1
Course: Clinical Analysis
Lecturer: Dr. Weam Saad
Lecture: Urine
Urine
1- Urine Analysis
Urine analysis usually used for identify diseases like urinary tract
infections, diabetes glomerulonephritis and others. Urine should be collected at
any time of day in clean containers during midstream.
Fresh urine is better to be
examined as quickly as possible. The time from collection to examination in the
laboratory is an important factor and should not exceed 1 hr. increase in time
can make the followings:
1) Decreased clarity due to crystallization of solutes
2) Rising pH.
3) Loss of ketone bodies.
4) Loss of bilirubin.
5) Dissolution of cells and casts.
6) Overgrowth of contaminating microorganisms.
A. Visual observation:
The first step is direct visual observation. Normal, fresh urine is dark
yellow or amber in color and clear. Normal urine volume is 750 to 2000
ml/24hr. Turbidity or cloudiness may be caused by excessive cellular material
or protein in the urine or may develop from crystallization or precipitation of
salts upon standing at room temperature or in the refrigerator.
Clearing of the specimen after addition of a small amount of acid
indicates that precipitation of salts is the probable cause of turbidity. A red or
red-brown (abnormal) color could be from a food dye, eating fresh beets, a
drug, or the presence of either hemoglobin or myoglobin. If the sample
contained many red blood cells, it would be cloudy as well as red.

2
B. Biochemical Tests:
pH:
The normal range is from a pH of 7.4 to 6.
Specific Gravity (sp gr):
Some laboratories measure urine density
which is the ability of the kidney to concentrate or dilute the urine, many
laboratories use refractometer instrument for specific gravity, and normal
range between 1.002 and 1.035, any measurement below this range
indicates hydration and any measurement above it indicates to dehydration
or high levels of glucose.
Protein:
It is better to do tests for urine protein on the supernatant of
centrifuged urine since the cells suspended in normal urine can produce a
falsely high estimation of protein. Normally, only small plasma proteins
filtered and can be found in normal urine. Normal total protein excretion
does not usually exceed 150 mg/24 hours or 10 mg/100 ml in any
specimen. More than 150 mg/day is defined as proteinuria.
Also, detection of protein by production of color with an indicator dye,
Bromphenol blue, which is most sensitive to albumin, and precipitation by
heat is a better method. The sulfosalicylic acid test is a more sensitive
precipitation test. It can detect albumin, globulins, and Bence-Jones protein
at low concentrations.
Glucose:
Normally there is small amount of glucose in urine; Glycosuria
(excess sugar in urine) generally means diabetes mellitus. The glucose
oxidase reaction used for glucose detection but can miss other reducing
sugars such as galactose and fructose. For this reason, most newborn and
infant urines are routinely screened for sugars by other methods like
Benedict's copper reduction test.
Ketones:
Ketones (acetone, aceto-acetic acid, beta-hydroxybutyric acid)
resulting from either diabetic ketosis or starvation), are easily detected
using tablets containing sodium nitroprusside.
Nitrite:
A positive nitrite test indicates that bacteria may be present in
significant numbers in urine. Gram negative rods such as E. coli are more
likely to give a positive test.

3
Leukocyte Esterase: Detects the presence of white blood cells either as
whole cells or as lysed cells.
C. Microscopic Urine Analysis:
Method:
A sample of well-mixed urine (usually 10-15 ml) is centrifuged in a test
tube at low speed (about 2000-3000 rpm) for 5-10 minutes until button is
produced at the bottom of the tube. The supernatant is discarded and a volume
of 0.2 to 0.5 ml is left inside the tube. The sediment is suspended in the
remaining supernate by flicking the bottom of the tube several times. A drop of
resuspended sediment is poured onto a glass slide and covered with coverslip.
Examination:
The sediment is first examined under low power to identify most crystals,
casts, squamous cells, and other large objects. The numbers of anything found
is per low power field (LPF). Since the number of elements found in each field
may be different from one field to another, several fields must be examined.
The Second examination at high power to identify types of crystals, cells, and
bacteria. The number is usually described as the number of each type found per
high power field (HPF). Example: 1-5 WBC/HPF.
Sediments can be found during microscopic examination:
1- Red Blood Cells:
The presence of abnormal numbers of red cells in urine due to:
glomerular damage, tumors, kidney trauma, urinary tract stones, renal infarcts,
acute tubular necrosis, upper and lower urinary tract infections, nephrotoxins,
and physical stress. Red cells may also contaminate the urine from the vagina in
menstruating women (during bleeding) or from trauma produced by bladder
catherization. Normally no red cells should be found, but some find their way
into the urine, if one or more red cells can be found in every high power field
that can be considered as abnormal.
4
2- White Blood Cells
The presence of abnormal numbers of leukocytes that may appear with
infection in either the upper or lower urinary tract or with acute
glomerulonephritis. Usually, the WBC's are granulocytes. White cells from
the vagina, especially in the presence of vaginal and cervical infections, or
the external urethral meatus in men and women may contaminate the urine.
If two or more leukocytes per each high power field (HPF) appear in non-
contaminated urine, the specimen is abnormal. Leukocytes have lobed nuclei
and granular cytoplasm.
3- Epithelial Cells
Renal tubular epithelial cells, usually larger than granulocytes, contain a
large round or oval nucleus and normally found in small numbers, with
nephrotic syndrome and in conditions leading to tubular degeneration, the
number is increased.
4- Lipids:
The presence of lipid cells, these cells contain endogenous fat and called oval
fat bodies.
5- Casts
Urinary casts are formed only in the collecting duct (distal nephron). Casts
can be seen in glomerular injury cases due to increased glomerular permeability
to plasma proteins causing proteinuria.
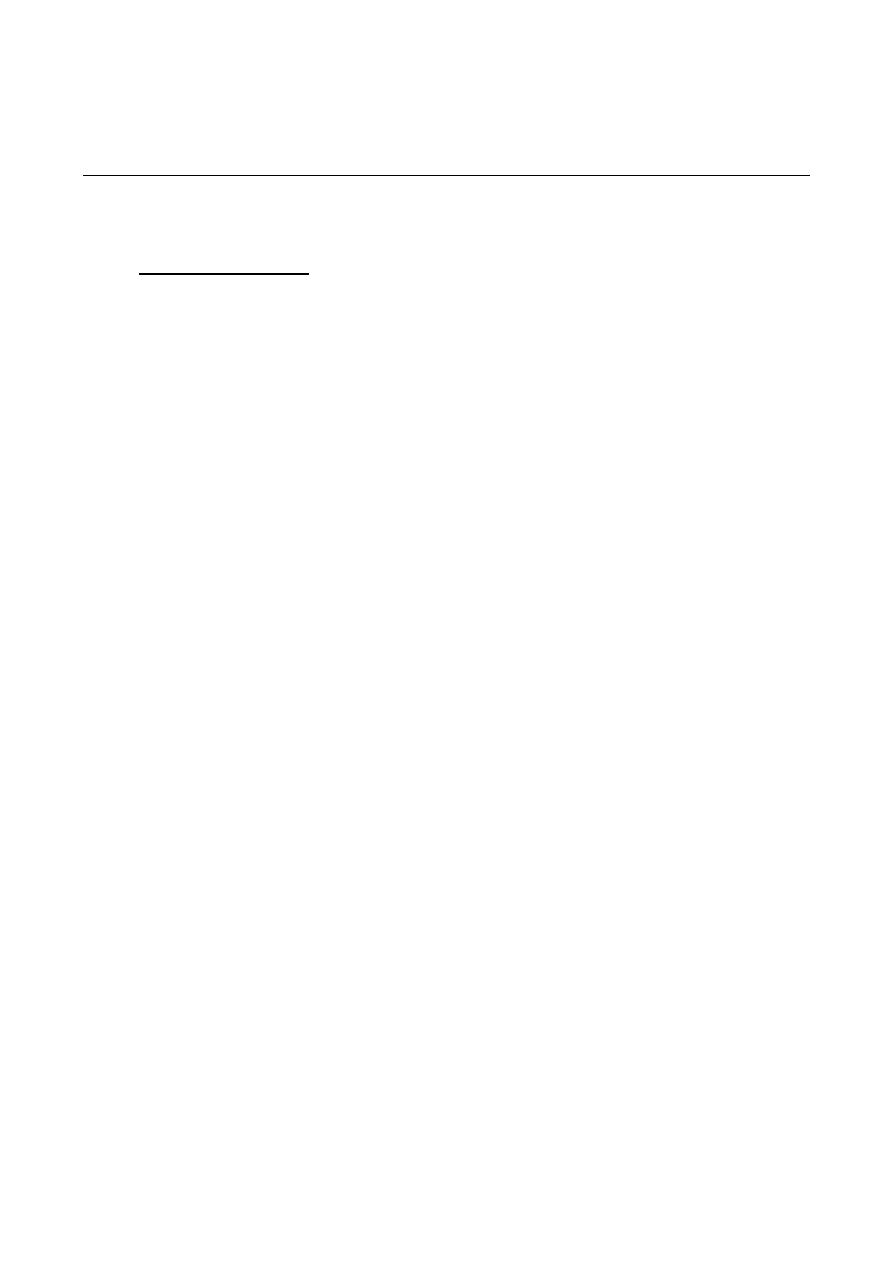
Types of casts:
1) Hyaline casts; can be seen in normal people. Can be formed due to low
flow rate, high salt concentration, and low pH.
5
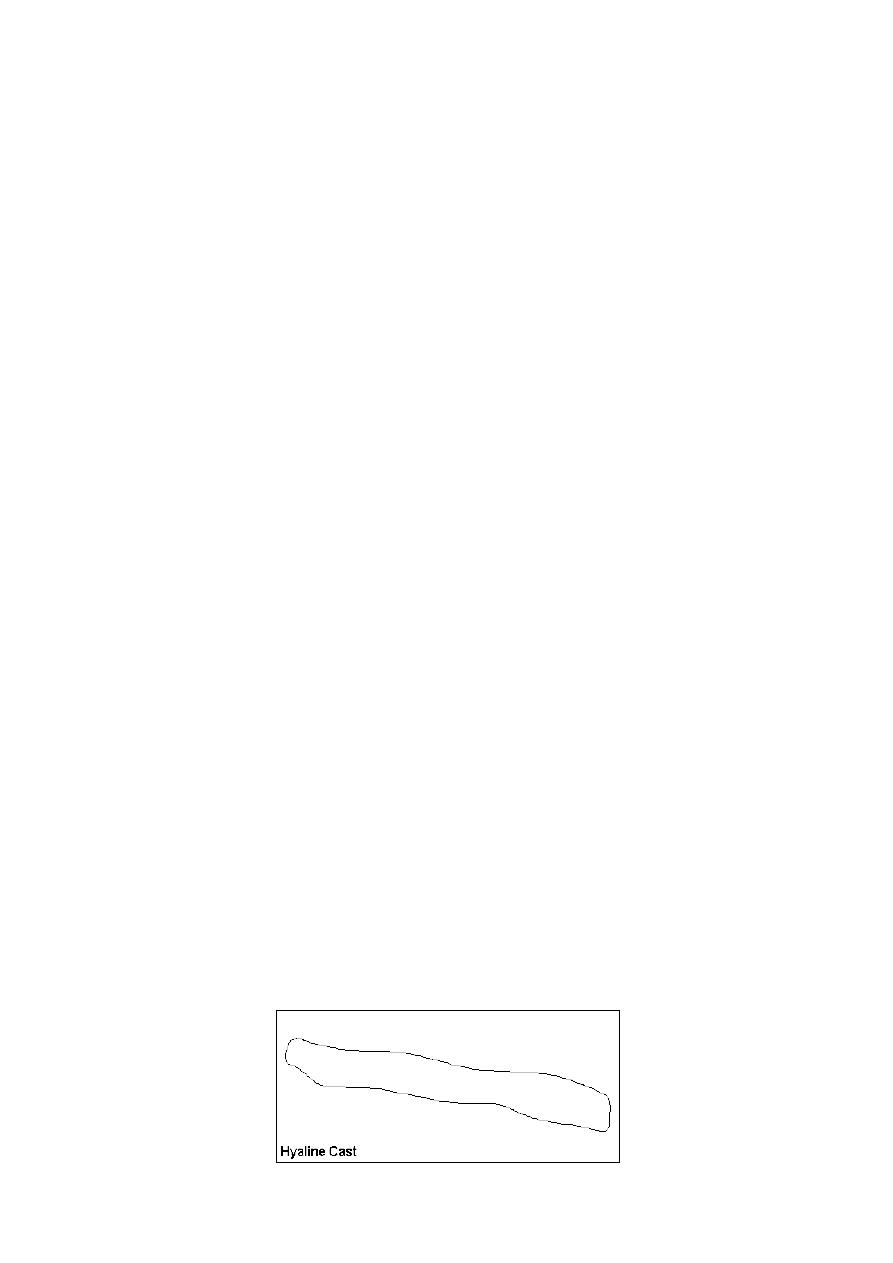
2) Red blood cells cast: RBCs may stick together and form red blood cell
casts. Such casts are indicator for glomerulonephritis, with leakage of
RBC's from glomeruli, or severe tubular damage.
3) White blood cell casts: Their presence indicates for inflammation of
the kidney, because such casts will not form except in the kidney.
4) Granular and waxy casts: they are derived from renal tubular cell casts.
Indicate for damaged tubules and usually seen in end stage of chronic
renal diseases.
6
5- Bacteria
Bacteria are common in urine specimens because of the large normal
microbial flora of the vagina or external urethra and because of their ability to
rapidly multiply in urine standing at room temperature. Therefore, microbial
organisms found in all urine samples. In suspected patients with urinary
infection, the diagnosis of bacteria needs culture. A colony count may also be
done to see if significant numbers of bacteria are present. Generally, more than
100,000 bacterium/ml is significant. Multiple organisms reflect contamination.
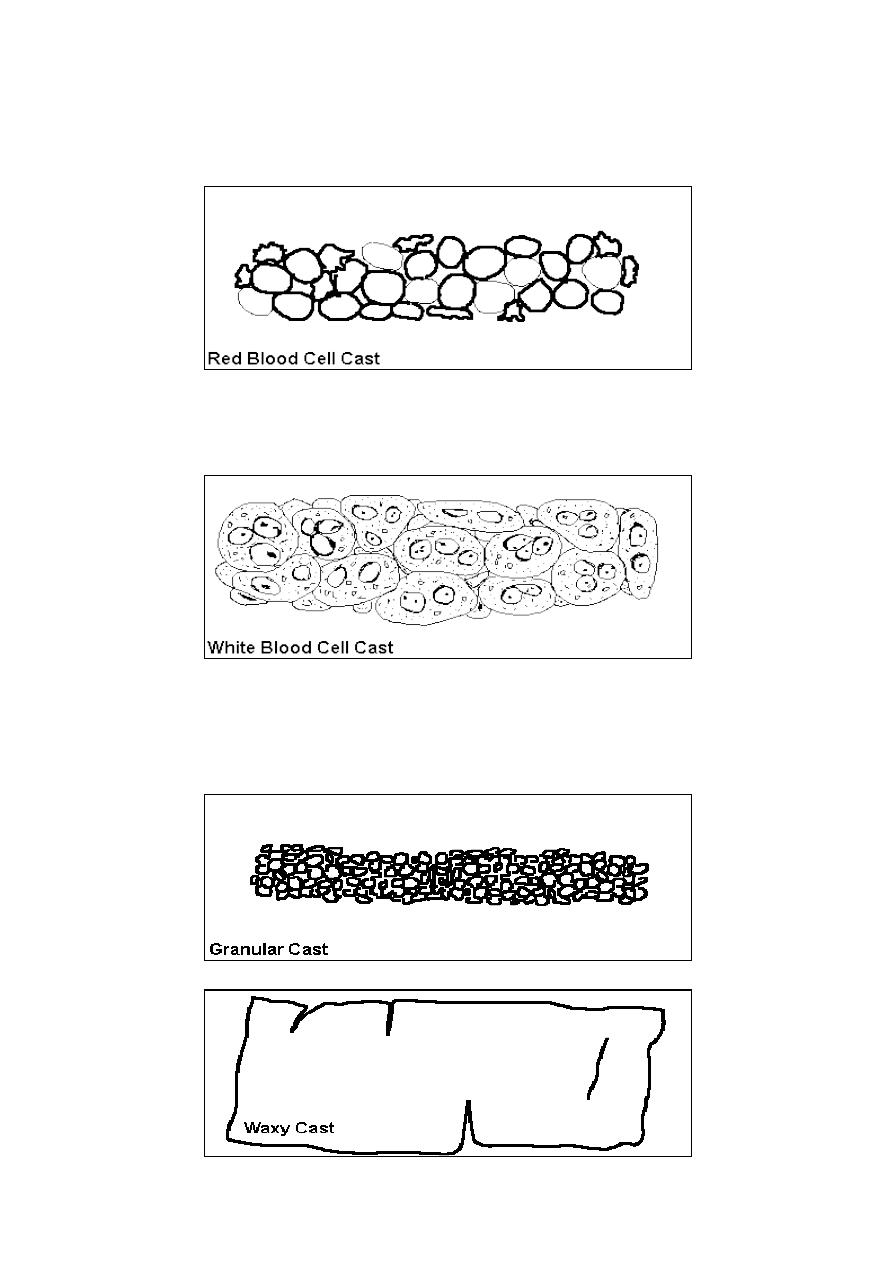
6- Yeast
Yeast cells may be contaminants or represent a yeast infection. They are
often difficult to distinguish from red cells and amorphous crystals but are
distinguished by their tendency to bud. Mostly they are Candida, which may
colonize bladder, urethra, or vagina.
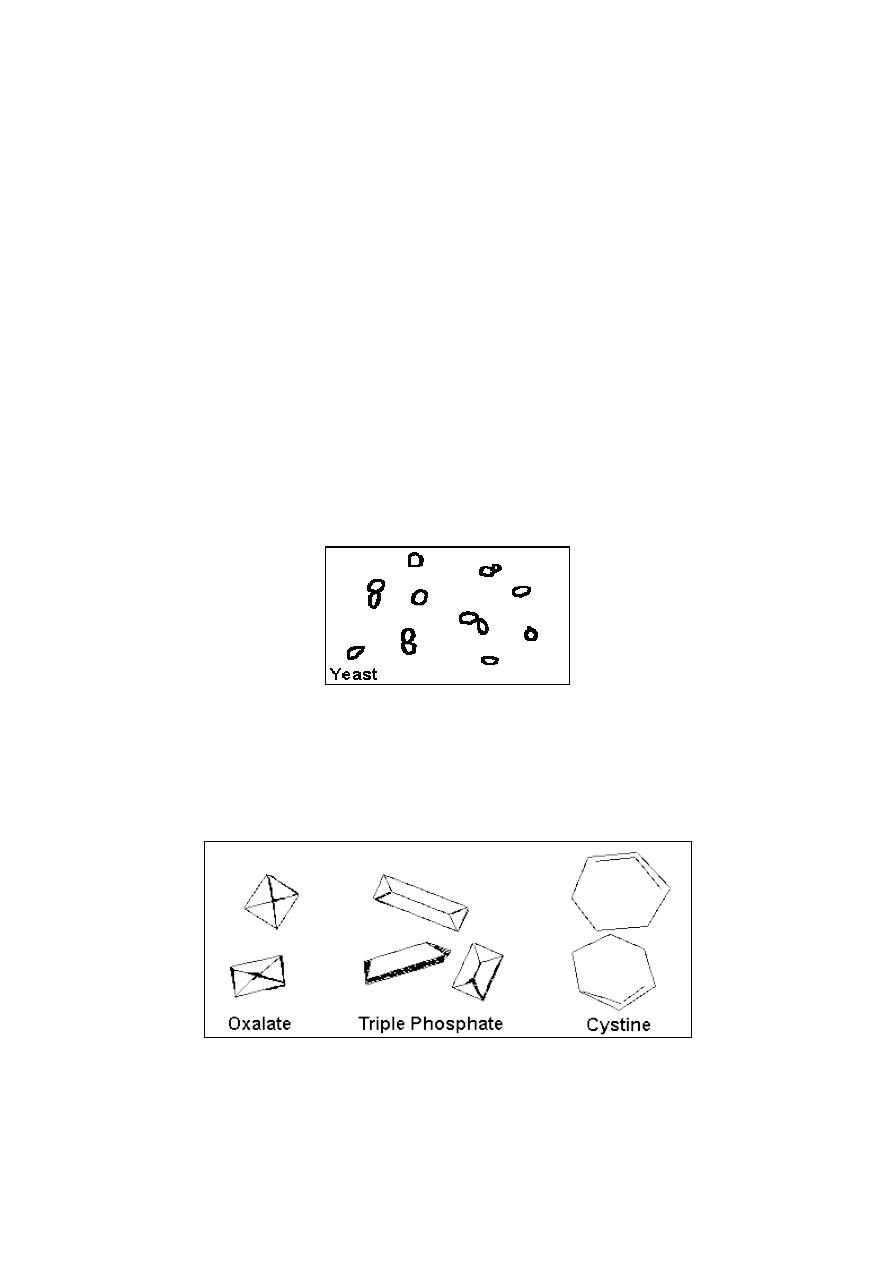
7- Crystals
Common crystals seen even in healthy people include calcium oxalate, triple
phosphate crystals and amorphous phosphates.
The uncommon crystals include: cystine crystals in urine of severe liver
disease, tyrosine crystals with congenital tyrosinosis or marked liver
impairment, or leucine crystals in patients with severe liver disease.
7
8- Others
Other objects may find their way into a specimen, particularly those that
patients bring from home. Spermatozoa can sometimes be seen. Rarely,
pinworm ova may contaminate the urine. In Egypt, ova from bladder
infestations with schistosomiasis may be seen.
2- Urine culture:
Urine sample can be used to do culture and antibiotic sensitivity test and
usually this test ordered by physician for urinary tract infection cases to
determine the most effective antibiotic to use. The special containers are
important to be used (closed and disinfected), then culturing done first on
nutrient agar for isolation then subculture for antibiotic sensitivity and other
biochemical test on the isolates sometimes. The results for each antibiotic listed
as resistance if no inhibition zone obtained and sensitive if inhibition present
(Sensitive: S+, S++, and S+++, and so on according to inhibition zone
diameter).
Urine sample should be cultured as soon as possible; some isolates need
48 hr. to show growth and inhibition zone.
3- Urine Human Chorionic Gonadotropin (HCG) Test or
pregnancy test:
Urine sample can be used for routine pregnancy testing or detection. The
human chorionic gonadotropin (HCG) is made by the placenta during
pregnancy and excreted in urine. The HCG test can be used to see if a woman is
pregnant or detection of some infertility
cases.
This test does not measure the
exact amount of HCG, but it shows if HCG is present. Home pregnancy tests
that show HCG in urine are also available. False negative result may due to
early pregnancy and need for more time to increase the amount of hormone
excreted in the pregnant woman urine. Also some abnormal cases lead to low
hormone levels in urine like ecto-pregnency.
This test is usually performed using latex agglutination Kit special for HCG.
When mixing centrifuged urine with drop of kit, then clumping (cotton like
appearance) will occurs indicating for pregnancy positive.
8
Examples for Normal Flora of urinary tract
or urogenital tract:
Candida albicans
Anterior urethra, vagina
Chlamydia trachomatis
Urethra, vagina, fallopian tubes, prostate gland
Clostridium spp
Vagina
Corynebacterium spp
Anterior urethra, external genitalia, vagina
Enterobacteriaceae
Anterior urethra, vagina
Neisseria gonorrhoeae
Urethra, vagina, prostate gland
Streptococcus viridans
Anterior urethra, vagina
Staphylococcus aureus
Perineum
Staphylococcus epidermidis Urethra, vagina
Mycoplasma hominis Cervix, vagina
Examples for pathogens of urinary tract or urogenital tract infections:
Bacteria:
Escherichia coli (cause 80- 85% of total infections)
Staphylococcus saprophyticus
Klebsiella
spp.
Proteus
spp.
Pseudomonas spp.
Enterobacter
spp.
Fungi
Mostly yeast infections with Candida albicans
Viruses
There is group of viruses infect urogenital tract but cannot be identified in ordinary
clinical laboratories.