions, including
acute ischemic heart disease,
acute aortic dissection,
pulmonary embolism,
tension pneumothorax .
If such conditions are unlikely, the clinician must address questions
such as:
the safety of discharge to home,
admission to a non-coronary care unit facility, or
immediate exercise testing.

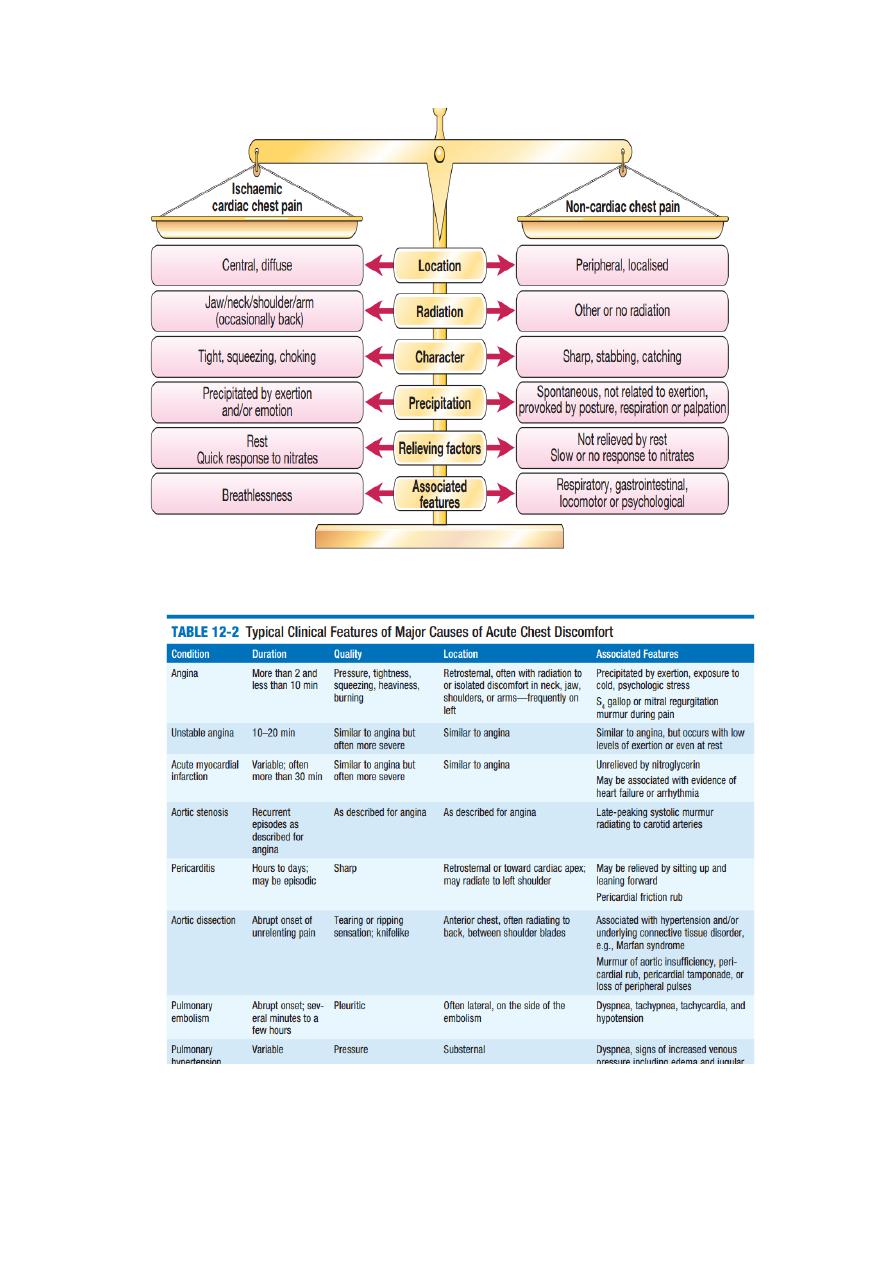
Considerations in the Assessment of the Patient With Chest Discomfort
1.
Could the chest discomfort be due to an acute, potentially life
threatening condition that warrants immediate hospitalization and
aggressive evaluation?
Like Acute ischemic heart disease P E, Aortic dissection or
Spontaneous pneumothorax.
2
. If not, could the discomfort be due to a chronic condition likely to
lead to serious complications?
Stable angina,Aortic stenosis,Pulmonary hypertension
3.
If not, could the discomfort be due to an acute condition that
warrants specific treatment?
Pericarditis,Pneumonia/pleuritis or Herpes zoster.
4
. If not, could the discomfort be due to another treatable chronic
condition?
Esophageal reflux, Cervical disk disease,Esophageal spasm, Arthritis
of the shoulder or spine,Peptic ulcer disease Costochondritis
Gallbladder disease Other musculoskeletal disorders or Other
gastrointestinal conditions Anxiety state
ACUTE CHEST DISCOMFORT:
In patients with acute chest discomfort, the clinician must first
assess the patient’s respiratory and hemodynamic status .
Include focused history, physical
examination, and laboratory evaluation should be performed to
assess the patient’s risk of life-threatening conditions .

The history:
the history should include questions about
the onset,site, duration and quality of the chest discomfort .
Angina,AMI is usually associated with a gradual intensification of
symptoms over a period of minutes.
radiation of chest pain increases probability that pain is
due to myocardial infarction. Radiation of chest pain to the left
arm is common with acute ischemic heart disease, but radiation to
the right arm is also highly consistent with this diagnosis.
Epigastic region
Referred pain
Pain situated over the left anterior chest and radiating laterally is
unlikely to be due to cardiac ischaemia
The pain of aortic dissection
, massive
pulmonary embolism or pneumothorax
is usually very sudden or
instantaneous in onset.
Pain of AMI
increase over a time
The physical examination:
should include evaluation of blood pressure in both arms and of
pulses in both legs. Poor perfusion of a limb may be due to an
aortic dissection that has compromised flow to an artery
branching from the aorta.
Chest auscultation may reveal diminished breath sounds; a
pleural rub; or evidence of pneumothorax, pulmonary embolism,
pneumonia,or pleurisy.
Tension pneumothorax may lead to a shift in the trachea from the
midline, away from the side of the pneumothorax.
The cardiac examination should seek pericardial rubs, systolic and
cardiac murmurs, and 3
rd
or 4
th
heart sounds.
Ligh Pressure on the chest wall may reproduce symptoms in
patients with musculoskeletal causes of chest pain.
Investigations:
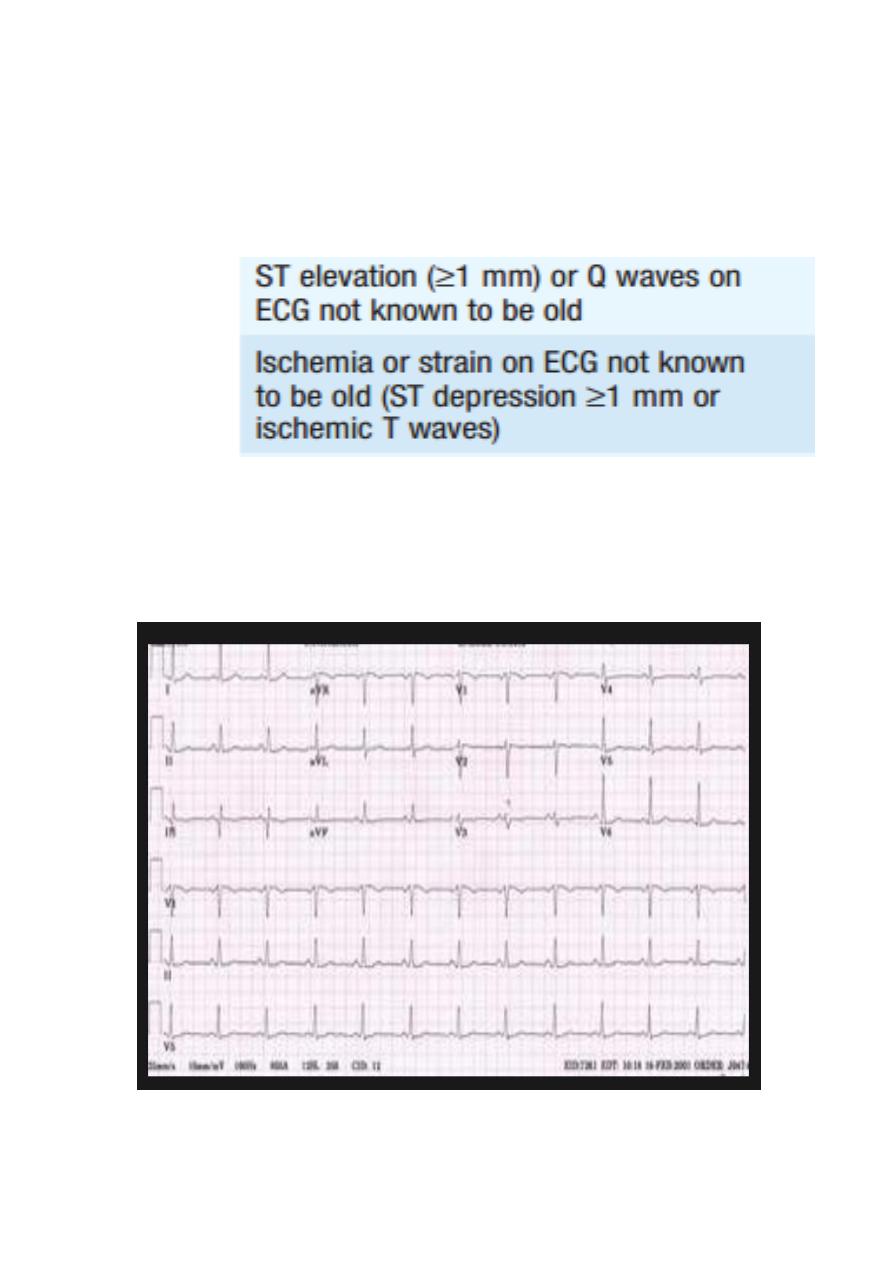
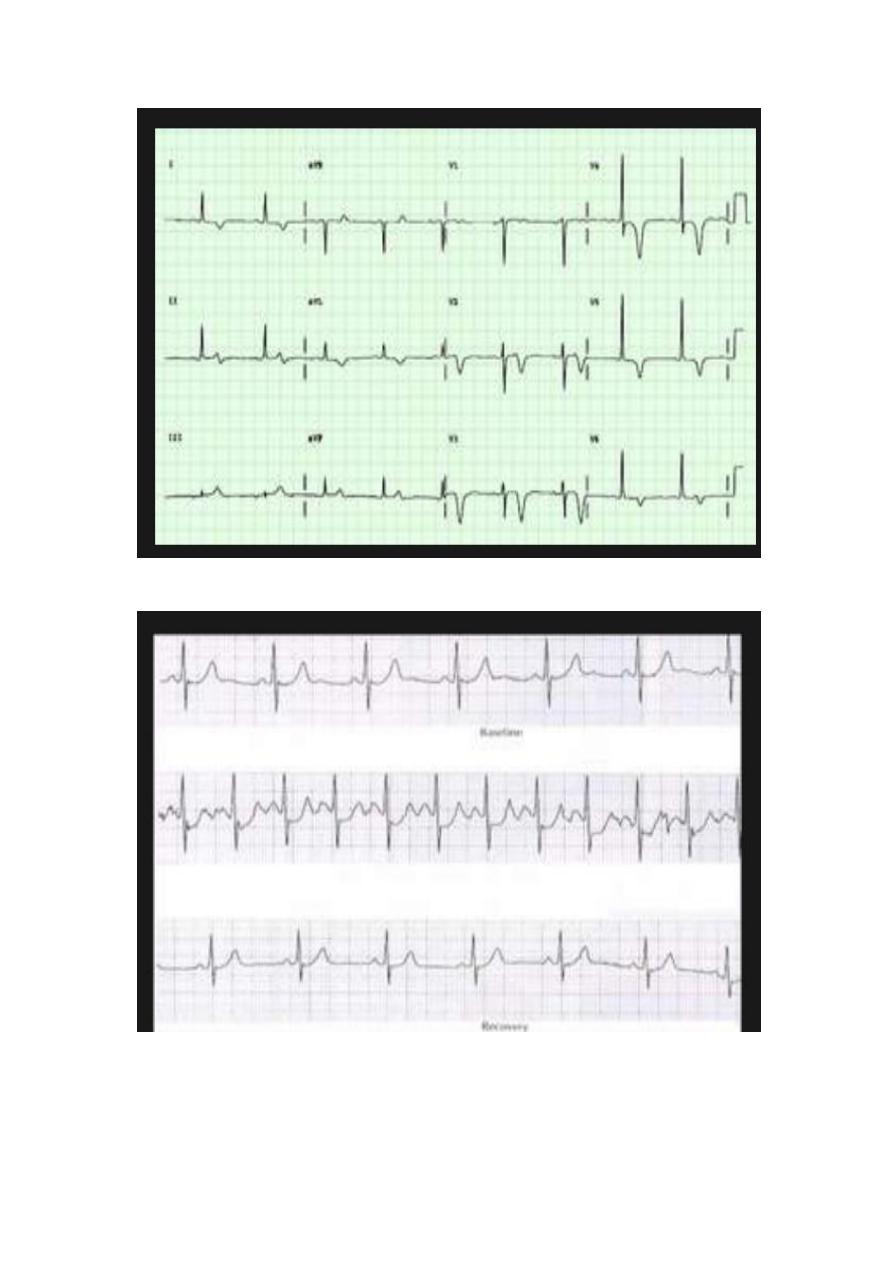
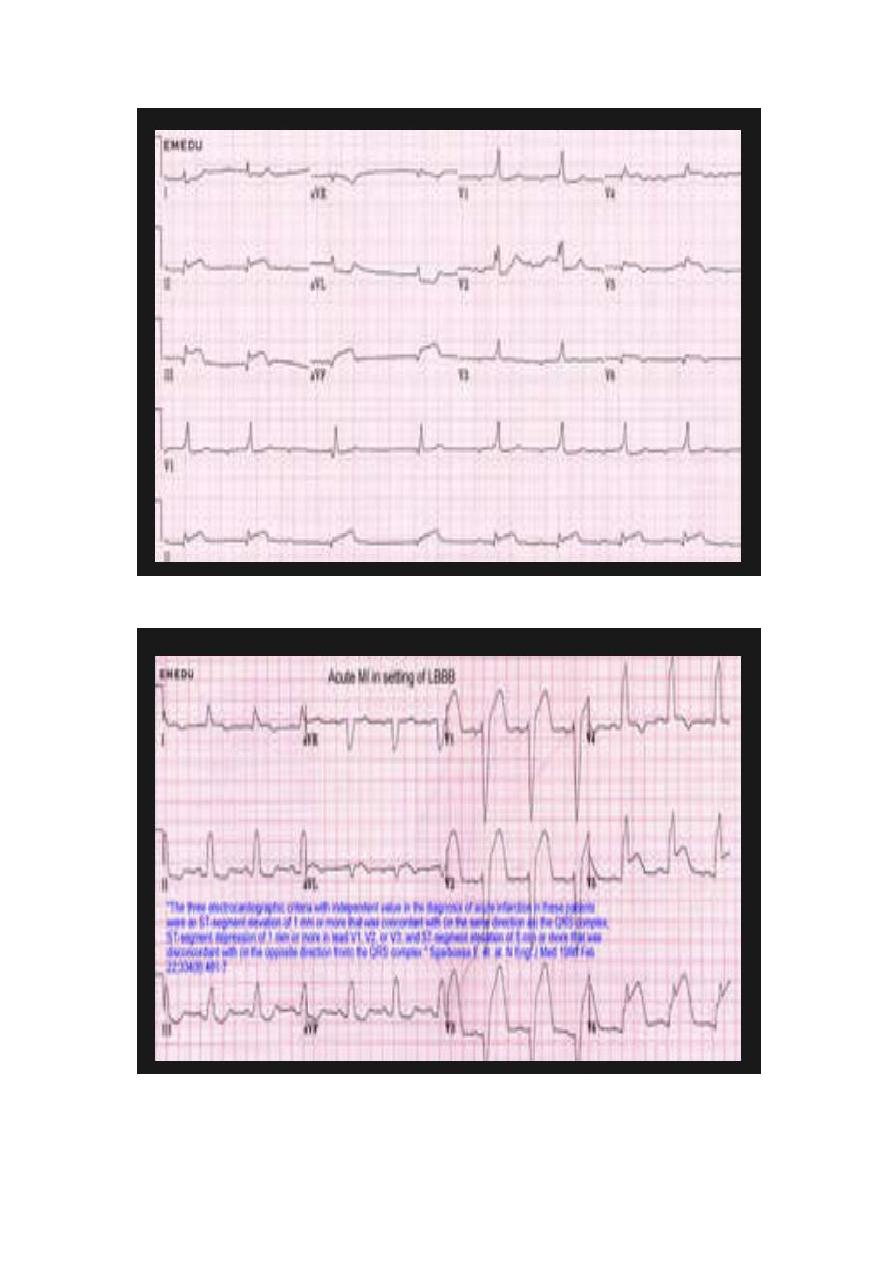
An ECG is an essential test for adults with chest discomfort.
The electrocardiographic changes consistent with ischemia or
infarction include:
T
h
e
E
C
G
changes are associated with high risks of acute myocardial
infarction or unstable angina .
The absence of such changes does not exclude acute ischemic
heart disease.
Cardiac markers:
Markers of myocardial injury are often obtained in the emergency
department evaluation of acute chest discomfort include cardiac
troponins (I and T).
decisions to discharge patients home should not be made on the
basis of single negative values of these tests.
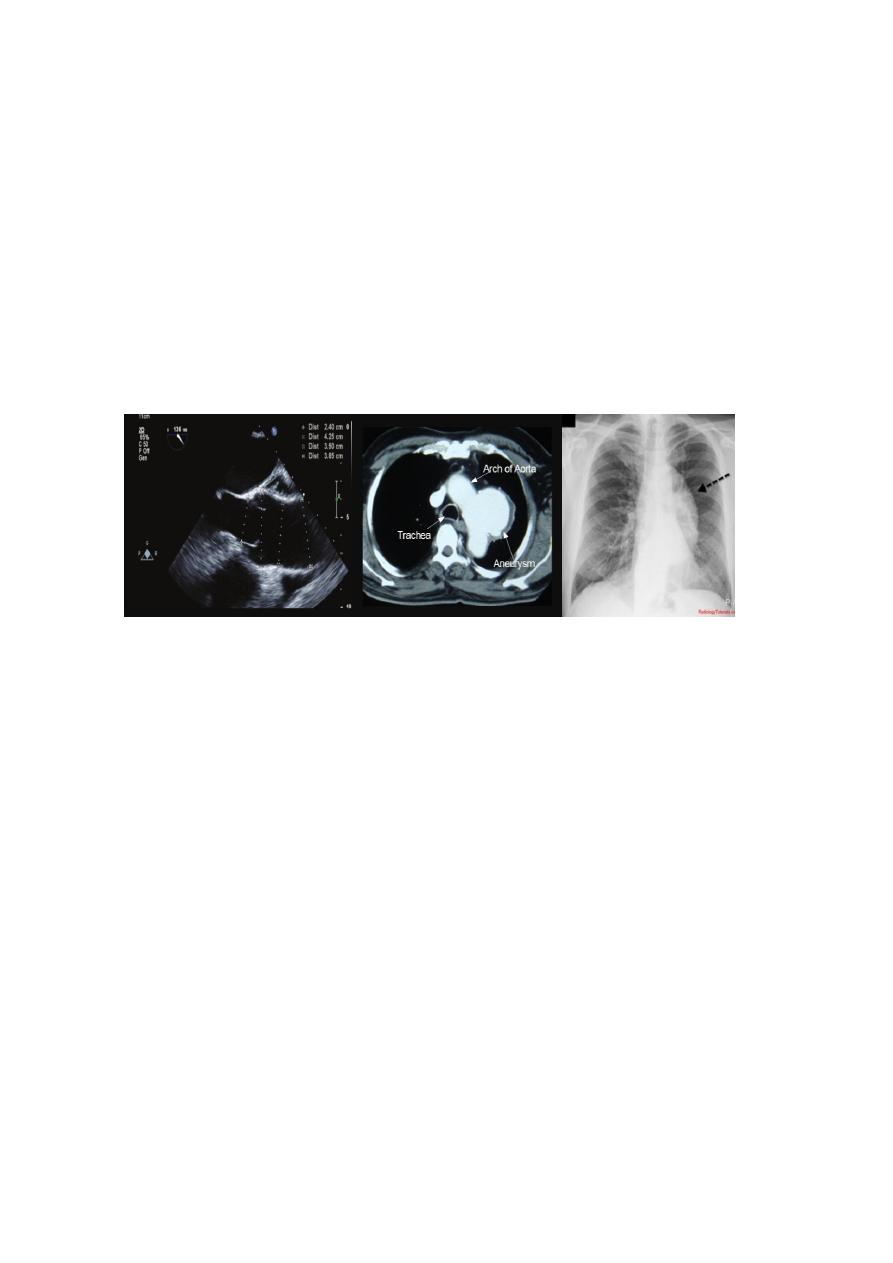
If the patient’s history or examination is consistent with aortic
dissection, imaging studies to evaluate the aorta include a chest CT
scan with contrast, MRI, or TE.
Pulmonary embolism:
ECG.
CXR,
ECHO.
D dimer
CT angio