SPINAL CORD TUMOURS
SPINAL TUMOURS
DEFINTION
A spinal tumor is an abnormal mass of tissue within or surrounding the spinal cord and/or spinal column.Spinal cord tumours
Tumours within the spine are classified accordingtheir anatomic relation to the spinal cord.
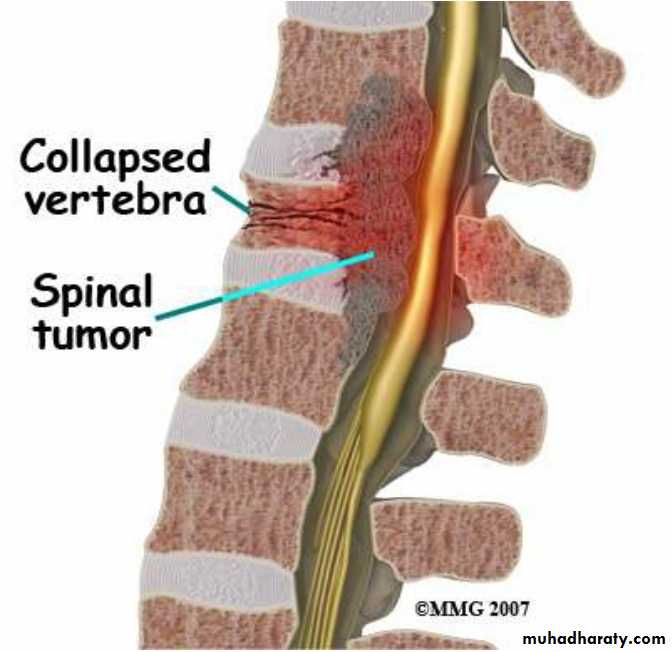
Tumours that occur within the spinal cord or exert pressure on it cause symptoms ranging from localized or shooting pains and weakness and loss of reflexes below the tumour level to progressive loss
of motor function and paralysis.
Spinal cord tumours
Classification of spinal tumorsIntra-medullary lesions (within the spinal cord)
Extramedullary- intradural lesions(within or under thespinal dura)
Extredullary-extradural lesions (outside the dural
membrane)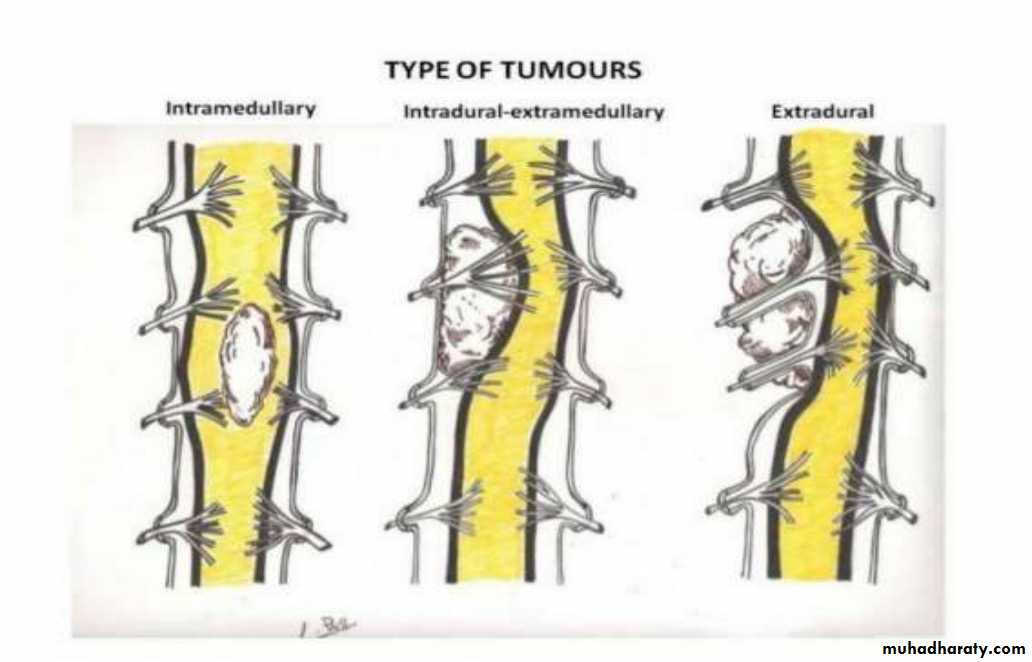
TYPES OF SPINAL CORD TUMORS
TYPES OF SPINAL CORD TUMORS
The cause of most primary spinal tumors is unknown.Degenerative process in spinal cord Metastatic tumors
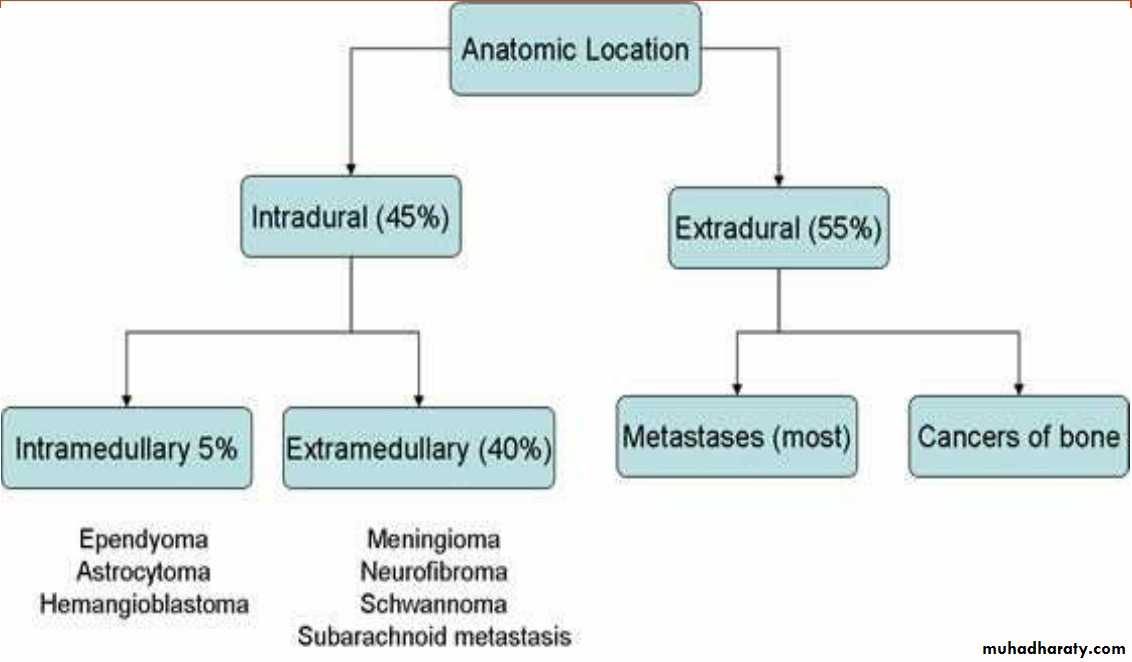
• Intradural tumors can be categorized into:
• 1-intramedullary• 2-extramedullary
• The most common intramedullary tumors are ependymoma and astrocytoma,
• whereas schwannoma and meningioma
• are the most frequent extramedullary tumors.
Clinical manifestations
Depends on location and type of tumour and extent ofspinal cord compression.
1.
Back pain that is localized or radiates, may be absent in more than 50% of clients.(is the most frequent symptom of both benign and malignant spinal tumors.)
2. Weakness of extremity with abnormal reflexes.
3. Progressive loss of motor function and paralysis
Clinical manifestations
4. Sharp pain occurs in the area innervated by the spinal
roots that arise from the cord in the region of the tumour5.
increasing sensory deficits develop below the level of the lesion.
6. Bladder, bowel, or sexual dysfunction.
Assessment and diagnostic findings
Neurologic examination.it include assessment of pain ,loss of reflexes, loss of sensation or
motor function and the pressure of weakness and paralysis.
Biopsy
X-ray and radionuclide bone scans.
CT myelography with lumber puncture is sensitive to tumour detection but may be uncomfortable &result in complications from LP.
MRI scan is the most commonly used and the most sensitive
diagnostic tool.
Medical management
Treatment of specific intraspinal tumors depends on the type and location of the tumor and the presenting symptoms and physical status of the patient.
Surgical intervention is the primary treatment for most spinal cord tumors.
Other treatment modalities include:1. Partial removal of the tumor
2. Decompression of the spinal cord
3.
Chemotherapy and Radiation therapy particularly for intramedullary tumors and metastatic lesions.
Surgical management client with spinal cord tumors.
Tumor removal is desirable but not always possible. The goal is to remove as much tumor as possible while sparing uninvolved portions of the spinal cord.Surgical management client with spinal cord tumors.
Two surgical approaches may be used to manage spinal cordtumors.
1)
Anterior decompression: is typically indicated because most spinal tumors are anterior.
2)
The posterolateral : approach may be used for excision of thoracic tumors.
Complications
A) Spinal cord infarction secondary to compression.
B) Nerve or spinal compression from tumor expansion.C) Tetraplegia or Paraplegia due to spinal cord
compression.PROVIDING PREOPERATIVE CARE:
The objectives of preoperative care include recognition of neurologic changes through ongoing assessments, pain control, and management of altered activities of daily living due to sensory and motor deficits and bowel and bladder dysfunction.The nurse assesses for weakness, muscle wasting, spasticity, sensory changes, bowel and bladder dysfunction, and potential respiratory problems, especially if a cervical tumor is present.
The patient is also evaluated for coagulation deficiencies. A history of aspirin intake is obtained and reported because the use of aspirin may impede hemostasis postoperatively.
Breathing exercises are taught and demonstrated preoperatively. Postoperative pain management strategies are discussed with the patient before surgery.
ASSESSING THE PATIENT AFTER SURGERY
The patient is monitored for deterioration in neurologic status.A sudden onset of neurologic deficit is an ominous sign and may be due to vertebral collapse associated with spinal cord infarction.
ASSESSING THE PATIENT AFTER SURGERY
Frequent neurologic checks are carried out, with emphasis on movement, strength, and sensation of the upper and lower extremities and GCS.Assessment of sensory function involves pinching the skin of the arms, legs, and trunk to determine if there is loss of feeling and, if so, determining at what level. Vital signs are monitored at regular intervals.
MANAGING PAIN
The prescribed pain medication should be administered in adequate amounts and at appropriate intervals to relieve pain and prevent its recurrence. Pain is the hallmark of spinal metastasis.Assess pain using scale of 0 to 10,as indicated.
MONITORING AND MANAGING POTENTIAL COMPLICATIONSIf the tumor was in the cervical area, the possibility of postoperative respiratory compromise arises.
The nurse monitors the patient for asymmetric chest movement, abdominal breathing, and abnormal breath sounds.
Demonstrate to patient to perform breathing exercise.
Anxiety related to diagnosis of spinal tumor, surgery and
outcome.
Pain related to nerve compression
Risk for peripheral Neuromuscular Dysfunction related tonerve compression.
Risk for injury related to surgery.
Impaired urinary elimination related to spinal cordcompression.