Salivary gland disease
Dr. Wafaa Khalil
Types :-
Major salivary glandsParotid glands
Submandibular(submaxilary)glands
Sublingual glands
Minor salivary glands
Distributed throughout the oral cavity except dorsal surface of the tongue and attached gingiva
Effect of saliva:
Aid in swallowingDecrease in caries rate
Aid in chewing
Aid in talking
Digestion (Amylase, lipase)
Antibacterial (Lysozyme, IgA, peroxidase)
Buffer (HCO3)
The Salivary glands secrets saliva which contains the enzyme amylase (protein of molecular wt. 50,000. Containing calcium which splits starch and glycogen into maltose) all the secretory activity is regulated mainly by parasympathetic nerves.
FUNCTIONS:
The total salivary secretion is between 1,000 ml – 1,500 ml daily and is almost all the result of stimulation.

Deficiency of the saliva cause dry mouth (xerostormia)
eg: Dehydration, Sjogren’s syndrome, atropine which blocks the action of parasympathetic nerves on the glands.Deficiency

Evaluation of the SALIVARY GLANDS Diseases:
• a. History: Age, pain, swelling, duration etc..• b. Clinical Examination: Position (site), colour, temperature, tenderness, shape, surface. Edge, composition, relation, lymphatic drainage.
• c. Investigations:
• I. Blood (CBC), Hb, Urea and Electrolytes, Blood Sugar etc..
• II. Constituents of saliva in inflammatory diseases. The sodium increased while the phosphate level is decreased. The albumin usually very low but increased in Sjogren’s diseases, also antibodies can be demonstrated.

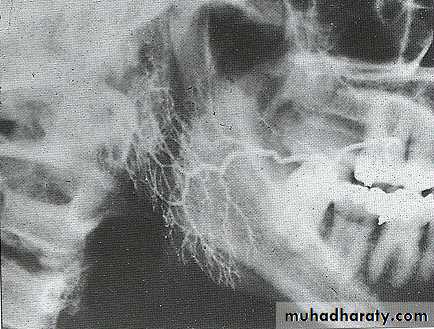
• III. Radiology:
• a) Plain X-ray (20% of salivary calculi are non-opaque to X-rays)• b) Sialogram
• Radiology is helpful in the diagnosis of;
• Calculi
• Degree of glandular damage in obstruction
• Duct strictures
• Duct fistulas and sialoceles

• IV. Ultrasound distinguishes solid tumour from the rare cyst and sialocates.
• V. CAT scanning has definite place in the assessment of deep parotid tumours.
Classification:
• 1. Acute swelling• Mumps
• Sialoadenitis
• 2. Recurrent swelling
• Sialo-angiectasis or punctate sialectasis
• Papillary obstruction:
• Acute (ulcerative)papilary obstruction
• Chronic (fibrotic)papillary obstruction
• Relative papillary obstruction
• Ductal obstruction due to:
• Causes in the lumen• Causes in the wall
• Causes outside the wall
• Gland distension
• The effect of drug
• An ellergic reaction
• 3. Persistent swelling:
• Benign tumour
• Malignant tumour
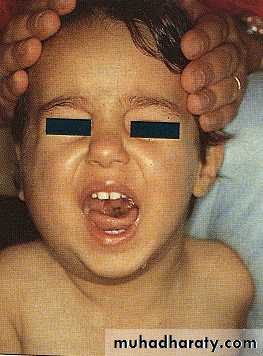
Mumps:
• Its avirus infection affect mainly the parotid gland
• Its usually bilateral swelling or unilateral
• Sign and symptom:
• Swelling behind the ear
• Tender to palpation
• Pain in area during meal, eating, talking,and smelling
• Slight elevation of body temp.
• Child become less energetic
Treatment:
Bed restIsolation of child
High nutritioning food
AB to prevent 2ry infection
Acute sialoadenitis
• Etiology:-• Usually occur behind an obstruction of main duct
• Dehydrated patient
• Debilitated patient
• Patient expose to radiation
• Sign & symptoms :-
• Swollen of gland
• Very tender
• Painful
• Odema of surrounding soft tissue
• Inflammation or redness of soft tissue
• Pus discharge from the duct opening
• Increase body temp.
• Swelling increase during eating,talking………ect.
After surgical operation
Treatment:-
AB (tetracyclin)Vit-c lozenges
Incision & drainage by Helton’s method
Recurrent swelling:-
• It occurs with 2 type of periodicity• Appear when a flow of saliva is stimulate by thought, sight,smoking,or taste of food
• Appear at intervals of week due to attacks of ascending infection
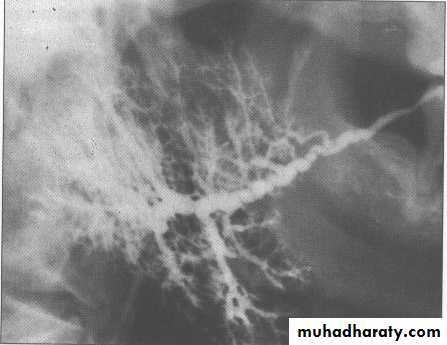
• Sialo-angiectasis or punctuate sialoectasis:
• etiology:
• Unknown
• Autoimmune condition
• It’s a part of sjogren’s syndrome
• developmental
Raidographical feature:
• There are stricture and dilatation of ductal tree.it has aproximal cavities in the sialograph.• Clinically:
• 1ry (acute) condition
• 2ry condition
• Rx:-
• AB (penecilline)
• Sugar- free chewing gum
• May curred after sialography
• Secondary condition:
• Occures in patient expose to radiation
• Patient has chronic infection
• Sjogren’s syndrom
• Cavities are larger &irregular in shape with multiple fibrosis of duct of s.g.
(streptococci virdans)
• Papillary obstruction:
• Mainly occur in parotid gland• Acute ulcerative papillary obstruction
• Occurs as a result of an ulcer in papillae which cause obstruction of parotid gland .
• Etiological factor is trauma
• Rx :removal of the causative agent the condition subside by it self when the ulcer is heal
• b. Chronic fibrosis papillary obstruction
• It’s a gradual decrease of salivary flow according to the amount of fibrosis in the papillae which may reach complete closure of duct opening.
• Cause is trauma.
• Treatment: need several visit to the clinician to dilate the stricture of papillae.
• papillotomy is done by creation a new opening in mucosa distal to the original one.
c.Relative papillary obstruction
It occur when there is thick saliva which unable to excreted freely from the opening of the parotid gland duct.treatment:
Vit. C . Lozenges
Sugar free chewing gum
Frequent massage of the gland
wharton’s duct
stensen’s duct