Done by :
Abdul Hakeem Hady.
Practical obstetric
What is showing in slide ?
Fetal head position during descent .
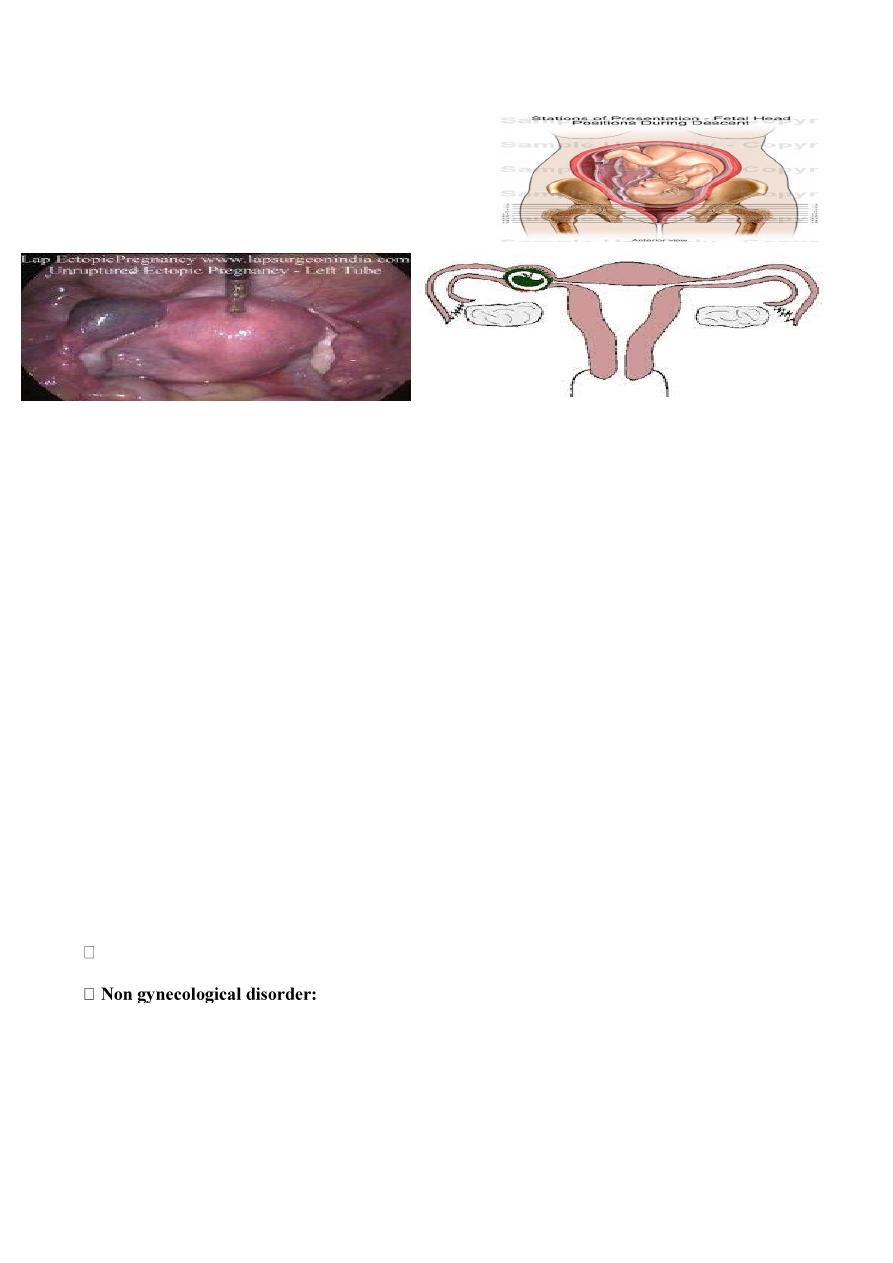
What is showing in slides ? Laparoscopy showing un ruptured ectopic pregnancy.
Sites of ectopic:
1. Fallopian tube is the most common site ( 98%), the ampulla (80%) is the most common site of implantation.
2. Also in Uterus. Ovary. Cervix.
Causes:
1. Pelvic inflammatory disease 3. Tubal surgery (tubal sterilization) 4.Congenital abnormalities of fallopian tube
5.Peritubal adhesion. 6. Endometriosis 7. Uterine fibroid 8. Intra uterine device (IUD) 9. Progesterone only pills.
Risk factors for ectopic pregnancy:
1. History of previous ectopic pregnancy 2. Early age of intercourse and multiple partners. 3. History of infertility.
4. Increased maternal age . 5. Cigarette smoking. 6 . In utero diethylstilbestrol (DES) exposure.
Course and outcome
1. Tubal abortion 2. Tubal rupture 3. Tubal mole 4. Secondary abdominal pregnancy (rare)
Clinical presentation
1. Asymptomatic
2. Symptomatic ( sharp lower abdominal pain , scanty or dark brown irregular vaginal bleeding , Amenorrhea ) .
Diagnosis :
1. HX 2. Examination .
3.Investigation : (( U\S , progesterone level , Laparoscopy , Culdocentesis ,
uterine curttage , Surgery (laprotomy)
Serum B-hCG tests are positive in 100% of ectopic pregnancy.)) and decrease in HB .
DDX :
Gynecological disorder:
1. abortion. 2. ruptured corpus luteum cyst. 3. acute (PID). 4. adnexal torsion. 5. degenerating fibroid.
Acute abdomen .
Treatment :
1. medical treatment : methotrexate , prostaglandin( PGE2 ,PGF2α), potassium chloride .
In case of :
size of ectopic pregnancy less than 4 cm.
unruptured tube.
Serum hCG level less than 1500 IU/lit.
2. Surgical approach :
immediate resuscitation and intravenous fluid with blood transfusion then under
( laparoscopy , laparotomy )
Conservative : Salpingotomy , Fimbrial evacuation. , Mid tubal resection with or with out re-anastmosis.
Radical surgery: salpingectomy
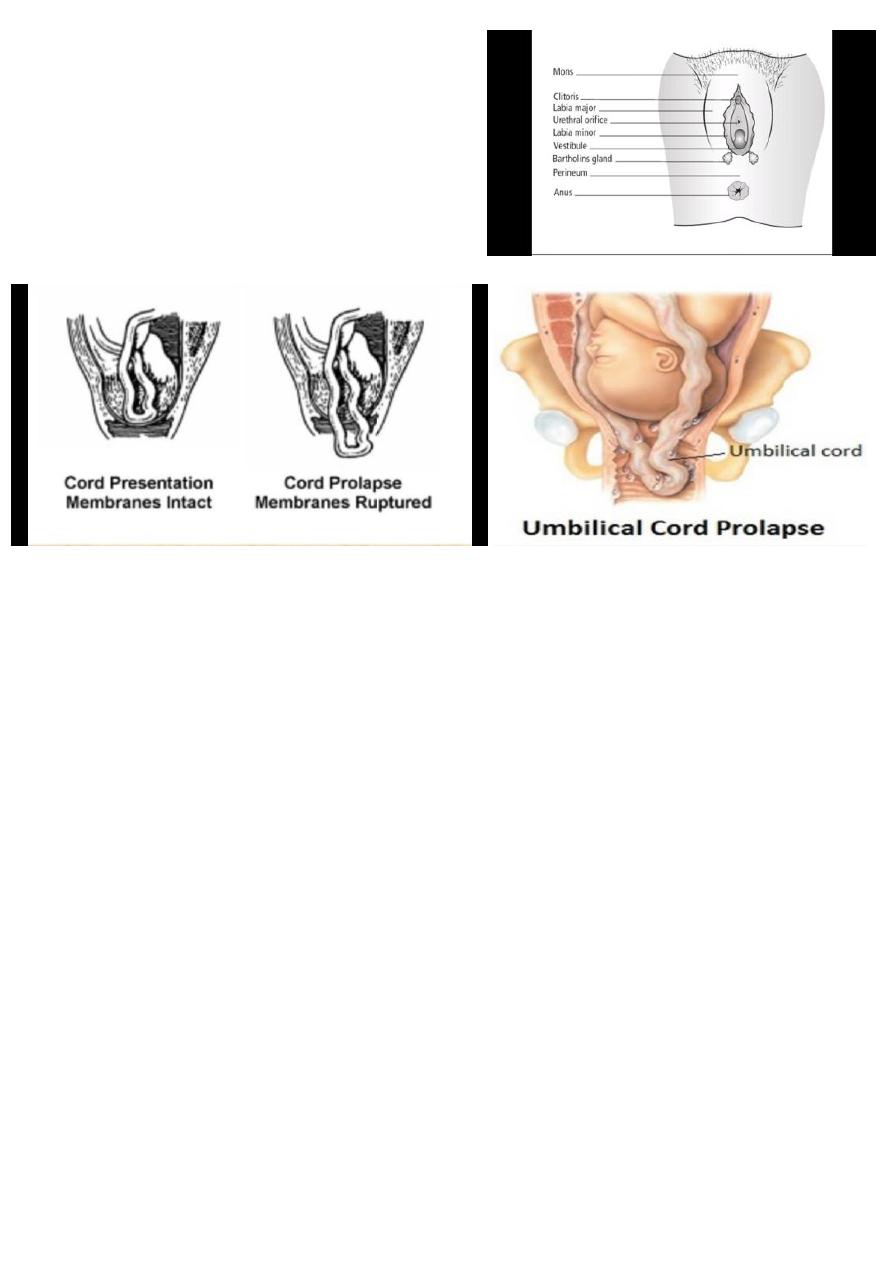
what is the image showing ?
Bartholin's duct
2 pea size gland lie at the base of each bulb and open by duct
into the vestibule
What happen if the duct obstruct ?
Bartholin's cyst ( painless swelling )
What happen if the cyst become infected ?
Bartholin's abscess ( painful swelling ).
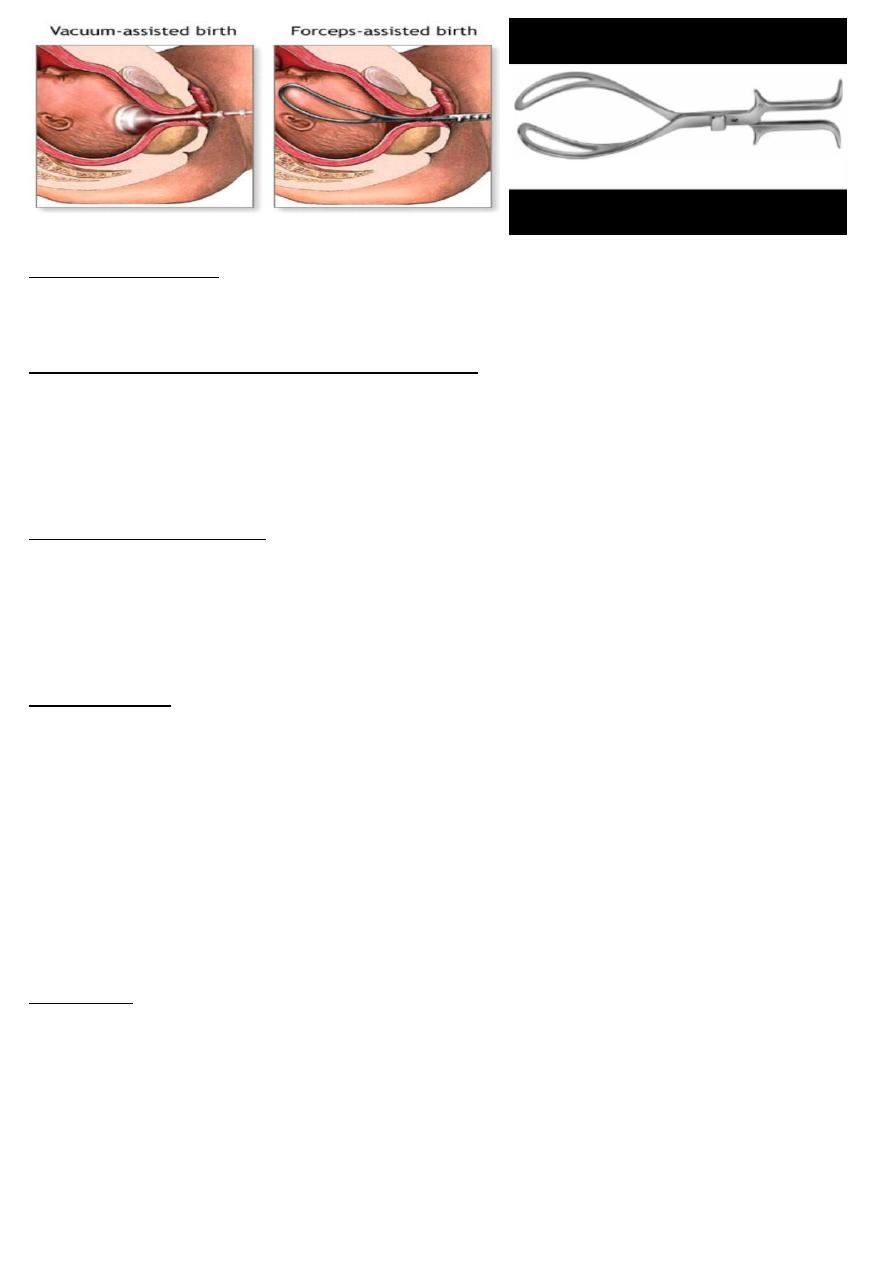
What the difference between cord presentation and cord prolapse?
Cord presentation : umbilical cord below the fetal presenting part when the membranes are intact.
Cord prolapse : umbilical cord below the fetal presenting part when the membranes are intact.
How we can diagnose it ?
Most commonly, it is diagnosed by seeing the cord at the introitus , or feeling it during a vaginal examination and
also abnormal heart rate ( deep variable deceleration and bradycardia ) may suggest it .
Risk factors( CAUSES ) for cord prolapse
1) P : Prematurity ,
Polyhydramnios , Placenta praevia , Pelvic tumors.
2) M : Multiple pregnancy , Malpresentation ( e.g breech , transverse lie ).
3) L : Large baby , long cord , low lying placenta
What the approach ?
1. Call for help
2. Check fetal heart
3. postural treatment involves
:
The cord should be replaced within the warm, moist vagina ,so preventing vasospasm.
Placing fingers in the vagina lifting the presenting part.
Placing patient in Trendelenburg's position or Knee elbow position
.
Full the bladder with 500-700 ml of saline ,used when the patient transported for some distance
4.Immediate management aims to minimize the pressure of the fetal presenting part on the cord , By
C .section is required unless the cervix is fully dilated and an assisted vaginal delivery can be safely and
easily performed .
What is Complication of cord compression ?
Total cord compression for longer than 10 minutes will cause cerebral damage and, if continued for around
20 minutes, death .
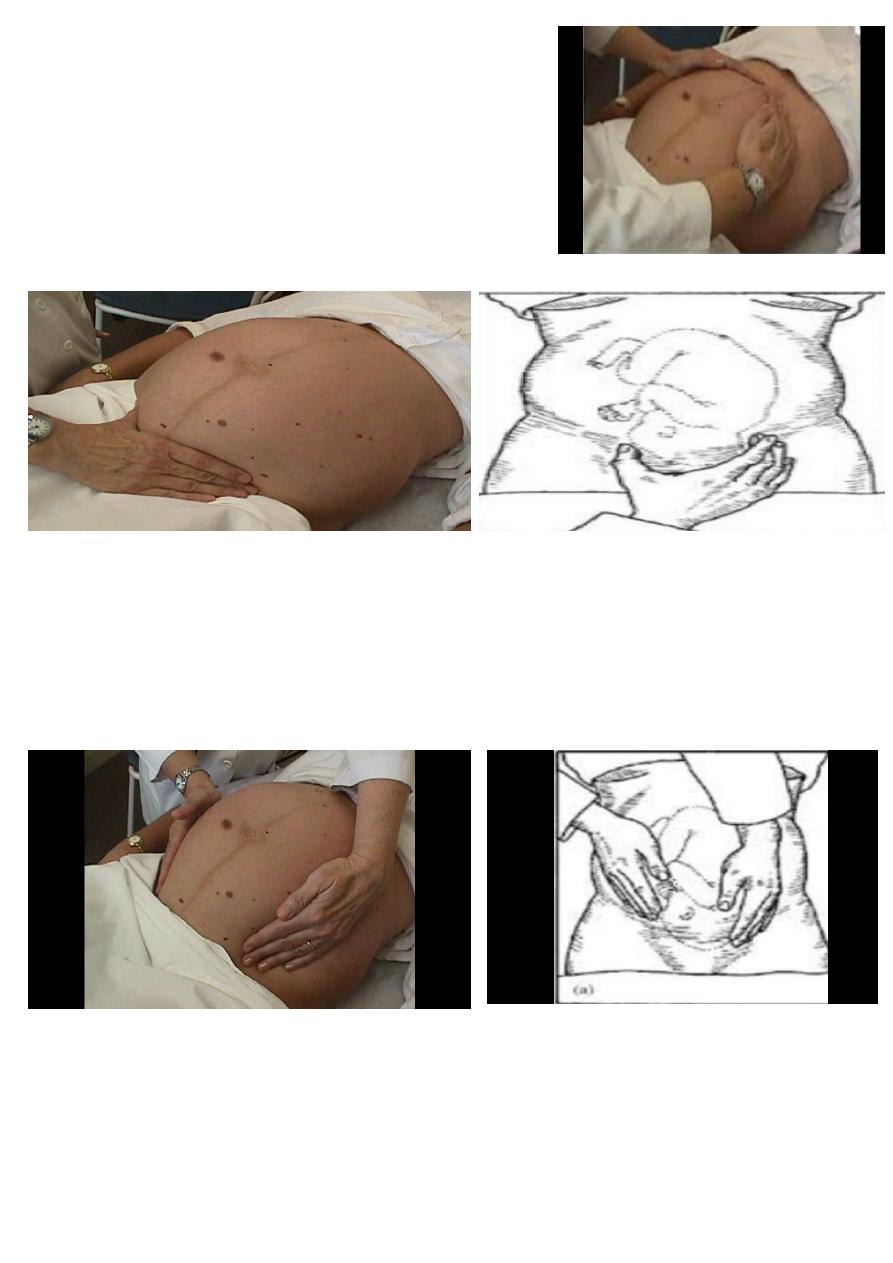
what is this instrument ?
Kielland's forceps : have minimal pelvic curve to allow rotation around a fixed axis; the sliding lock of the
Kielland forceps facilitates correction of asynclitism.
In the left : this is a vacuum
What the pre-requesting condition to use this instrument ?
1. Engaged head . 2. Position and attitude of the head .
3. Clinically adequate pelvis (mid ,outlet ) 4. Empty bladder .
5. Ruptured membrane . 6. Cervix is fully dilated .
7. Appropriate anesthesia (vacuum without ) 8. Experience of the doctor .
9. Well informed patient . 10. working equipment .
Indication for assisted delivery:
Maternal Indication :
(( Maternal distress during 2nd stage ,, Prolonged 2nd stage ,, Cardiopulmonary or vascular disease ,, Vaginal
birth after previous lower segment C.S. to reduce the stress on the scar ,, vaginal bleeding . ))
Fetal Indications :
(( Malposition of the fetal head (OP, OT) , Fetal distress and cord prolapse , Preterm baby )).
Contraindication :
Absolute :
lack of engagement .
Condition that contraindicate vaginal delivery (pelvic abnormality , fetopelvic disproportion)
Fetal malposition (face ,brow).
Dead fetus with postmortem changes .
Inability to diagnose the position of the fetal head .
Relative :
Fetal macrosomia .
Lack of experience .
Fetal bleeding or suspected coagulation defect .
Premature < 34 weeks or less than 1500 gm .
Complication
Maternal complication.
Soft tissue injuries Genital : uterine ,cervical ,vaginal ,perineal lacerations .
Bladder and urethral injury : retention ,fistula .
Rectal injuries : laceration ,fistula ,defecation problems .
Fetal complication :
with forceps (( Transient facial marks , Facial palsy and intracranial hemorrhage , Fracture of skull or facial
bones , Sever cervical cord damage )).
With vacuum ((Scalp injury , Fracture of skull , Cephalhaematoma , Subgleal hematoma , Intracranial
haemorrhage , Tentorial tears , cerebral palsy )).
what you see ? name the maneuver ?
Abdominal examination, ( fundal grip )
Use both hand to feel which part of fetus lying the fundus .
What is your finding ?
Cephalic: is more firm, hard, round that moves independently of the
body
Breech: is less well defined, moves only in conjunction with the body
Name this maneuver ?
Pelvic grip ( Pawlik’s grip):
Spread apart the thumb and fingers of the hand. Place them just above the patient’s symphysis pubis
What is the finding ?
a.)If descended (engaged): you’ll feel the head fixed
b.)If undescended (not engaged ): you’ll feel less distinct mass mobile.
Name this maneuver ? pelvic grip
Facing foot part of the woman, palpate fetal head pressing downward about 2 inches above the inguinal ligament.
Use both hands.
What is the finding ?
Good attitude: if brow correspond to the side that contained the elbows & knees.
Poor attitude: if examining fingers will meet an obstruction on the same side as fetal back. If brow is very
easily palpated, fetus is at posterior position.
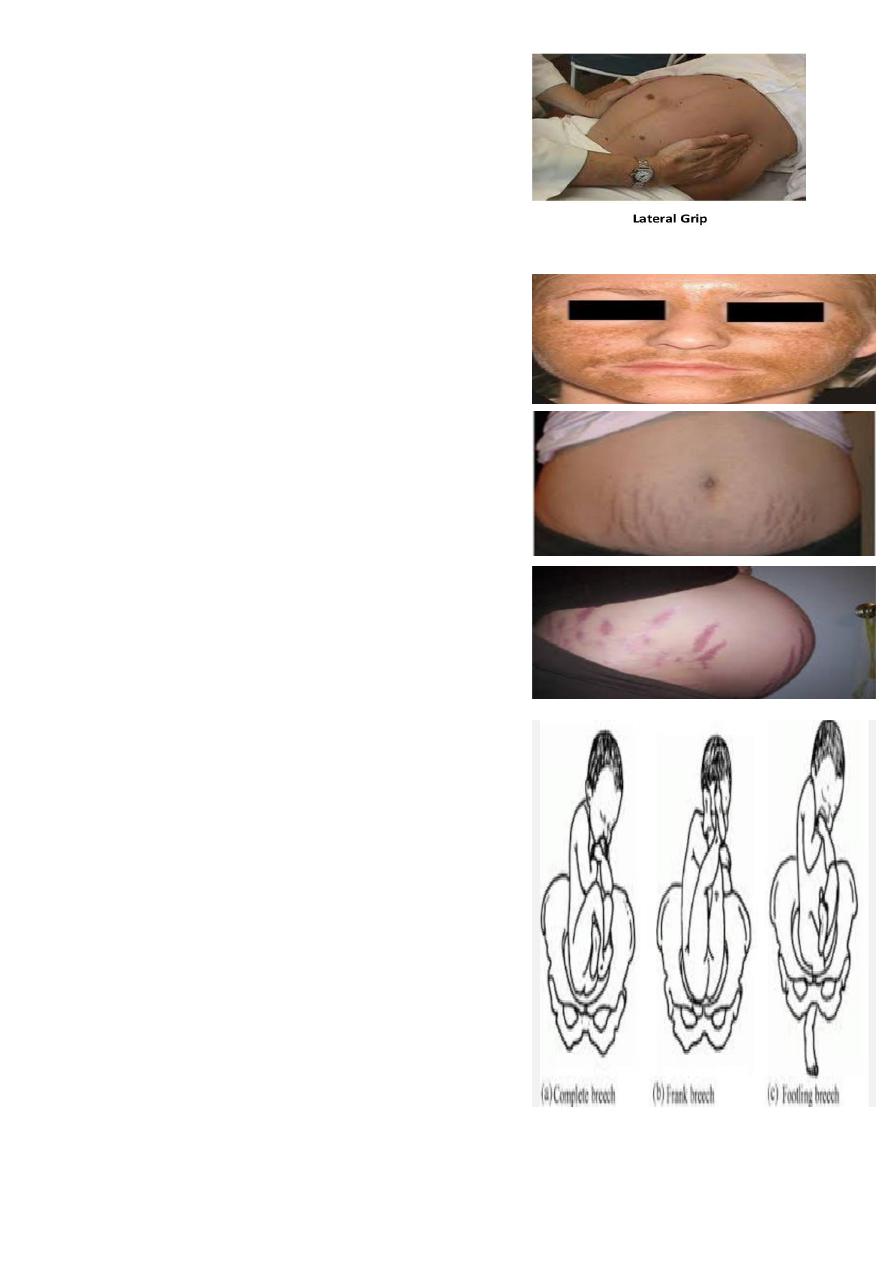
Name this maneuver ? Lateral grip
Move your hands down the sides of the abdomen and apply
gentle pressure.
What is the finding ?
Fetal back: is smooth, hard, and resistant surface
Knees and elbows of fetus: feel with a number of angular
nodulation .
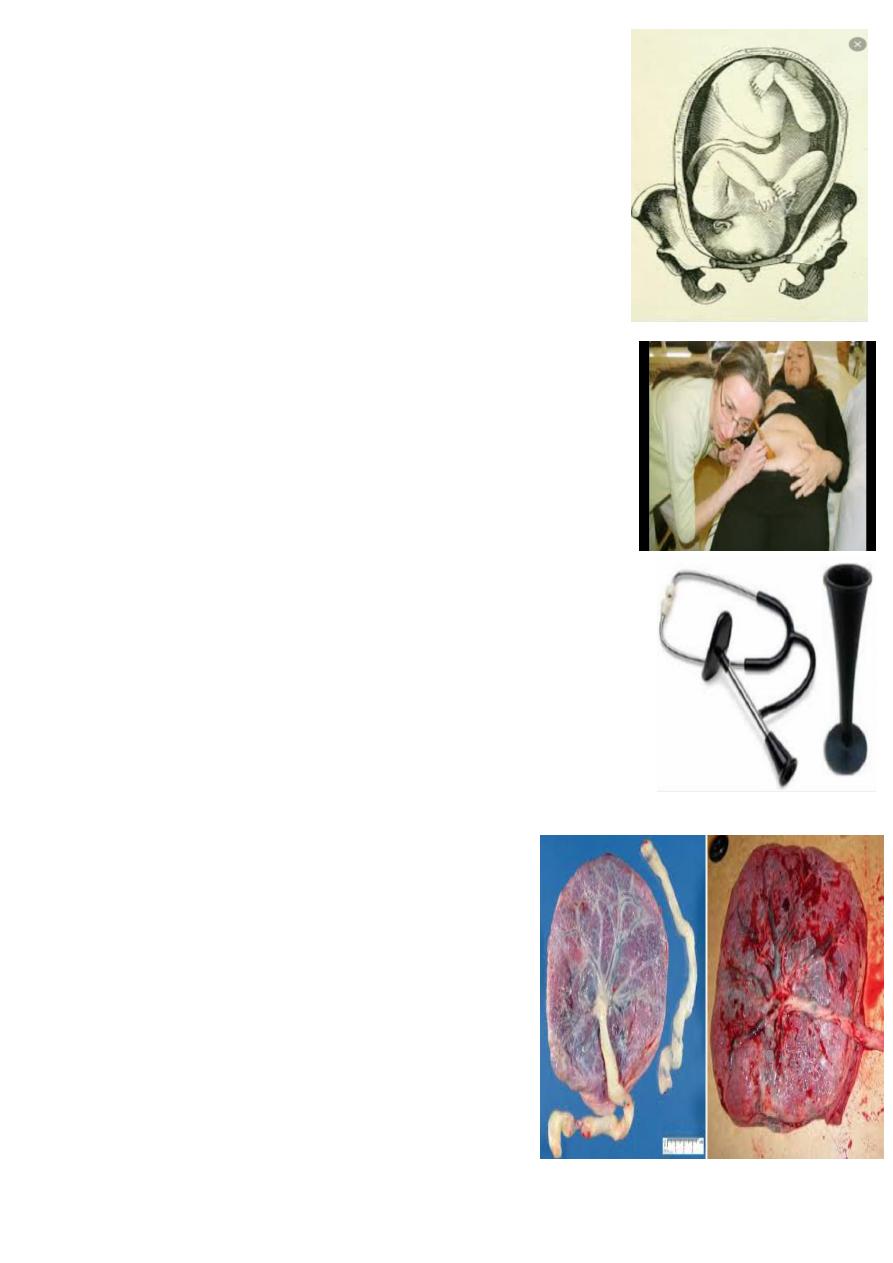
What is your diagnosis ?
Chloasma ( mask of pregnancy )
What is your diagnosis ?
Stria albicans : of previous pregnancy .
Slivery white in color ( due to fibrosis )
What is your diagnosis ?
Stria gravidarum: of current pregnancy
Pinkish in color
What is your diagnosis ?
Breech presentation
What is the type of breech ?
Frank (65%) - Hips flexed, knees extended
Complete breech (25%) - Hips flexed, knees flexed
Footling or incomplete (10%) - One or both hips extended,
foot presenting
What is the predisposing factor ?
1. prematurity , is major cause .
2. uterine abnormalities (malformations, fibroids).
3. fetal abnormalities (CNS malformations, neck masses )
4. multiple gestations. 5. AF abnormality. 6. Contracted pelvis.
On examination :
My finding is :- Longitudinal lie , breech presentation
Head is not engaged (not reach ischial spine) , Fetal heart is +ve
How to diagnosis of breech ?
Palpations and ballottement( leopold man.)
Pelvic exam , Ultrasound , X-ray studies.
What is the management ?
1. ECV : at 38 wks of gestation ( in the absence of risk ) .
2. Assisted vaginal breech delivery . 3. C.S ( elective , emergency ) .
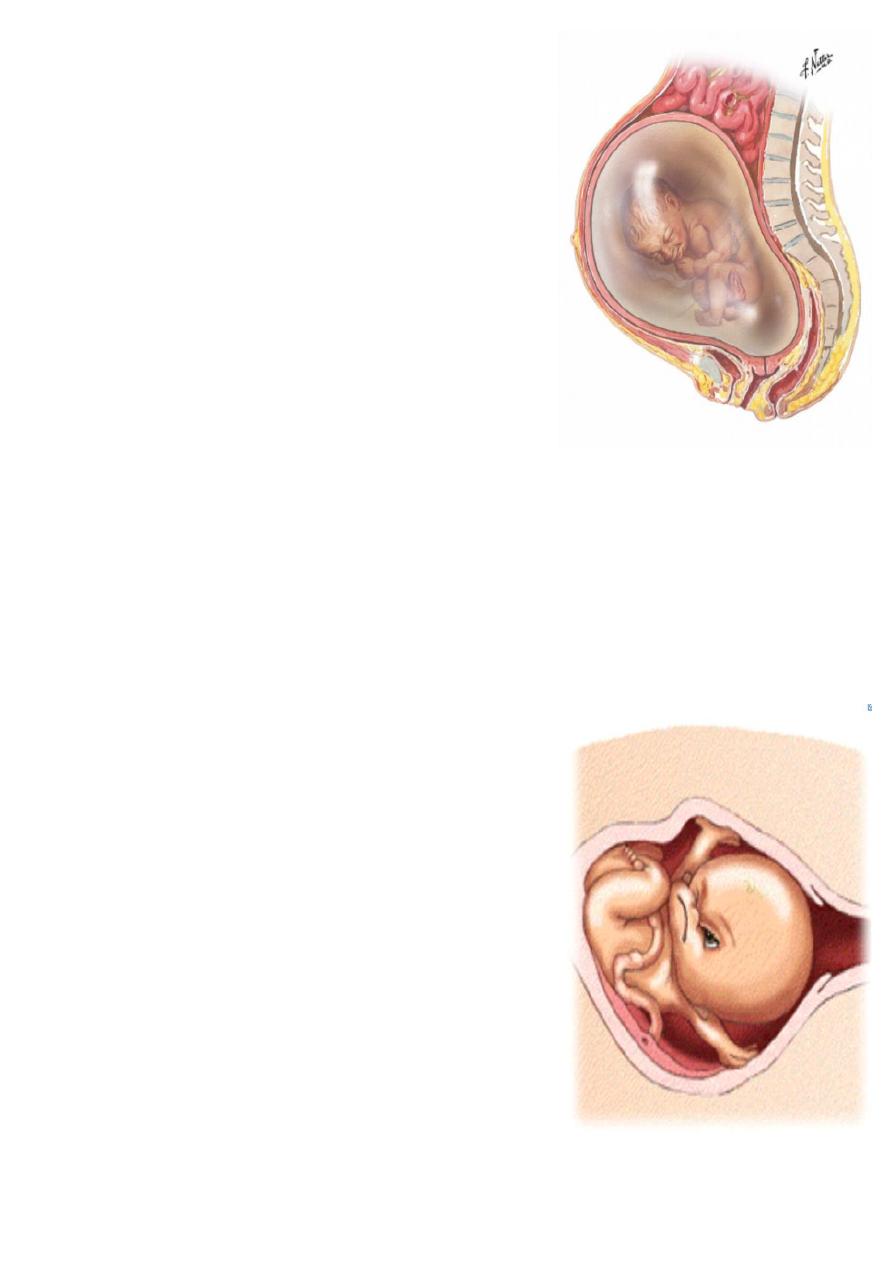
What is the diagnosis ?
face presentation .
Causes:
1. Anenecephaly
2. Prematurity
3. Multifetal pregnancy
4. sterno mastoid spasm
5. neck tumour
what is the mode of delivery ?
Mento anterior– Vaginal delivery
Mento posterior- Ceasaeran
what you seen in the image ?
fetoscope used for auscultation of fetal heart .
what is the name of this stethoscope ?
pinnerd stethoscope .
mention other type of stethoscope ?
sonic aid
At which point the fetal heart can be heard ?
If the presentation is cephalic : at a point midway between the anterior superior
iliac spine & the umbilicus on the back of the baby (usually in the right).
In breech presentations: the heart sounds will often be heard above the umbilicus
In Head (vertex) presentations: the heart sounds will often be heard below
umbilicus
What is the feature of normal fetal heart ?
RATE ( 115_ 150 bpm ) ,, Variability ( 5-15 ) ,, acceleration ( 15bpm for 15 second)
What the causes of diminished or absence heart rate ?
( Sleeping , fetal distress , fetal death , cord prolapse , IUGR , Position of fetus ).
What is the character of normal placenta ?
Shape: discoid
Site :fundal .ant or post.
Surface:
Fetal surface : smooth with central insertion of umbilical cord
(2 artery 1 vein).
Maternal surface : divide into surface called cotyledons ( 15 -
20), rough surface .
Weight : 1/6 of the fetus wt. (average 500 gm ).
What is the abnormality of placenta ?
Anomalies in weight
Bilobate & trilobate placenta
Placenta succenturiata
Placenta circumvallata
Morbid adherence of the placenta
Site of implantation of the placenta
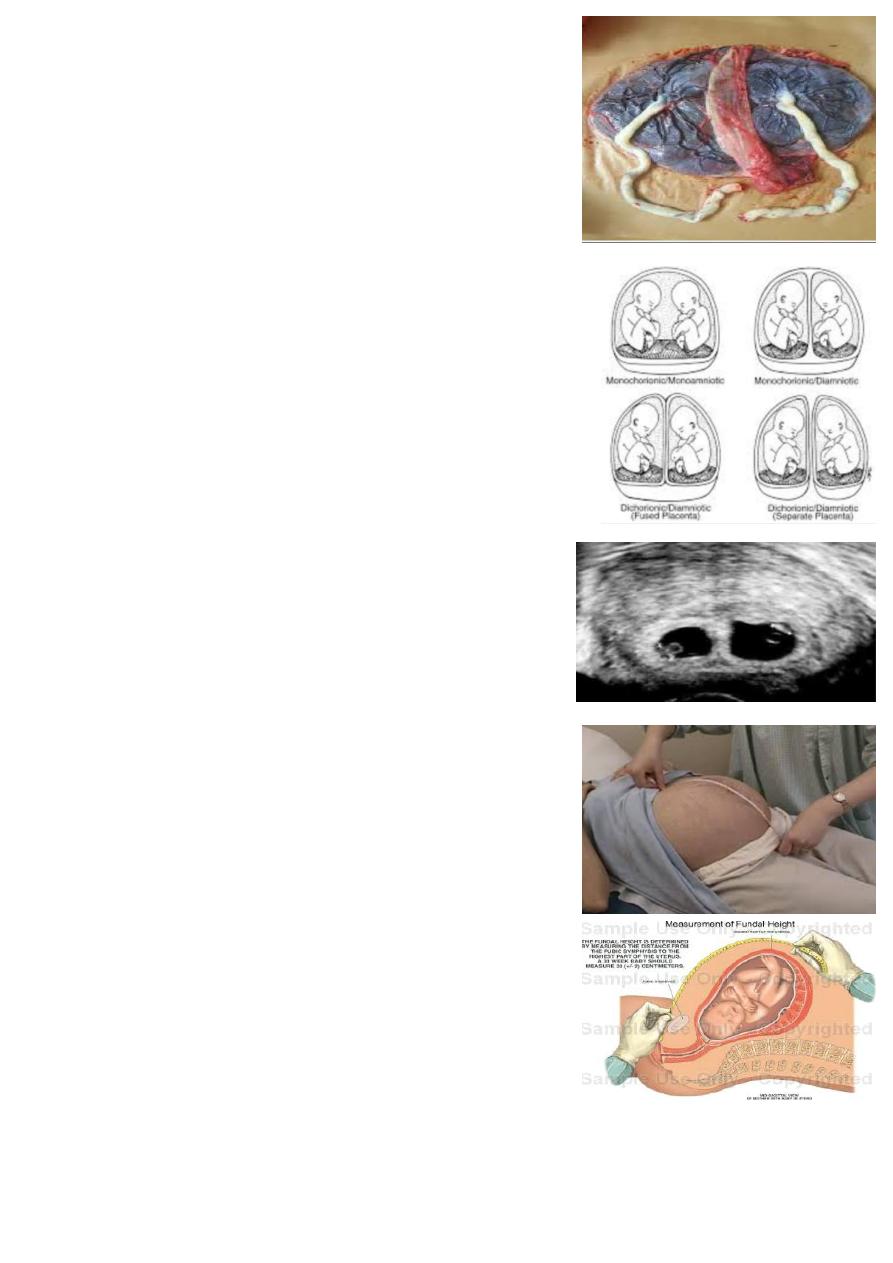
What is this ?
Placenta of twin pregnancy
What if the function of placenta ?
1. Enables the fetus to take oxygen & nutrients from the maternal blood.
2. Excretory function when CO2 & other waste products pass from the
fetus to the maternal circulation.
3. Barrier against the transfer of infection to the fetus.
4. Secrete hormones like hCG, oestrogen and progesterone.
What is this ?
Type of twin pregnancy .
embryo splits at 3 days ---» two chorions, two amnions (DCDA(
embryo splits at 4-7 days ---» single placenta, one chorion, two
amnions (MCDA(
embryo splits at 8-12 days ---» single placenta, one chorion and one
amnion (MCMA) (rare).
embryo splits at 13 days ---» conjoined or Siamese twins (very rare)
What is this ? Ultrasound
showing intrauterine pregnancy with two gestational sac.
( gestational sac can be seen in 5-6 weeks and fetal heart can be heard in
7 weeks ).
What is name of this maneuver ?
Fundal height :
the distance from the pubic bone to the top of the uterus
measured in centimeters.
Fundal height at level of symphysis pubis >> 12 weeks
Fundal height at level of umbilicus >>> 22 weeks
Fundal height at level of xiphosternum >>> 36 weeks
What is the causes of small and large for date uterus ?
Small for date
Large for date
Intra-uterine growth
retardation (IUGR)
Miscalculation (Wrong
LMP)
Oligohydramnios
Genetics
Transverse lie
A baby prematurely
descending into the pelvis
or settling into a breech
death
Rapid fetal growth
Miscalculation (Wrong
LMP)
Polyhydramnios
Multiple pregnancies
Macrosomia (diabetic
mother)
Abruption placenta
Multiple uterine fibroids
Edema and Full bladder
molar pregnancy
1. what is the diagnosis ?
Macrocosmic baby ( more than 4 kg )
DUE TO diabetic mother .
2. what is the intrapartum complication of macrosomia ?
Diagnosis an RX : يقرا من المحاضرة
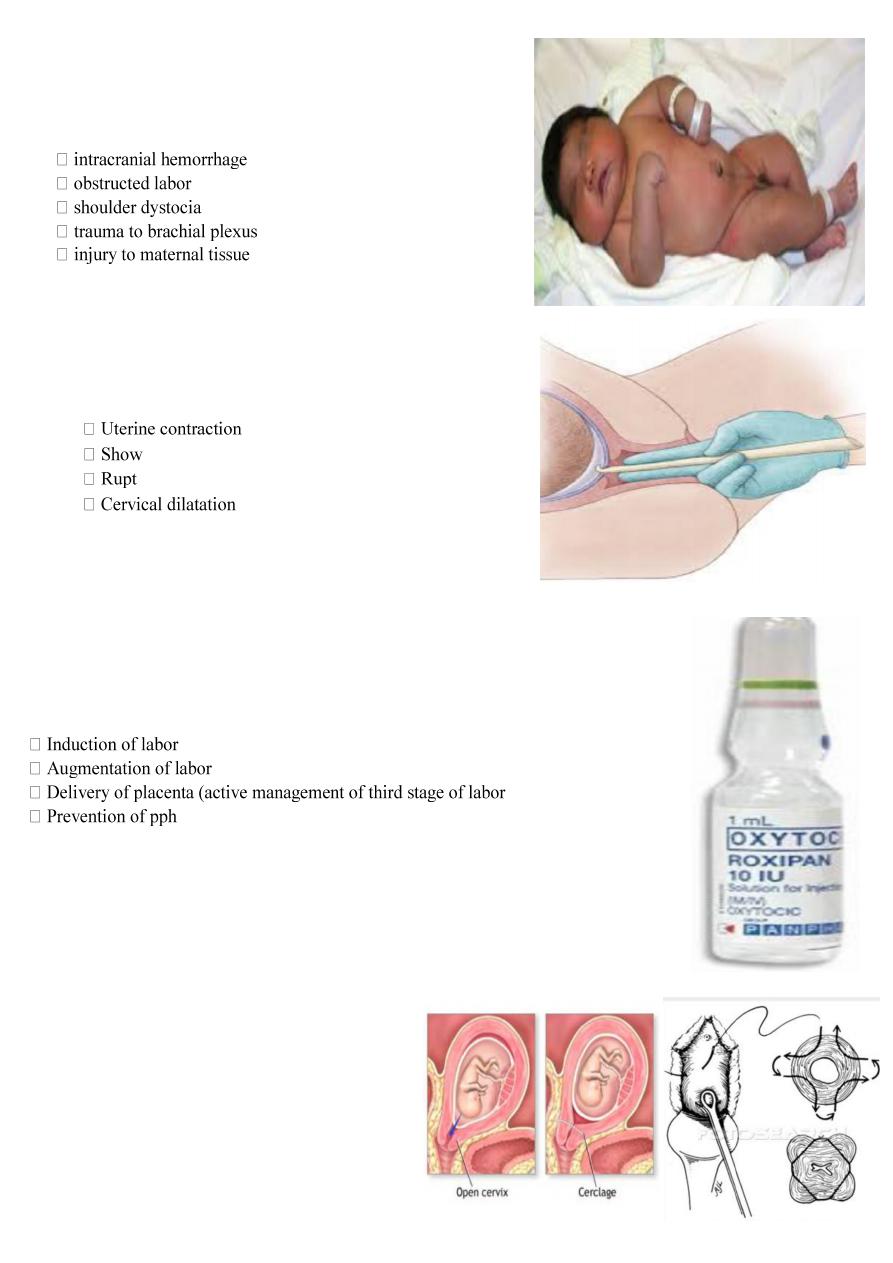
What is your diagnosis ?
artificial rupture of the membrane (aminiotomy ).
What is signs of labor ?
ure of membrane
Complications of AROM ?
( Infection , Injury to fetal head or maternal tissue , Cord prolapse ,
Bleeding )
What is this drug ? what is the doses of it ?
Oxytocin injection
Dose : ( 10 IU or 5 IU )
What is the uses of oxytocin ?
)
Complication of oxytocin :
1.Hyperstimulation.
2.water intoxication with convulsion and coma.
3.post partum hemorrhage : mainly due to uterine atony.
4. poor uterine action.
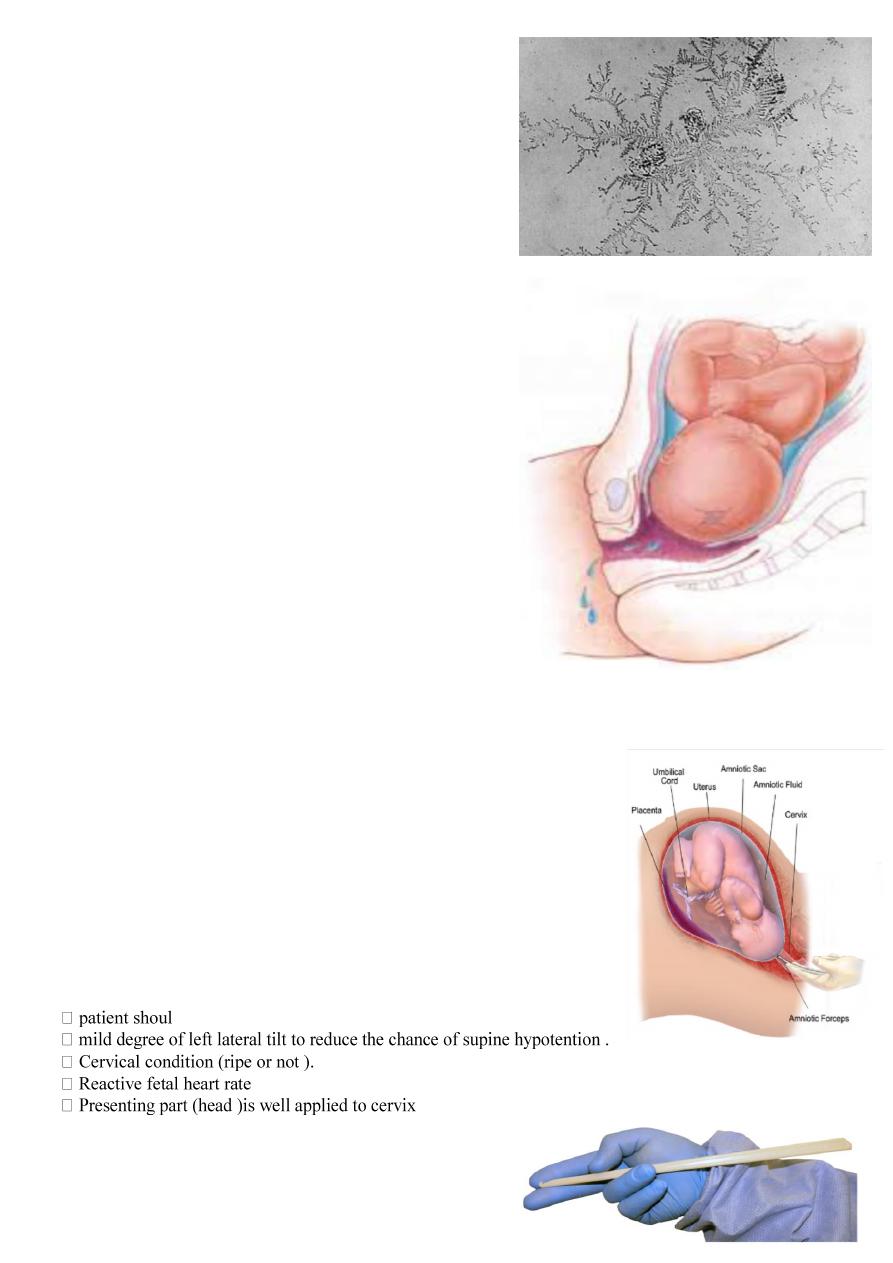
5.Neonatal hyperbilirubinemia.
What is this procedure ?
Cervical cerclage .
Used in : recurrent abortion .
By insertion of purest ring suture of non-absorbable
material before 14wks and remove it at 37wks .
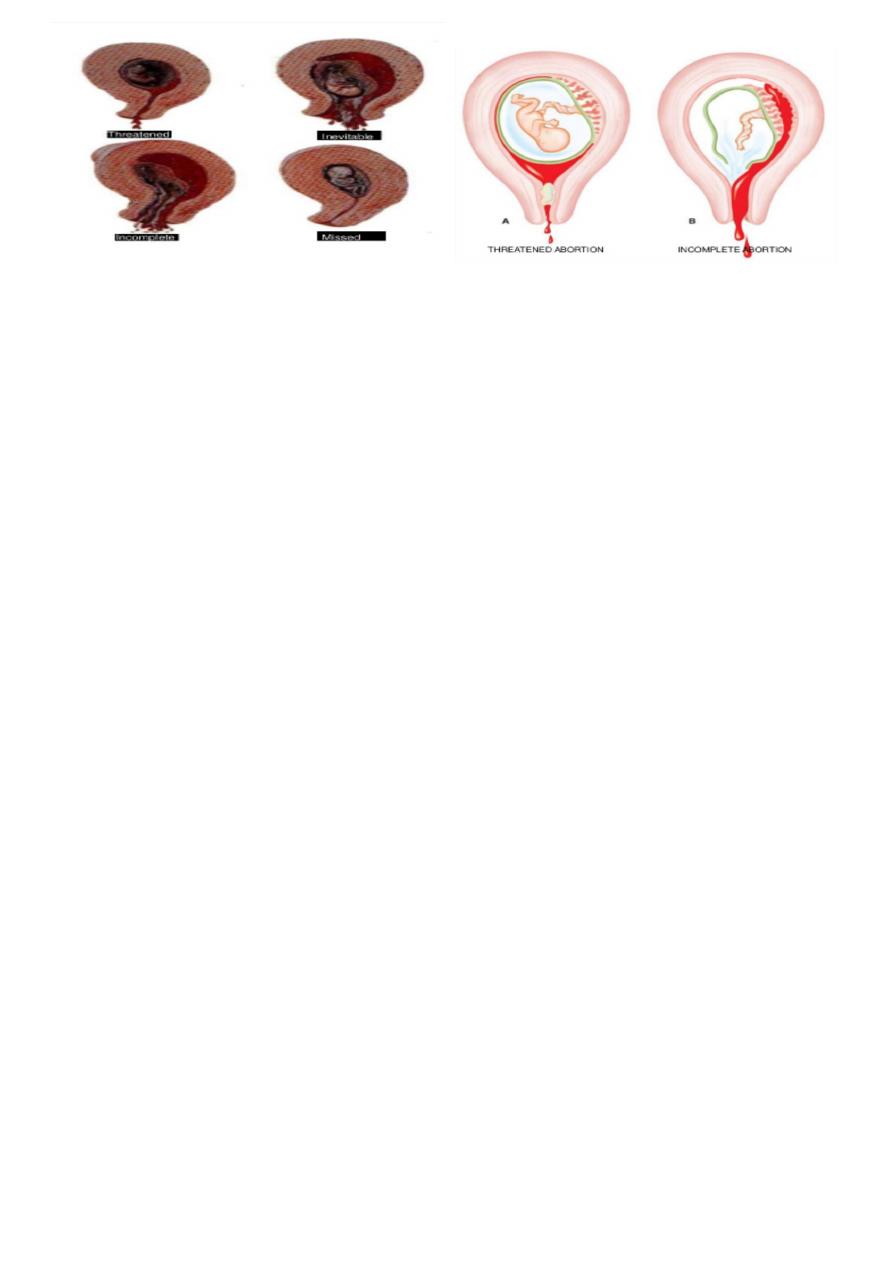
What is this ?
Types of abortion .
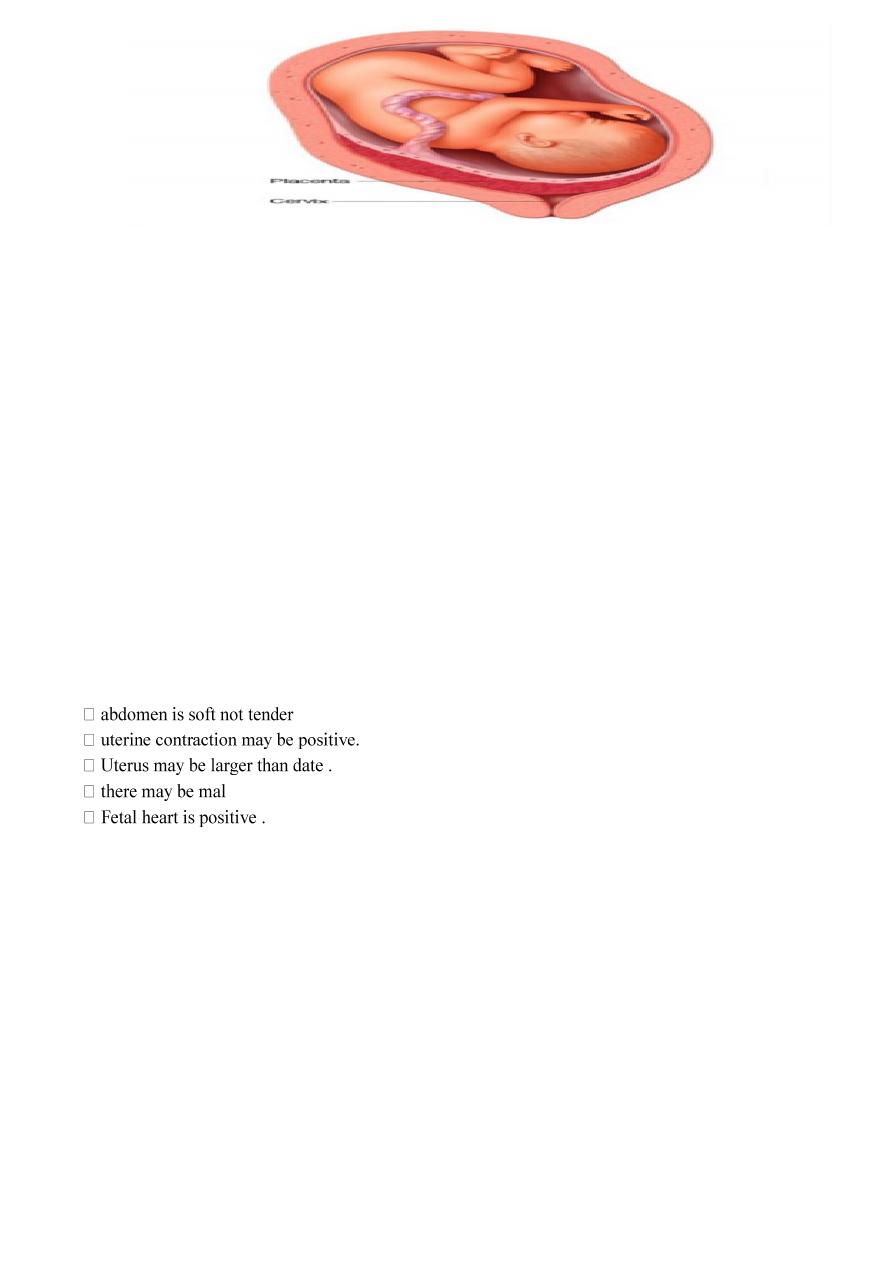
1.Threatened abortion :
symptoms:
1.scanty uterine bleeding(fresh blood) preceded by symptoms of pregnancy(frequency urination ,
backache , morning sickness , amenorrhea).
2.pain is usually absent but may be backache or mild lower abdominal pain.
Signs (Examination):
1.uterus is enlarged corresponding with date of amenorrhoea. 2.cervix is closed. 3.no pelvic tenderness
Investigations:
1-Ultrasound :confirm intrauterine gestation (IUG) and fetal heart (FH).
2-Human Chorionic Gonadotrophin (hCG) increase in serial measurement.
Treatment :
1-No specific treatment needed. only need reassurance and rest until bleeding stopped.
2-Progesterone, hCG it's benefit is not confirmed yet???
3-Anti D (250unite) should be given to non sensitized Rh negative women.
2-Inevetible pregnancy :
Means that it is impossible for the pregnancy to continue and the process is now irreversible
Symptoms:
1.severe vaginal bleeding because a large area of the placenta has detached from the uterine wall.
2. It is accompanied by acute abdominal pain which is similar to the pattern of uterine contractions in labour (intermittent).
3. No products of conception expelled yet.
Signs: (( Uterus is enlarged ,, Internal os is dilated (open)…..))
Treatment:
a-in first trimester :
Evacuate uterus under general anesthesia by curettage or suction curettage (without cervical dilatation because
cervix is already dilated).
b-in second trimester :
Allow miscarriage to take place spontaneously and the process can be expedited and bleeding controlled with
ergometrine 0.5mg and oxytocin 5unit(increase contraction of uterus) or prostaglandin in addition to supportive
therapy (correction of blood loss, analgesia, antibiotic is given as necessary).
Uterus need evacuation if patient not abort all the product of conception and severe bleeding was associated.
Anti D (250unite) should be given to non -sensitized Rh negative women .

3-Incomplete abortion :
Symptoms:
1. uterine bleeding which is varies may be severe to cause hypovolemia or mild
2.history of passing part of conception (Women describe the product of conception as looking like pieces of skin )
Sign:
1.Uterus may be smaller than expected for period of amenorrhea.
2.Cervix is open.
3.Speculum examination reveals dilated internal os and tissue within the endocervical canal or vagina.
4.Bleeding may be heavy.
Treatment:
A-Severe vaginal bleeding
1- Need admission to hospital and resuscitation with intravenous fluid (IV) fluid and blood transfusion(if needed)
and give analgesia and evacuation of uterus by curettage without need of dilatation under oxytocic drugs.
2-Anti D (250unite) should be given to non -sensitized Rh negative women.
3-Digital removing of product of conception which are in cervical canal is advised as this help to relieve the
discomfort.
B. Mild vaginal bleeding:
1-Ultrasound examination done to confirm presence of retained product of conception which need surgical
evacuation by curettage.
2-Anti D (250unite) should be given to non-sensitized Rh negative women.
4- complete abortion :
Symptoms:
Scanty blood loss and cessation of abdominal pain after history of severe abdominal pain
and severe vaginal bleeding with passing product of conception.
Signs
1.uterus is smaller than period of amenorrhea and firmly contracted.
2. cervix is closed or patulous in multiparous women.
Investigations:
Ultrasound to confirm empty cavity.
Treatment
-No further treatment is needed but patient warned to report at once if bleeding recur or develop fever.
Anti D (250unite) should be given to non sensitized Rh negative women.
5-Missed abortion
:
Symptoms:
1.May be preceded by sign and symptom of threatened abortion.
2.Disappearance of symptoms of pregnancy.
3.Dark brown vaginal discharge.
4.Diagnosed incidentally by ultrasound(sometimes).
Signs:
1.Uterus is smaller than period of amenorrhea (small for date uterus).
2.Cervix is closed.
Investigations:
1-hCG drops in 7-10 days. Positive test dose not exclude missed although negative test support diagnosis of dead fetus
2-Ultrasound showed: no fetal heart and gestational sac may collapse.
-If ultrasound is not available, abdominal x-ray after 16 weeks show collapse of fetal skeleton
Complication:
1.infection. 2.coagulation disorder DIC 3. psychological distress to mother.
Treatment:
First trimester:
Suction curettage is preferred.
Second trimester:
Induction of abortion and uterine activity is stimulated by oxytocin infusion after pre treatment with mifepristone or
vaginal prostaglandin E2 or prostaglandin extra-amniotically by folly catheter introduced through cervix.
Anti D (250unite) should be given to non sensitized Rh negative women.
........................ اقرأ االنواع االخرى من المحاضرة
.......
What is your diagnosis ?
Placenta previa
Aetiology : Not well known but may be due to
1-Low implantation of the blastocyst.
2-Development of the chorionic villi in the decidua capsularis leading to attachment to the lower uterine segment.
3-Large placenta as in twin pregnancy.
4-Older multipara.
5-Previous uterine damage and caesarean section.
6-Uterine abnormality.
Degrees ( types ) :
-First degree (Type I = P.P. lateralis = low-lying placenta):-
The lower edge of the placenta reaches the lower uterine segment but not the internal os.
-Second degree (Type II= P.P. marginalis):
The lower edge of the placenta reaches the margin of the internal os but does not cover it.
-Third - degree (Type III= P.P. incomplete centralis):
The placenta covers the internal os when it is closed or partially dilated but not when it is fully dilated.
-Fourth - degree (Type IV = P.P. complete centralis):
The placenta covers the internal os completely whether the cervix is partially or fully dilated.
Symptoms (( Painless vaginal bleeding ,, Uterine contraction ))
Signs
-presentation as breech or transverse lie or non-engaged cephalic presentation .
Vaginal examination :
P/V is indicated only if active treatment is initiated. This may provoke a severe attack of bleeding so it should be
done with the following precautions:
1-In the operating room, 2-under general anesthesia, 3-operating theatre is ready for immediate caesarean section.
If the index finger is introduced gently through the dilated cervix, the placenta can be felt as a tough fibrous mass
.
Investigation : ( ultrasound ,, Soft tissue placentography, isotopes and thermography ,, MRI ).
Treatment
If mild to moderate vaginal bleeding conservative management inform of correction of anemia ,
corticosteroid therapy
If sever and persistent vaginal bleeding and any bleeding after 36 week emergency delivery is indicated .
Patient with no vaginal bleeding should be delivered at term (38 week).
Mode of delivery: CS.
Complication :
1-Maternal:
(
Abortion , Preterm labour , Antepartum haemorrhage, PROM , Cord prolapse , PPH
)
2-Foetal: ( Prematurity , Asphyxia , Malformations (2%).
)
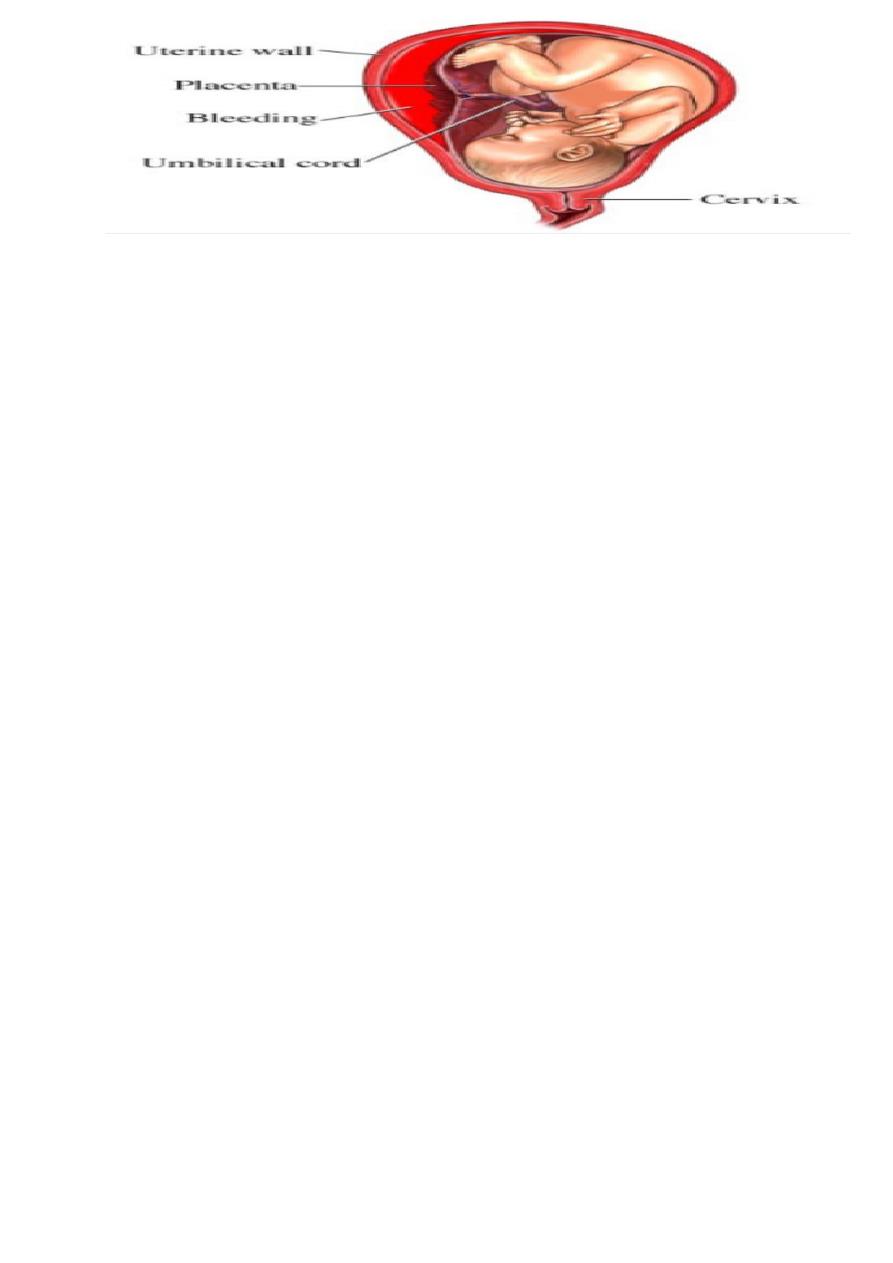
What is the diagnosis ?
Abruptio placenta .
Aetiology :
-Unknown, but the following factors may be associated with:
1-Hypertensive disorders of pregnancy (30%) due to spasm and degenerative changes in the decidual arterioles.
2-Trauma as during external version.
3-Sudden drop of intrauterine pressure as rupture of membranes in polyhydramnios.
4-Folate deficiency and may be vitamin C,K, or E deficiency.
5-Passive congestion of the uterus due to pressure of the gravid uterus on the inferior vena cava.
6-Torsion of the uterus.
7. Smoking .
Types
revealed hemorrhage (external )
concealed hemorrhage (internal )
Symptoms :
1-Acute constant severe abdominal pain which may be localised or diffuse.
2-Dark vaginal bleeding results from escape of blood from the retroplacental haematoma.
3-Cessation of foetal movement is common.
Abdominal examination:
-Uterus is large for date and increasing gradually in size due to retained blood.
-Uterus is very tender and hard (board-like).
-Fetal parts are difficult to be felt.
-FHS may be absent due to fetal death in severe cases or distressed in mild cases.
Vaginal examination:
Done under the same precautions in placenta praevia may reveal:
-Vaginal bleeding which is dark as it is retained for some time before escape.
-If the cervix is dilated the placenta is not felt.
Treatment :
General and abdominal examination and resuscitation ( give blood , normal saline ,HB , prepare blood )
Ultrasonography.
Delivery :
Patient with abruptio placenta has to be delivered and usually there is no place for conservative treatment.
-Amniotomy + oxytocin if:
1-bleeding is not severe, 2-vertex presentation, 3-the cervix is partially dilated.
4-adequate pelvis with no soft tissue obstruction .
CS indicated in :
1-Severe haemorrhage whether the foetus is dead or alive.
2-Living foetus and labour is expected to be longer than 6 hours e.g. closed cervix.
3-Foetal distress.
4-Failure of progress after amniotomy + oxytocin.
Complication of A.P : (( hypovolemic shock , fetal distress , DIC , Renal failure , Couvelaire uterus ))
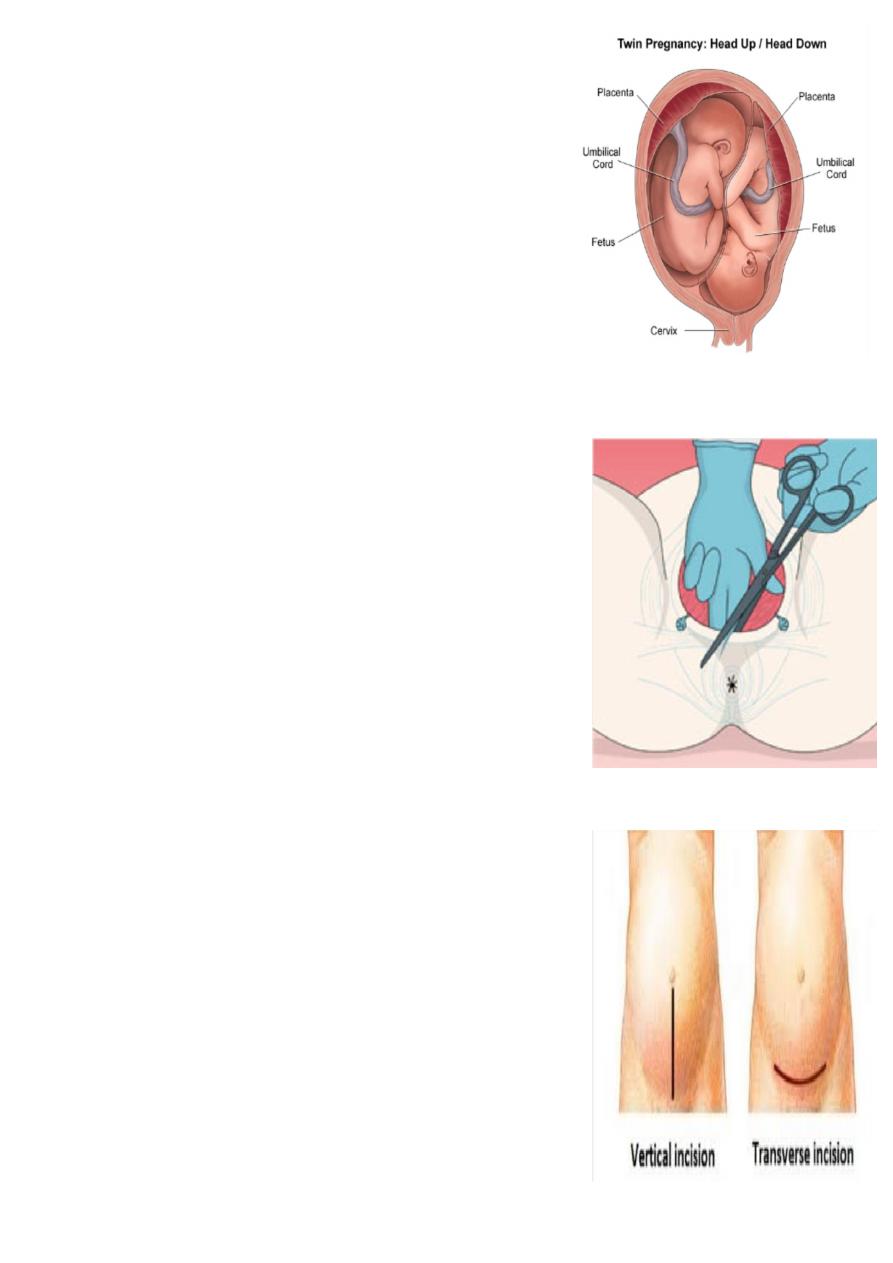
what is the diagnosis ?
Twin pregnancy.
Aetiology:
Dizygotic twins arise from the release of two eggs at ovulation.
Monozygotic twins arise from a single fertilized ovum that split into
two identical structures
How to delivery twin ?
Vaginally : The ideal criteria for a twin labour are:
Spontaneous onset,
Cephalic presentation of twin 1,
Twin 1 larger than twin 2,
Dichorionic pregnancy.
CS incase of ( 1
st
baby in transverse lie and in locked twin )
Complication : (( small babies , prematurity , congenital anomalies , cord prolapse , TTTS ….etc ))
What is this procedure ? Episiotomy
Indication :
Absolute :
previous pelvic reconstruction.
pelvic floor surgery.
Relative :
short rigid perinium.
shoulder dystocia.
fetal distress.
instrumental or breech delivery.
What is the type of it ?
(( Midline episiotomy, Medio-lateral episiotomy , Lateral episiotomy ))
Complication:
1.Difficult repair. 2.heavy bleeding. 3.extention to the anus. 4.infection.
5.pain and dyspareunia. 6.weak point in the perineum-tear.
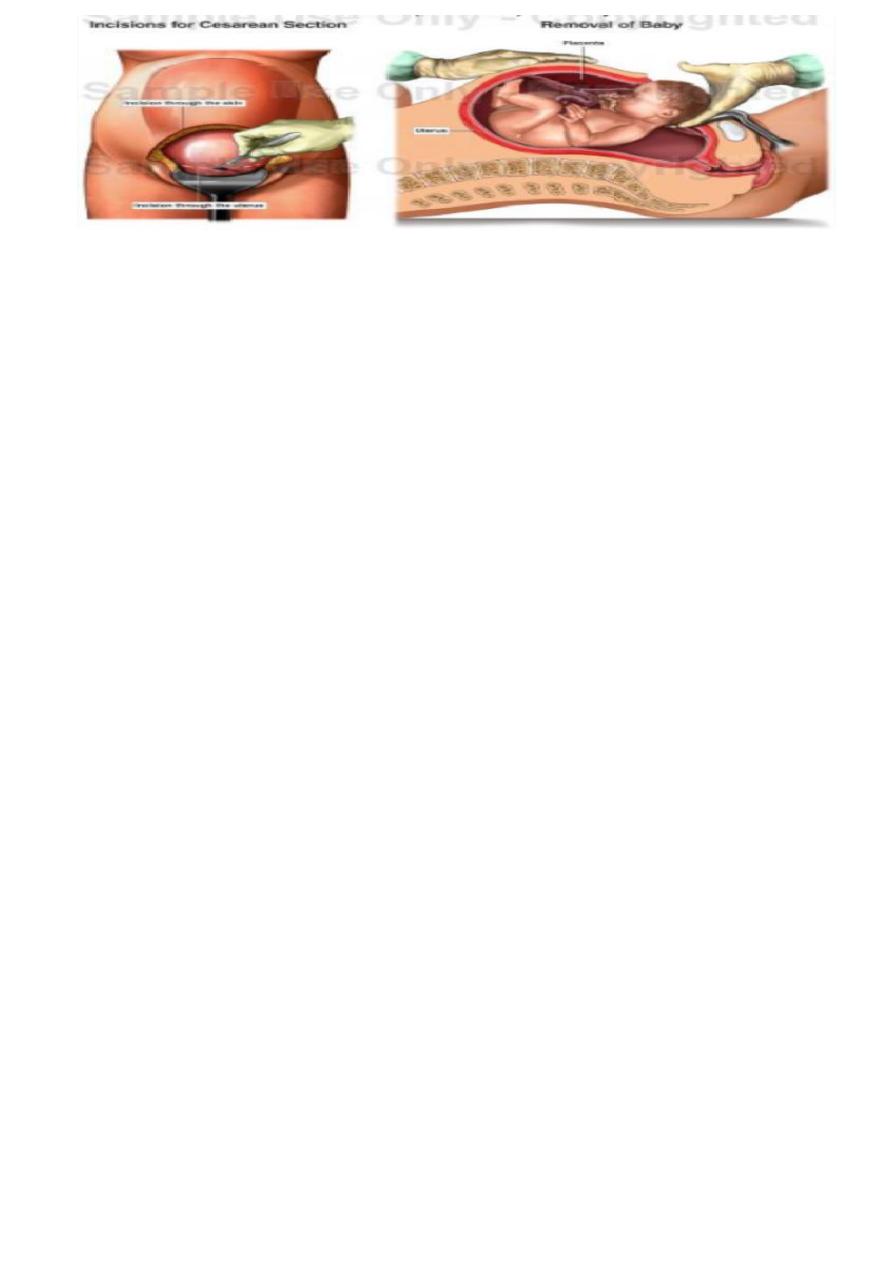
What you see in the picture ?
Incisions for CS .
Types of incisions :
Skin incision :
Low transverse suprapubic incision .(more cosmotic , less
dehiscence and hernia ).
Cohen’s incision : less post operative febrile morbidity , shorter
operative time .
Midline or paramedian incision better exposure .
Uterine incision :
Low transverse LSCS :
less dissection of the bladder , blood loss is less , lower incidence of
uterine rupture .
Low vertical incision .
Classical or upper segment incision .
What is this ?
caesarian section .
Preparation for C.S :-
Left lat. Position .
Empty the stomach and antacid , Thrombo prophylaxis .
Prophylactic antibiotics and Catheterization .
Skin preparation : shaving . iodine , chrorhexidine .
Investigation ( HB , cross match , prepare blood , serology , GUE , Fasting blood sugar , U\S , ECG ).
Indication of C.S.
1. Dystocia (maternal/fetal )
CPD.
Failed induction of labour.
2. Maternal
Disease : PE , Eclampsia/DM/cardiac dis./ cervical CA .
Previous uterine surgery : Classical C.S. / Previous 2 C.S. / Previous myomectomy (Full thickness ) .
Obstruction to birth canal : fibroid / ovarian tumor.
3. Fetal :
Fetal distress .
Cord prolapse.
Fetal malpresentation.
4. Placental : (( placenta previa , abruptio placentae. ))
Risk of C. S. :
Maternal risk
Mortality after C.S. is 5-10X after normal vaginal delivery .
Immediate complications :
1. Anasthesia , aspiation (Mendelson’s syndrome)
2. Haemorrhage (blood transfusion and shock)
3. Injury to adjacent organs .
4. Infection , DVT , pulmonary embolism .
Fetal risk :
1. Risk of anasthesia .
2. Respiratory problems (transient tachypnea)
3. Intracranial haemorrhage (difficult delivery)
4. Prematurity ( inaccurate date ).
What we must do after CS as a doctor?
Check level of consciousness
Chart of vital signs
Use : antibiotis ,analgesia ,i.v fluid
calculate urine outcome
breast feeding
early mobilization
start oral intake
come in 7 days
give contraception
partogram
يقرأ من المحاضر ة
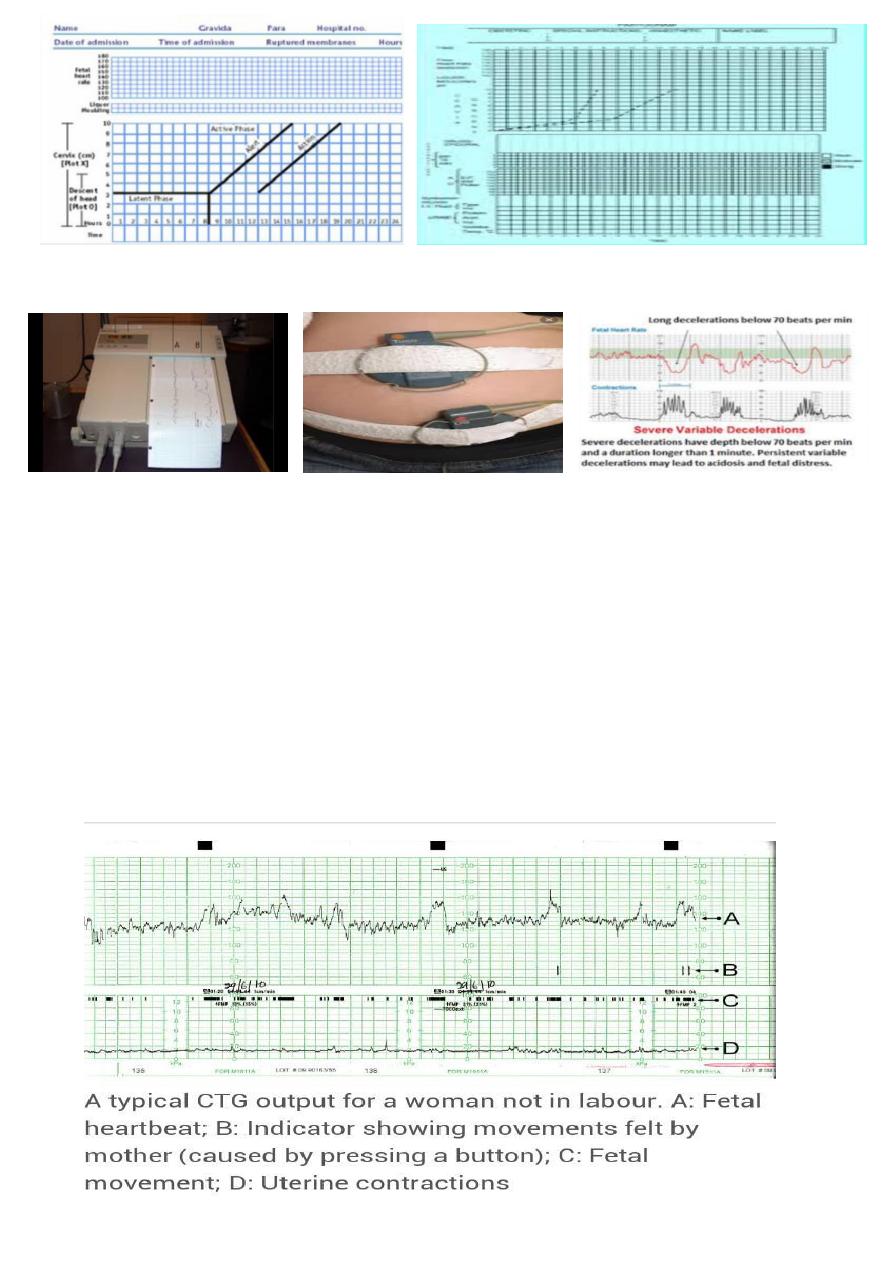
What is this ?
CTG
Character of normal CTG
1. 110 -160 bpm
2. two acceleration
3. no deceleration
4. baseline variability ± 5-15 bpm.
Abnormal CTG finding
1. persistent bradycardia (less than 110 bpm): fetal distress .
2. early deceleration (bradycardia on contraction) .
3. variable deceleration :cord compression.
4. Absence of Variable baseline :fetal heart rate is always change less than 5 or more than 15 .
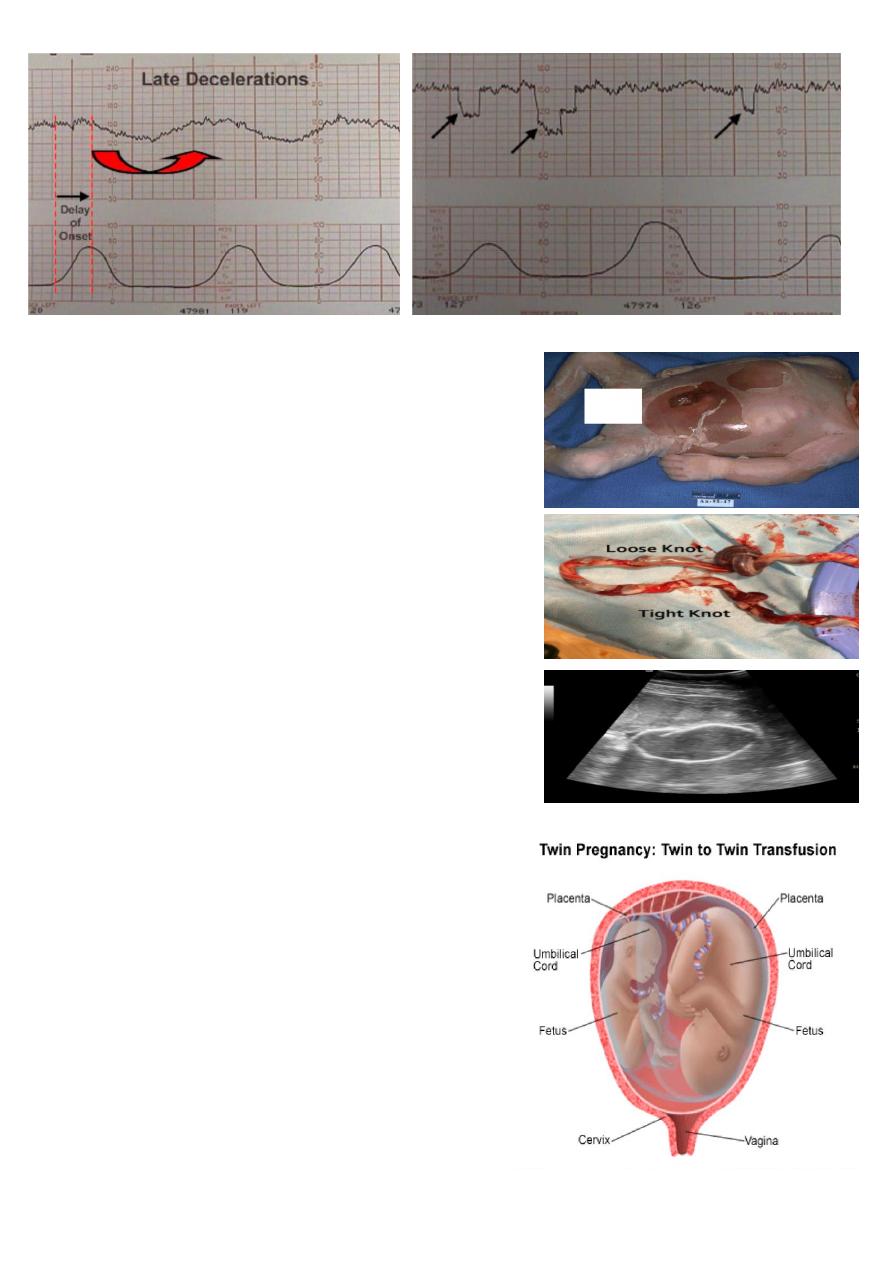
This is late deceleration .
What is your diagnosis ?
Macerated baby
Peeling skin, brown to blue color of the baby , hypotonic baby.
What is this ?
Cord accident (( cord knot ))
What is the result of this ?
Loss knot lead to deceleration .
Tight knot lead to Fetal death .
What is this ?
Ultrasonography for IUFD
What is showing ?
Spalding sign ( compressed skull ) .
What is the diagnosis ?
Twin-to-Twin transfusion syndrome (TTTS)
Caused by :
Imbalance in the flow of blood across these arteriovenous
communication result in twin-to-twin transfusion syndrome.
Complication :
The donor twin may become growth restricted and
oliguric with oligohydromnios.
The recipient fetus become hypervolaemic, leading to
polyuria and polyhydramnios.
There is a risk of myocardial damage and a high output
cardiac failure. It occurs in about 15 percent of twins
with a shared placenta.\
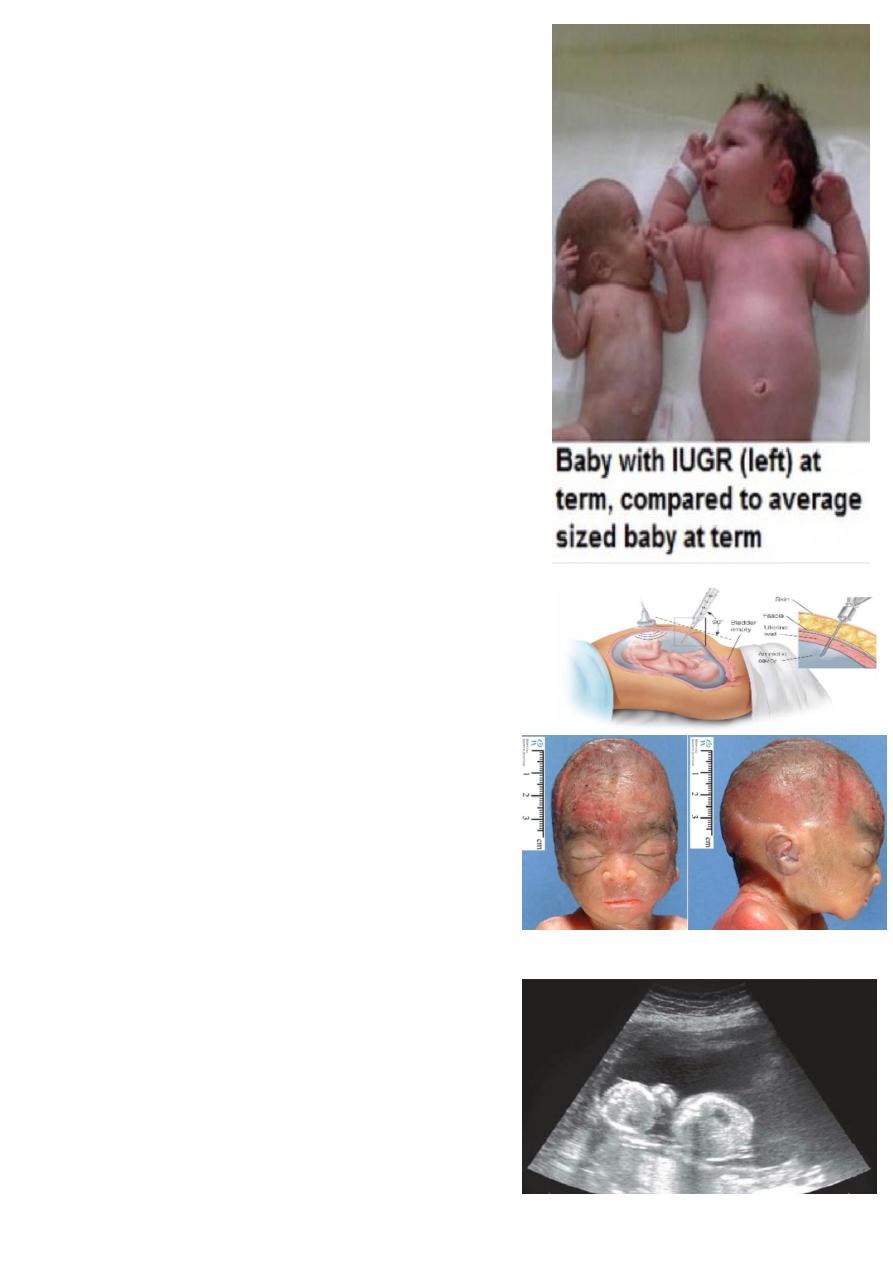
WHAT IS THE DIAGNOSIS ?
IUGR .
What the causes ?
Maternal factors
1-maternal disease (chronic respiratory dis.) ,, 2-malnutrition
3-ethinic & socio-economic factors ,,, 4-maternal hypoxemia
5-low pre-pregnancy weight ,,,,,, 6-primigravida . 7-drugs
Fetal factors
1-genetic disease ,,,,, 2-structural abnormalities
3-chromosomal abnormalities (trisomy 13،18 ،21)
4-cardiovascular disease
5-congenital infection (TORCH ) ,, 6-multiple pregnancy
Placental factors
1-reduced utero-placental perfusion( APS., DM, multiple gestation )
2-reduced feto-placental perfusion
Complication of IUGR :
* Antepartum complications
1-still birth. 2-oligohydromnios.
*During labour
1-meconium aspiration . 2-fetal distress . 3-intrapartum fetal death.
*Neonatal complications
1-hypoxic ischemic encephalopathy. 2-hypoglycemia.
3-hypocalcemia . 4-chronic intrauterine hypoxia ...polycythemia.
What this procedure ?
Amniocentesis.
What is the diagnosis ?
Potter syndrome
Flatten of face
Lung hypoplasia
Postural deformity
All are due to oligohydromnia
What is this ?
Ultrasound
Showing polyhydromnia
What is the diagnosis ?
Polyhydromnia ( by ultrasound :::: AFI> 20-24 or DVP of >8 cm )
Classification of severity
• Mild....DVP=8-12 cm
• Moderate.....DVP=12-15 cm
• Severe......DVP >15 cm .
What is the causes ?
1-Maternal ( DM ) .
2-Placental ( Chorioangioma of placenta. )
3-idiopathic.
4-Fetal
...Intestinal obstruction
...Impairment of swallowing due to CNS lesion
...Chromosomal abnormalities as trisomy 18
...Fetal polyuria
...Multiple gestation
...Fetal hydrops.
On clinical examination :
Dyspnea, vomiting , mobile fetus , large abdomen .
large for date uterus , abdomen may be tense, tender & fetal pools hard to palpate .
edema of abdominal wall & vulva.
the presentation is unstable.
it may be difficult to hear fetal heart beat.
Complications of polyhydromnios:
Fetal risks ( 1-perinatal mortality , 2-hypoxia ).
Maternal risks:
1-abdominal discomfort , 2-spontaneous preterm labour
3-spontaneous rupture of membrane 4-malpresentation & unstable lie.
5-PPH. 6-increase incidence of CS 7-higher incidence of pre-eclampsia .
What is the diagnosis ?
Oligohydromnia . ( by ultrasound AFI < 5 or DVP < 2cm )
What is the cause ?
1-preterm premature rupture of membrane
2-placental insufficiency
3-congenital fetal anomalies.
4-prolonged pregnancy or post-term.
5-maternal drugs as NSAID.
6-maternal complications as hypertension, dehydration, preeclampsia.
Assessment of oligohydromnia
HX ( HX of PPROM , post maturity , less fetal movement ).
Examination :
small for date uterus.
Fetal pools may be very obviously felt , the uterus "full of fetus".
fetal malpresentation
Complication of oligohydromnia :
Fetal risk (( 1-perinatal mortality , 2-pulmonary hypoplasia
3-skeletal deformities. Potter syndrome .
4-prematurity. 5-fetal distress. ))
Maternal risk (( 1-increase the risk of CS due to fetal distress secondary to either IUGR, cord compression .
2-high rate of physician intervention )).
What is your diagnosis ?
Fern test for pre-labour rupture of membrane .
Describe it ?
Estrogen in the amniotic fluid cause crystallization of the salt in
the amino fluid , so when it dried under microscope the crystal
resemble the blades of ferns .
Mention other tests ?
Nitrazine test , amino dye test , Aminsure test .
What is your diagnosis ?
PROM
What is the risk of this ?
If infection occur after 48hrs Called
Chorioaminonities : Is an inflammation of the fetal membranes
(amnion & chorion ) due to bacterial infection.
Clinical features (important).
1-maternal pyrexia > 38C°
2-maternal tachycardia >100 beats/min.
3-uterine tenderness
4-offensive vaginal discharge.
5-fetal tachycardia >160 beats/min.
6-raise C-reactive protein.
7-raise in maternal WBC count.
Delivered by :
Induction of labour avoid CS(( risk of infection )) + Antibiotic .
Complication :
A-maternal (( 1-septicemia , 2-infection in the pelvic region & abdomen. 3-endometritis . ))
B-newborn infant (( 1-sepsis , 2-meningitis , 3-respiratory problems.))
What is this ?
Artificial rupture of the membrane
Aminotomy :manipulation of the membranes cause prostaglandin release uterine
contractions, and cervical rippining
Risks associated with this procedure include:
1. umbilical cord prolapse or compression.
2. maternal or neonatal infection.
3. fetal heart deceleration.
4. bleeding from placenta previa or low-lying placenta.
5. possible fetal injury.
Before rupturing the membrane it is necessary to :
d empty her bladder
What is this ?
Aminohook
for artificial rupture of membrane.
What is this ?
Uterine sound
Aim ? to detect the length of uterine cavity.
What is this ?
Bakri balloon
Used to treat PPH .
What is this maneuver ?
Uterine compression
What is the indication ?
TO treat PPH .
How does it act ?
By compression on the bed of uterine and iliac vessels so
reduce blood loss
Mention one medical and surgical method to treat PPH?
Medical : oxytocin , misoprostol.
Surgical : ( bakri balloon , B-lynch suture , hysterectomy )
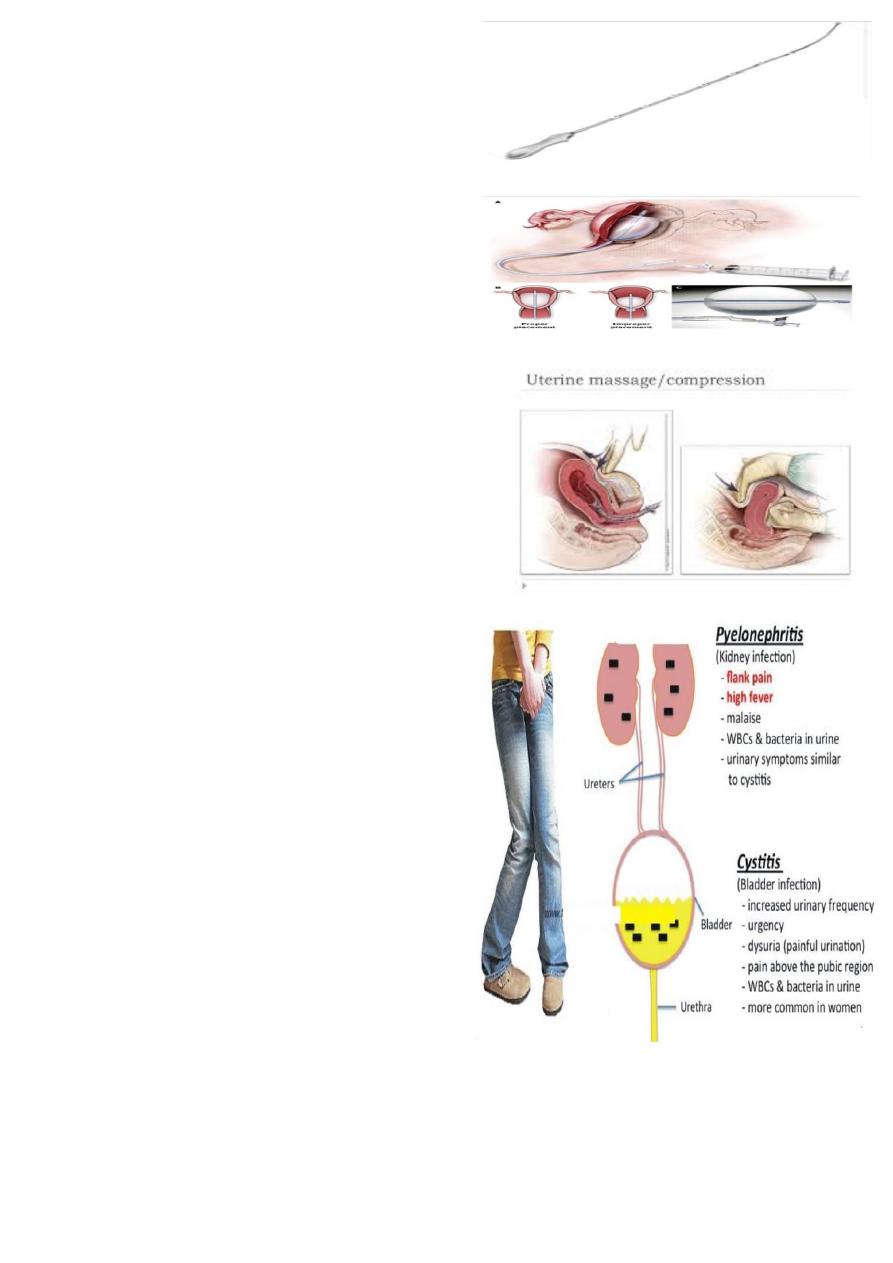
How to manage each of this ?
Treatment of cystitis
1-hydration to wash the bacteria.
2-antibiotics.
Types of antibiotics given;
Ampicillin, Amoxicillin, Augmentin, Nitrofurantoin.
Treatment of pyelonephritis :
Should be more aggressive;
1. admition to hospital "some patient can be managed as
outpatients" & bed rest
2. light diet & rehydration. IV fluid may be needed
3. analgesics & antipyretics.
4. alkalies as K citrate to inhibit the growth of E.coli.
5. antibiotics as ampicillin 500 mg/ 6hr or nitrofurantoin
100 mg/ 6hr or cephalosporins 500 mg/6hr untilthe
result of culture & sensitivity. The treatment is
continued for 7-10 days.
6. repeat culture after 2 wk.s.
Complications of pyelonephritis :
1-chronicity due to recurrent infections. In these cases, plain X-ray & IV pyelography should be done after delivery to
exclude urinary stones.
2-hypertension & renal failure(in chronic case).
3-pulmonary oedema & adult RDSdue to dehydration.
4-effect on fetus; abortion, preterm labour, prenatal mortality & morbidity.
What is this device ?
non-pneumatic anti-shock garment (NASG).
Why it used ?
used to treat hypovolemic shock, resuscitate, stabilize and prevent
further bleeding in women with obstetric hemorrhage.
What is this drug ?
Ergometrine.
Give to use ?
Used in
Active management of 3
rd
stage of labour
Treatment of PPH
Contraindication:-
hypertension
ischemic heart disease
varicose
What is this drug ?
Misoprostol (( prostaglandin E1 )).
indication ?
start labour
induction of abortion
treat post partum hemorrhage with oxytocin
Risks associated with the use of prostaglandins include:
1.uterine hyperstimulation
2. maternal side effects such as nausea, vomiting, diarrhea, and fever
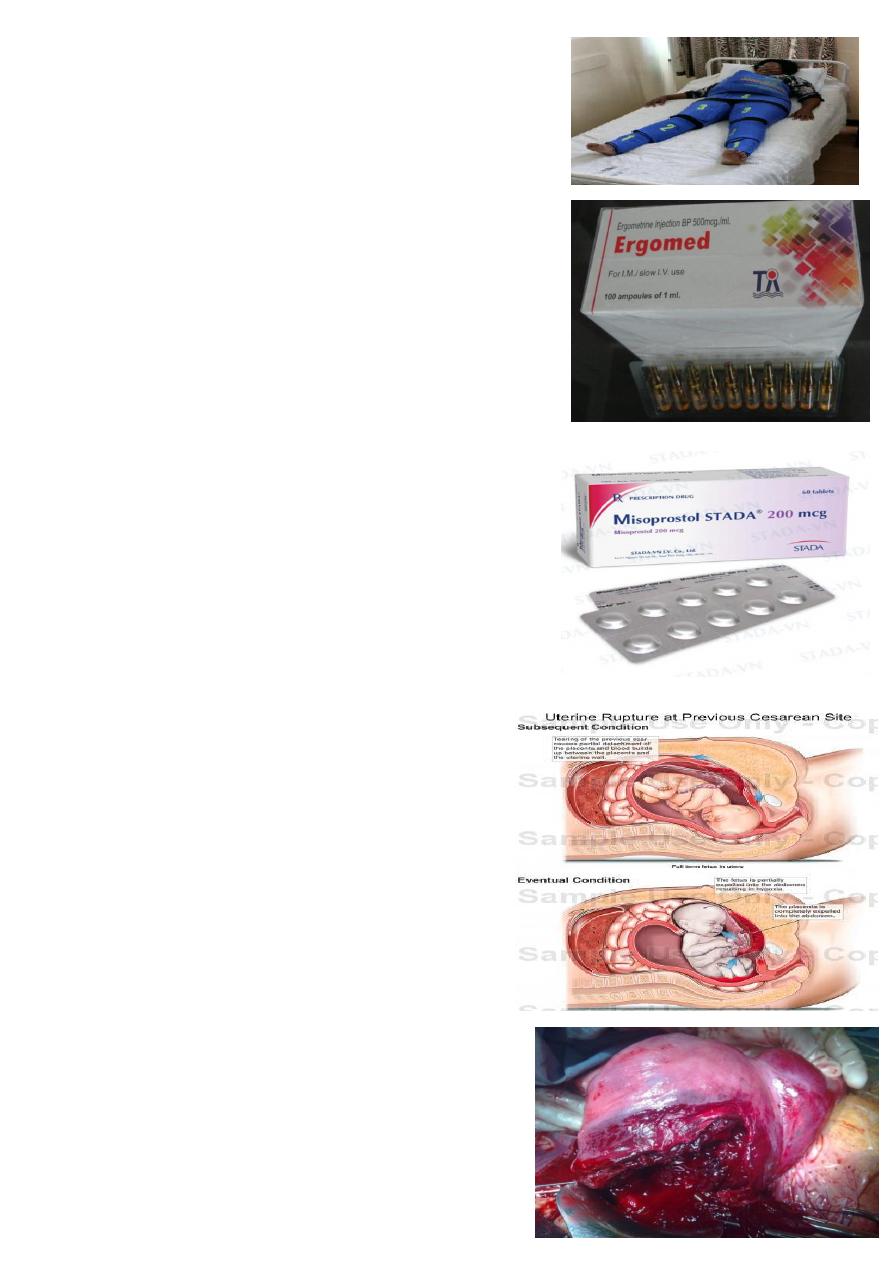
What is your diagnosis ?
Uterine rupture
What it's type ?
Complete : involve the peritoneum .
Incomplete : not involve the peritoneum
What is the cause ?
1)rupture of uterine scar . 2) external trauma . 3) obstructed
labour. 4) internal podalic version . 5) over dose oxytocin .
6) manual removal of palcenta .
Finding :
Impending : ( lower Abd pain , tender uterine scar , vaginal
spotting ).
At clinic : ( sudden sever Abd pain , shoulder pain , during
labour ;cessation of contraction )
On exam : ( FH –ve , fetal part dominant ,vaginal bleeding ).
Treatment :
1) ABC .
2) Laparotomy and Delivery .
3) Uterus : amenable for repair ( repair it ) , if not hysterectomy .
4) Internal iliac artery ligation .
5) Folly catheter and monitoring .
What is this ?
Broad ligament hematoma
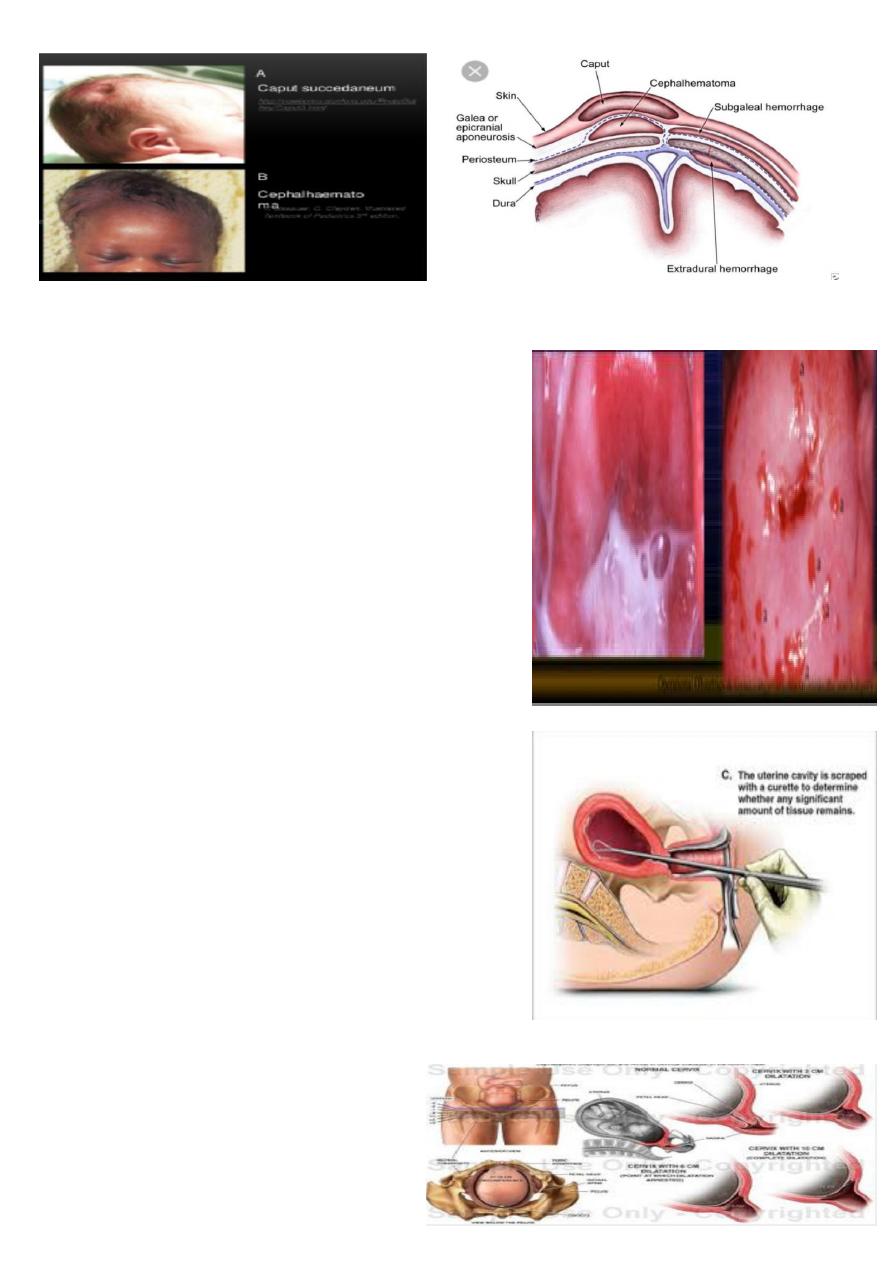
What is this ?
Degree of perineal laceration
What is your diagnosis ?
Hydrops fetalis baby .
Brown , hypotonic , peeling skin .
What is the causes ?
-HB deficit.
-portal hypertension Liver and spleen are enlarged
because of extra medullary hematopoiesis and
congestion.
-Hypoalbuminaemia secondary to liver dysfunction.
-Cardiac dysfunction .
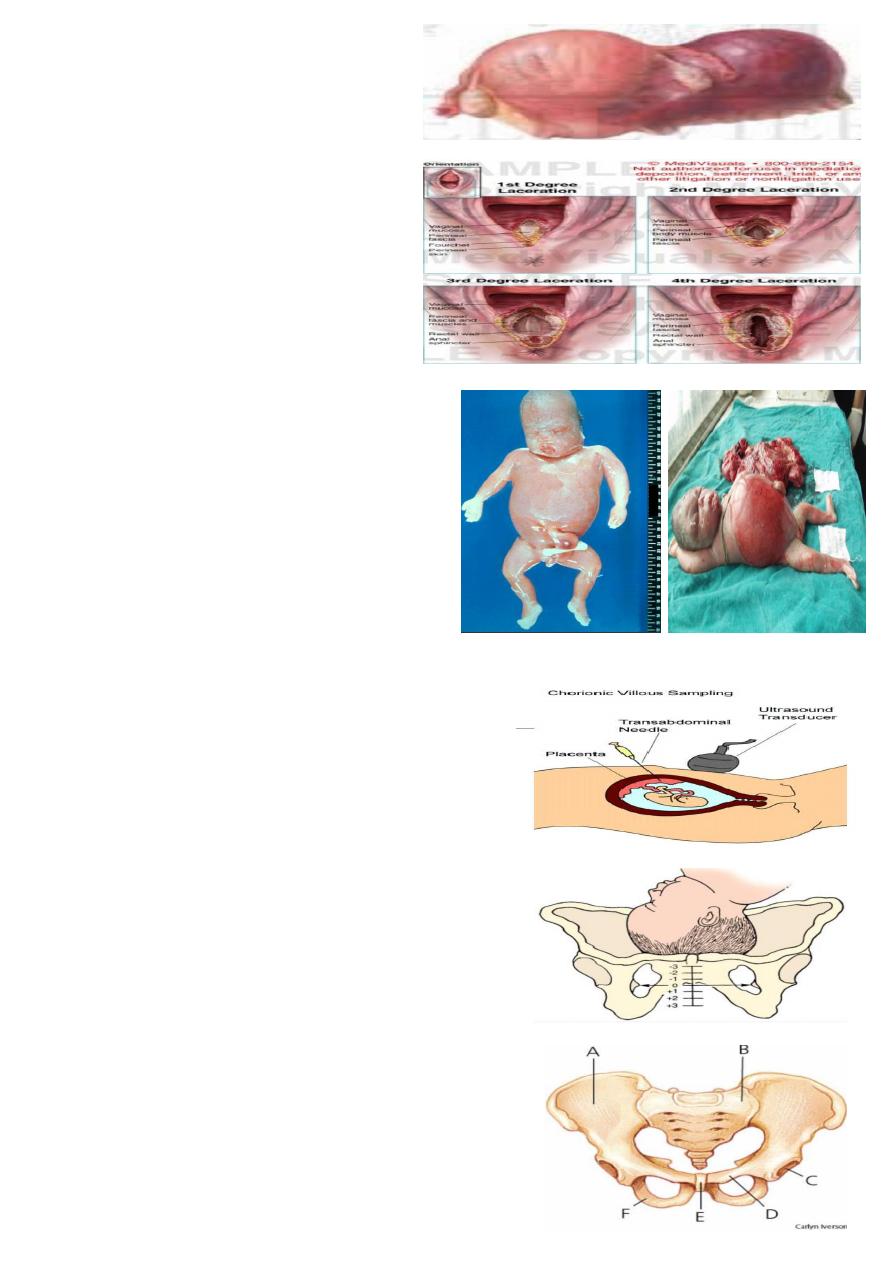
What is this procedure ?
Chorionic villous sampling . ( trans-cervically or abdominally )
usually done between weeks 10 and 13 of pregnancy
Indication for it ?
To determine chromosomal or genetic disorders in the fetus.
Complication of it ?
Risk of miscarriage 1-2%
Risk of infection and amniotic fluid leakage
What you seen ?
Head not engaged .
How we can determine head engaged or not ?
By rule of five
And by pelvic grip (one hand ).
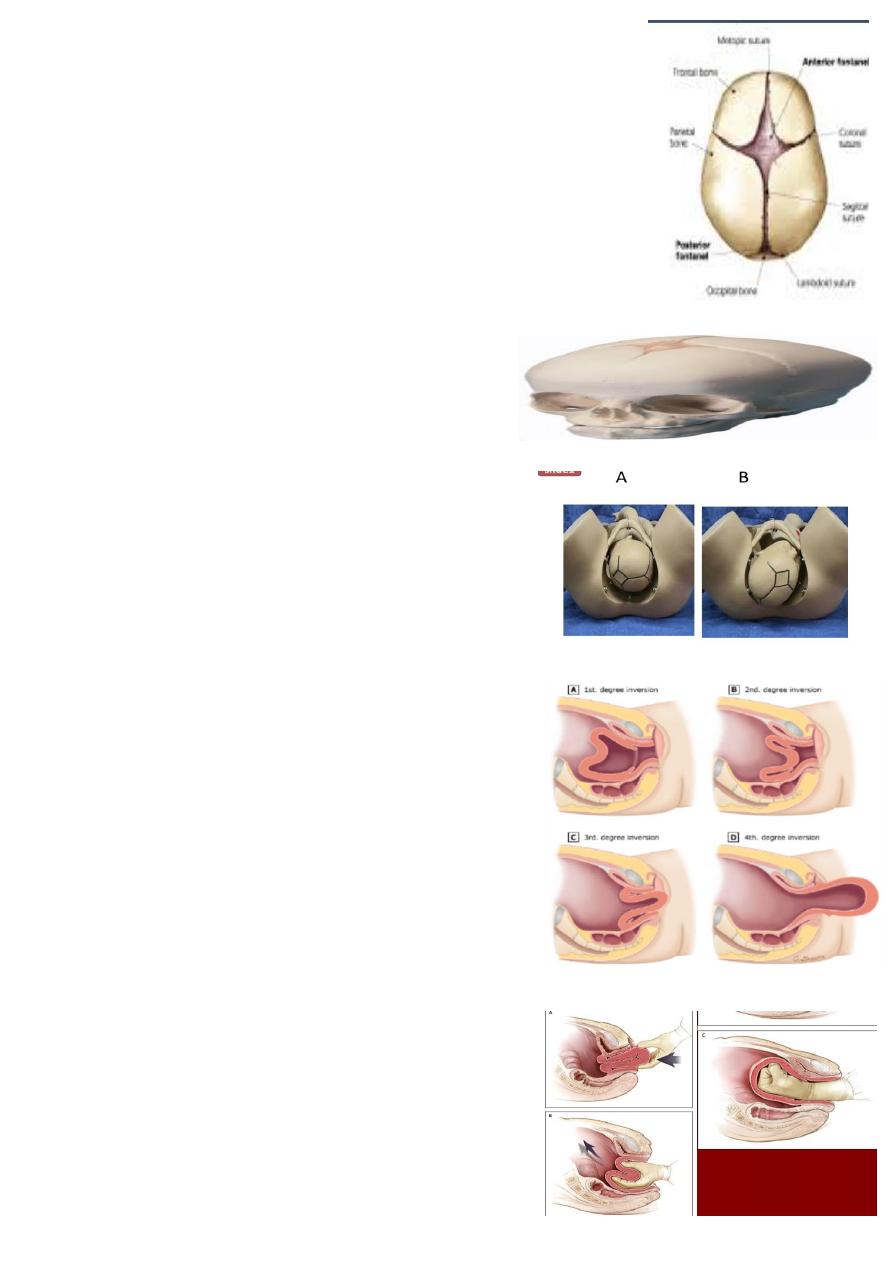
What IS the name of this pelvis ?
Gynecoid pelvis.
Mention other types of pelvis ?
Anthropoid pelvis
Android pelvis
Platypelloid pelvis
What is your diagnosis ?
Transverse lie baby.
ON Abdominal examination :
1. Small for date . 2. no presenting part .
3. On pelvic grip ( lateral position ) 4. FH +ve
5. the head on the right side . 6 . empty lower segment .
Two positions are described:
Dorsoanterior
Dorsoposterior
Aetiology:
Multiparity.
Prematurity.
Polyhydramnios.
Multiple pregnancy.
Contracted pelvis,placenta previa ,fibroid.
Uterine malformation
Treatment :
Caesarean section should be performed in persistant
transverse lie presentation.
Internal podalic version in delivery of second twin (transverse lie).
External cephalic version may be tried in selected cases before labour or in early labour .
In advanced labour or in case of ruptured membrane C.S. IS SAFER EVEN IN A CASE OF FETAL DEATH.
What is your diagnosis ?
RT and LF occiput position of the baby
Occipito –anterior position in majority of cases.
Occipitoposterior position in minority of cases.
What you seen in the picture ?
Flexion of the head .
What is this maneuver ?
External cephalic version.
Done AT 37-38wk
Carried in hospital equipped for emergency CS because
of the risk of placental abruption ,or cord compression .
Indiacation ?
breech presentation .
contraindication ?
Evidence of uteroplacental insufficiency.
Placenta previa.
Non reassuring fetal monitoring.
IUGR or oligohyraminos.
History of previous uterine surgery.
What is this picture showing ?
Fontanelle and Sutures of fetal skull.
The sutures :
SAGITTAL SUTURE lies between the superior borders of the parietal bones
FRONTAL SUTURE is a forward continuation of the sagittal suture, lies
between the two parts of frontal bone
CORONAL SUTURE lies between the anterior borders of the parietal bones &
the posterior borders of frontal bones.
The fontanelle :
ANTERIOR FONTANELLE: Lies where the sagittal, frontal & coronal sutures
meet, is diamond shaped is present at birth &takes about 20 months to close.
POSTERIOR FONTANELLE: Lies at the posterior end of the sagittal suture
between the two parietal bones & occipital bone. Is triangular in shape &it closed
soon after birth.
What is this ?
Fetal skull ( scalp )
Diamond in shape .
What is the diagnosis ?
A- Left occipito-tranverse.
B- Right occipito-posterior.
What is the causes of occipto-transvers ?
Cephalopelvic disproportion.
Platypelloid or android pelvis.
Relaxed pelvic floor due to multiparity and epidural anasthesia.
What is your diagnosis ?
Uterine inversion .
Degree of uterine inversion :
1st. degree (incomplete) inversion: the fundus is within the
endometrial cavity.
2nd. degree (complete) inversion: the fundus protrudes through
the cervical os.
3rd. degree inversion (uterine prolapse): the fundus protrudes to
or beyond the introitus.
4th. degree (total uterine and vaginal) inversion: both the uterus
and vagina are inverted.
Causes :
( uterine atony , increase intra-abdominal pressure ,
fundal attachment of placenta , placenta accrete )
What is this maneuver ?
Manual replacement of uterus .
How to perform it ?
To replace the 1
st
part which inverted last with placenta
attached to the uterus to it's normal place by steady firm
pressure by fingers .
Apply counter support by hand applied on abdomen .
Keep the fist of hand inside the uterus until it become
contracted after giving oxytocin or PGF2
What is this ?
Degree of cervical dilatation .
Two phases :
Latent phase : 3-4 cm dilatation .
Active phase : 4 cm to full dilatation 10 cm .
Cervical dilatation in hours :
In primi : 1cm every 1 hour
In multi : 2cm every 1 hour .
What is your diagnosis ?
Morbid adherence of placenta .
The degree of morbidity is determined by the depth of invasion.
Placenta accrete the placenta is partially or completely
adherent to the uterus with penetration of villi into the
superficial part of the myometrium.
Placenta increta the villi penetrate deeply through the
decidua into the myometrium.
Placenta percreta penetration can even be seen on the
serosal surface.
What is this ?
Manual removal of placenta .
How to deliver placenta manually ?
When a contraction is felt the left hand should be moved
suprapubically& the fundus is elevated with the palm facing
towards the mother.
At the same time the right hand should grasp the cord & exert
steady traction so that the placenta separates & delivered gently.
Then the placenta should be inspected for missing cotyledons or
a succenturiate lobe.
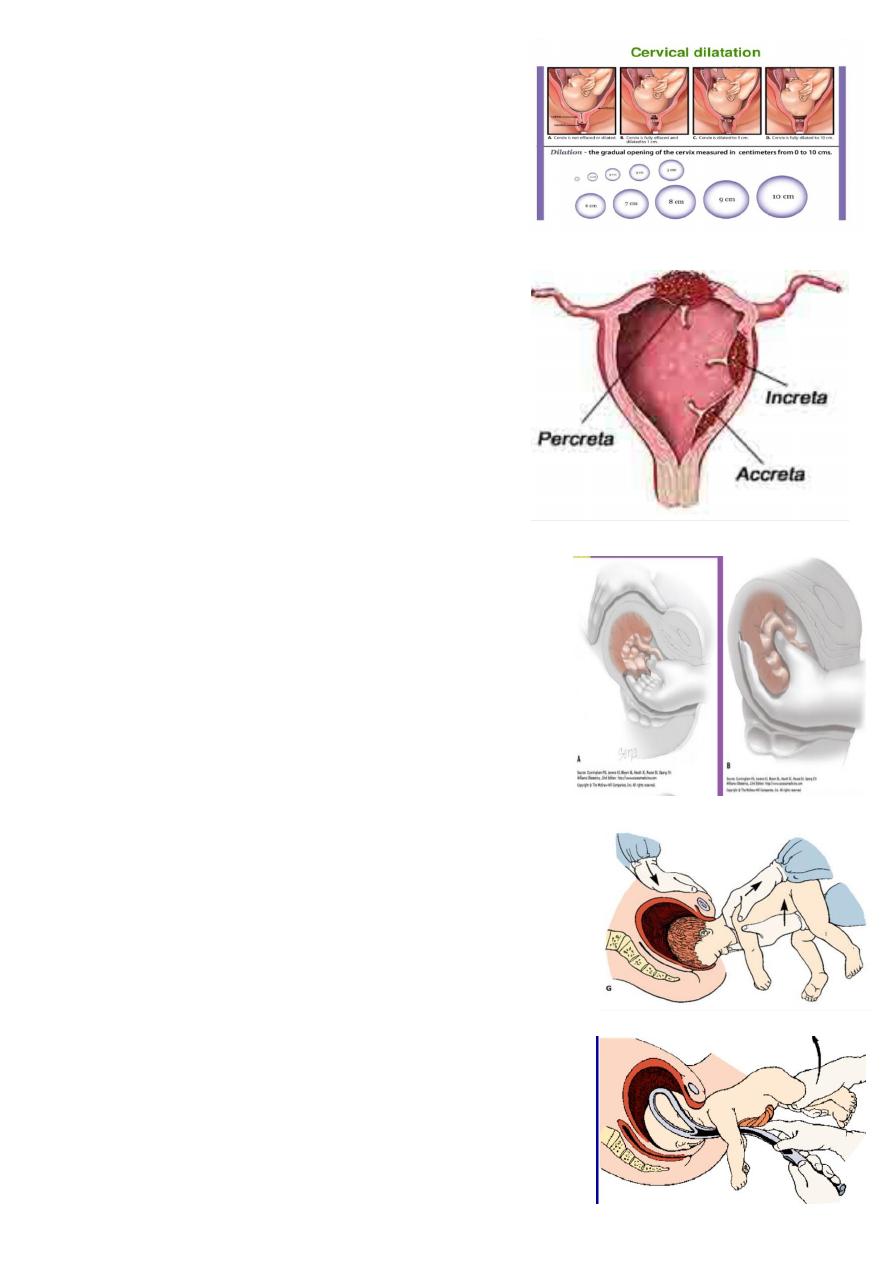
What is this ?
Breech presentation
Delivery of after coming head .
The fetal head is maintained in a flexed position by using the
Mauriceau-Smellie-Veit maneuver, which is performed by placing
the index and middle fingers over the maxillary prominence on
either side of the nose. The fetal body is supported in a neutral
position with care to not overextend the neck.
What is this ?
Assisted vaginal breech delivery
Using (( forceps )) .
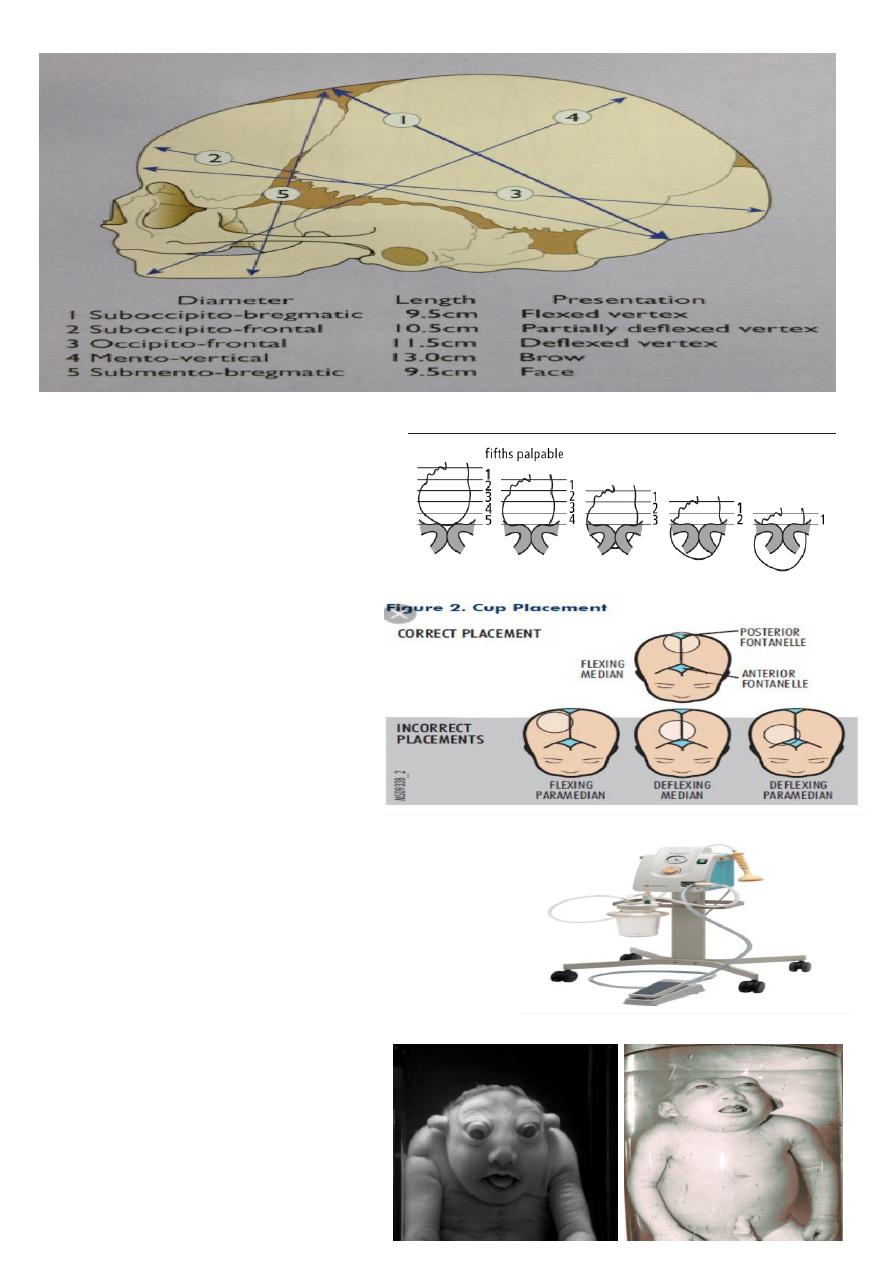
Diameter of skull .
What is this ?
Degree of head descent
Which is palpable in abdomen by rule of five
What is this ?
Correct and incorrect cup placement .
What is this ?
Vacuum extractor
Types :
( rigid and soft )
Used : for assisted vaginally delivery .
What is the diagnosis ?
Anencephaly
What is the cause ?
Cephalic disorder due neural tube defect if the
mother not use folic acid .
On examination :
Polyhydromnia due to exposed CSF in the
extra fluid .
Head injuries caused by instrumental delivery ( forceps and vacuum ).
What is the diagnosis ?
Cervical infection (( trichomonas vaginalis )).
Signs & Symptoms
Asymptomatic in 10–50%, but may present with:
• Frothy,yellowish green, offensive smelling vaginal discharge.
• Vulval itching and soreness.
• Dysuria.
• Cervix may have a ‘strawberry’ appearance from punctate
haemorrhages (2%).
Management
Both partners should be treated and both should be screened for
other sexually transmitted infections.
• Metronidazole 2g orally in a single dose.
• Metronidazole 400mg bd for 5–7 days.
• Tinidazole in a single oral dose of 2 g
What is this procedure ?
Curettage .
Used in :
To remove missed Abortion and retained piece of placenta .
Complications of curettage:
1-Immediate :
• -haemorrhage.
• -uterine perforation.
• -cervical injury.
2-Delayed:
• -infection.
• -retained tissue.
3-late:
• .Asherman's syndrome (intrauterine adhesions).
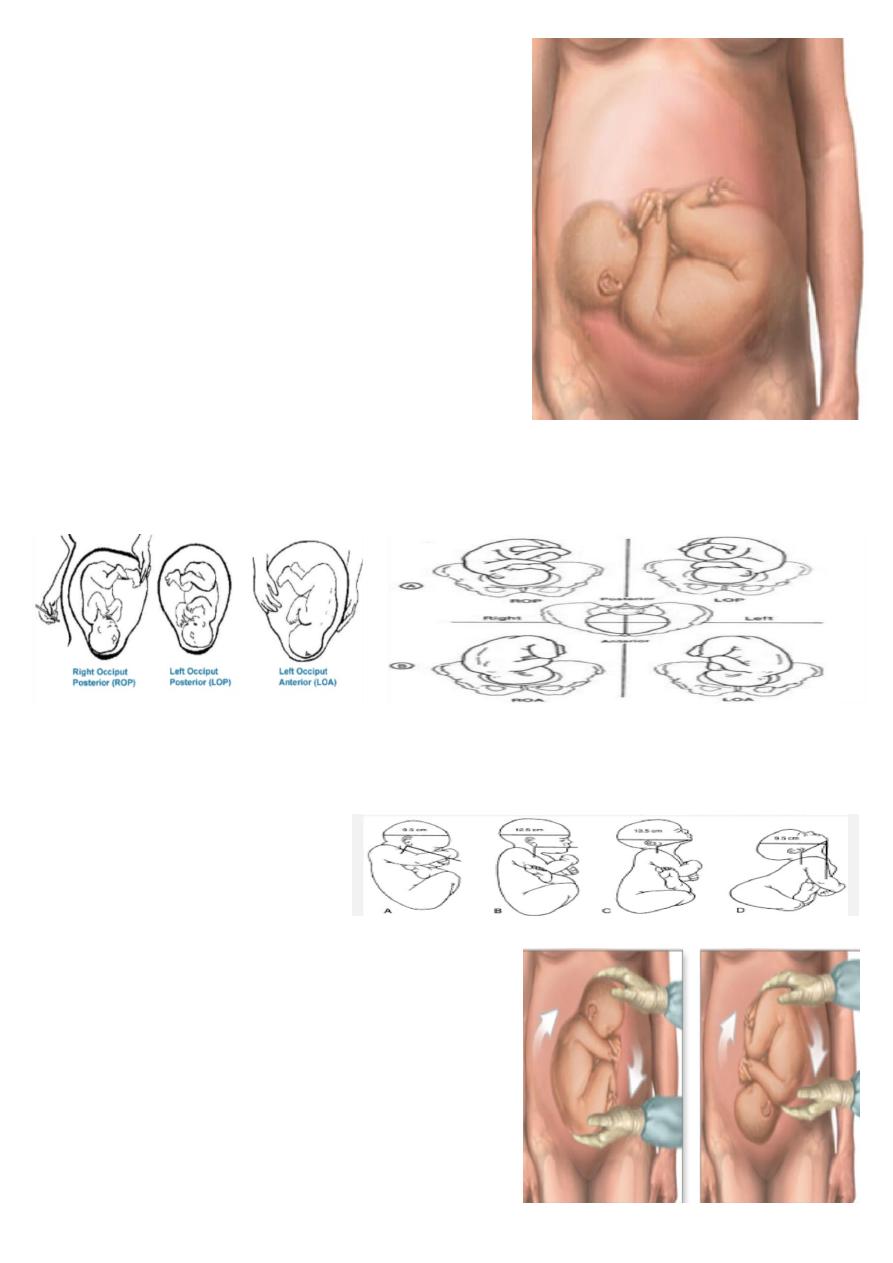
What is this picture showing ?
Showing :
1) normal and degree of cervical dilatation.
2) station of the head .
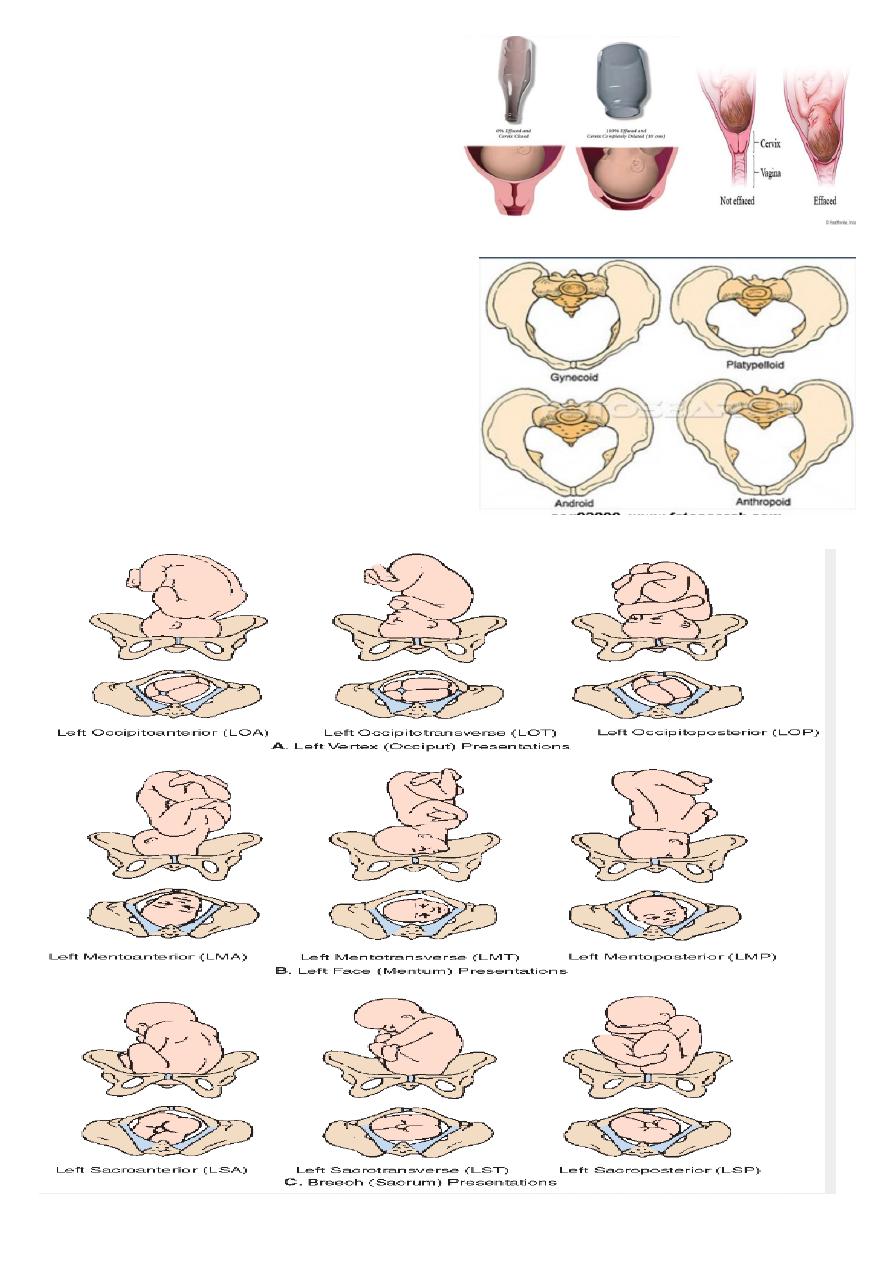
what is picture showing ?
showing :
cervical dilatation and effacement.
What is this ?
Type of pelvis .
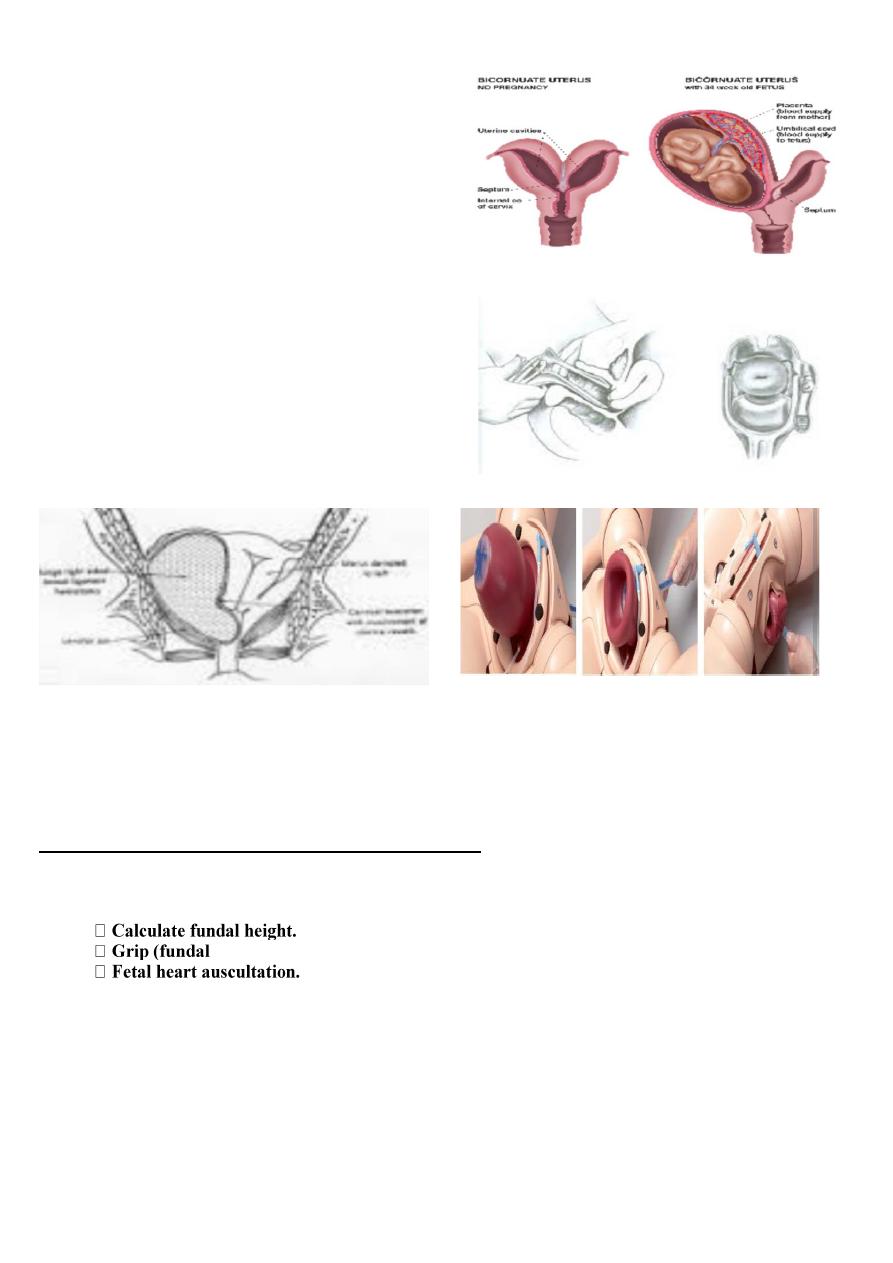
What is this ?
Bicornuate uterus
(with and without fetus )
Risk of Bicornuate uterus ?
• Recurrent pregnancy loss .
• Preterm birth .
• Malpresentation .
What is this ?
Vaginal speculum and colposcopy for pap smear .
I DON’T KNOW WHAT IS THESE 2slides
اللي يعرفهم يجاوبهم
Important questions in clinic >>
What is your finding in abdominal examination ?
You should write about each presentation ( beech , cephalic ,transverse …… ETC )
Obstetric finding in abdominal examination
•
•
,lateral ,pelvic)
•
AND
FINALLY DONE
………………….
BEST WISHES TO ALL MY COLLEGUES