Viral meningoencephalitis

Viral meningoencephalitis is the most common cause of CNS infection Et .
• Enteroviruses are the most common cause of viral• meningoencephalitis. It spread directly from person to person
• Herpes simplex virus type 1 (HSV-1) is an important cause
• of severe sporadic encephalitis. Brain involvement usually is
• focal .
• Herpes simplex virus type 2 (HSV-2) may cause severe encephalitis with diffuse brain involvement in neonates .
• Varicella-zoster virus (VZV) may cause CNS infection (especially cerebellar ataxia) in associated with chickenpox.
CLINICAL MANIFESTATION
• The onset is generally acute, CNS signs and symptoms are preceded by a nonspecific febrile illness of a few days' duration.• In the infant the presenting manifestations are irritability and lethargy.
• In older children are headache (frontal or generalized) and hyperesthesia.
• adolescents frequently complain of retrobulbar pain. Fever, nausea and vomiting, photophobia, and pain in the neck, back, and legs are common.
Other manifestations include:
Focal neurologic signs may be present, especially in HSV-1 which cause sever encephalitis, progression to coma & death occurs in 70% of cases without antiviral treatment.
Loss of bowel and bladder control may occur. Skin rash may occurs with enteroviruses & measles infection.
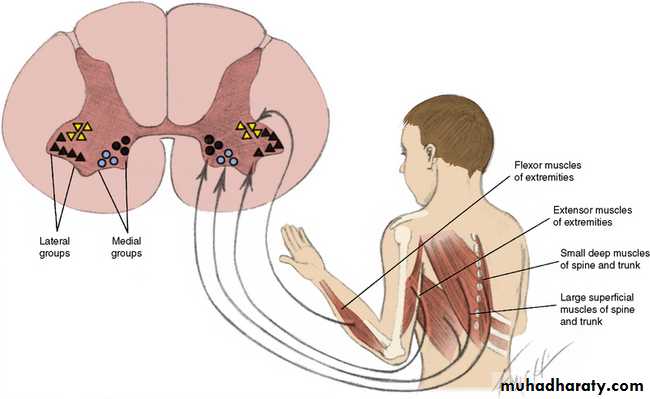
Enteroviruses may cause anterior horn cell injury and
acute flaccid paralysis.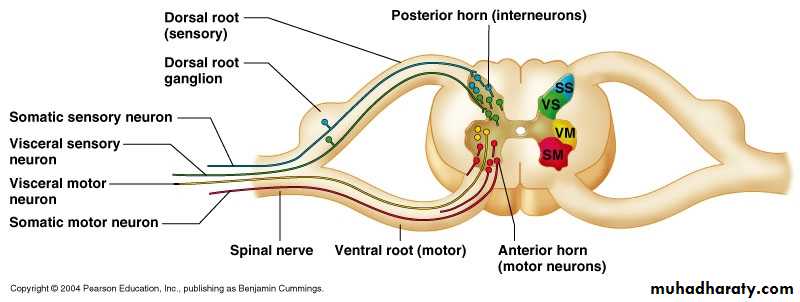
Investigations
• CSF exam• Serology of blood may be useful in determining of some viral CNS infection e.g. arboviral infection, but it is of no value in Enteroviruses.
• EEG show diffuse slow wave activity.
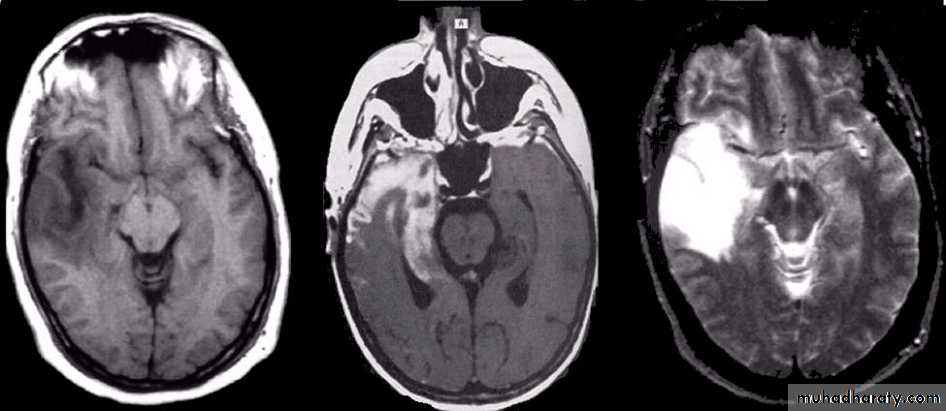
• CT & MRI show swelling of brain parenchyma.
Note: HSV encephalitis is suggested by focal seizures & focal finding on EEG, CT, or MRI especially if involve the temporal lobe.
Treatment
HSV encephalitis is treated with IV Acyclovir , for 2-3 wk.Otherwise, Treatment of viral meningoencephalitis is supportive.
Mild disease may require only symptomatic relief. More severe disease may require hospitalization and intensive care.
• Headache and hyperesthesia are treated with rest, non–aspirin- containing analgesics & reduction in room light, noise, and visitors.
• Fever ; acetaminophen.
• Vomiting ; phenothiazine.
• Poor oral intake ; IV fluids .
• Total parenteral nutrition
• may be required in prolonged coma.

Complications Guillain-Barre syndrome, Transverse myelitis, Hemiplegia, and Cerebellar ataxia.
Prognosis
Most children recover completely from viral infections of the CNS, especially those due to enteroviruses, whereas others have high mortality rate e.g. HSV.
severe sequelae e.g. epileptic, visual, or auditory.
Prevention
Isolation of cases, vaccination is available for some viruses e.g. varicella, & measles .
Neurocutaneous Syndromes
The neurocutaneous syndromes include a heterogeneous group of disorders characterized by abnormalities of both the skin and central nervous system (CNS).
These syndromes include:
NeurofibromatosisTuberous sclerosis
Sturge-Weber disease
Neurofibromatosis(NF)
NF is a common• autosomal dominant
• Clinical manifestations and Diagnosis:
• There are two forms of NF:
• NF-1: is the most prevalent type (90%).
• The NF-1 gene located on chromosome region 17q11.
• It is diagnosed when any two of the following seven
• signs are present:
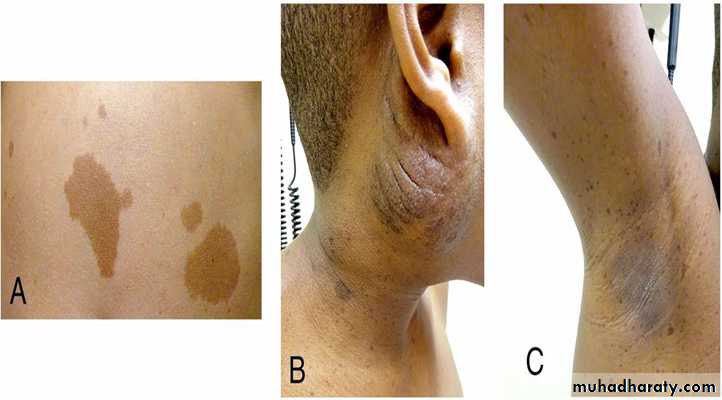
1- Six or more caféau-lait spots over 5 mm in diameter in pre pubertal individuals and over 15 mm in greatest diameter in post pubertal individuals.
Café au-lait spots are the hallmark
of neurofibromatosis and are presentin almost 100% of patients.
They are present at birth but increase in size, number, and pigmentation, especially during the 1st few years of life.
The spots are scattered over the body surface, mainly the trunk and extremities, and with sparing of the face.

2- Axillary or inguinal freckling
• consisting of multiple hyperpigmented• areas 2–3 mm in diameter.
3- Two or more iris Lisch nodules.
• Lisch nodules are hamartomas
• located within the iris and are best
• identified by a slit-lamp examination.
• They are present in >74% of patients with NF-1.


4- Two or more neurofibromas or one plexiform neurofibroma. Neurofibromas typically involve the skin, but they may be situated along peripheral nerves appear
• characteristically during adolescence .
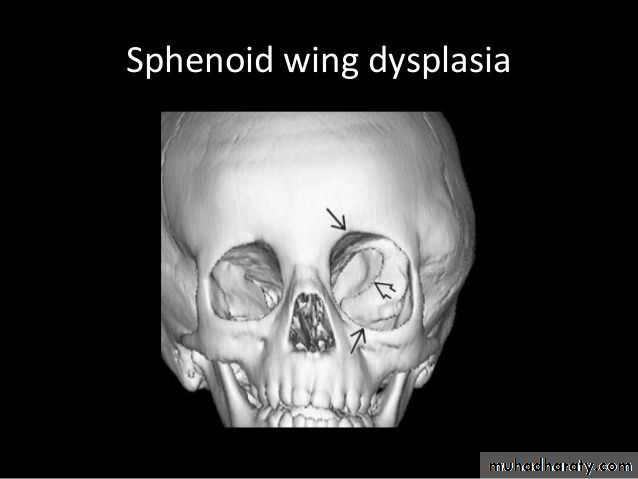
5- A distinctive osseous lesion such
• as sphenoid dysplasia (which may• cause exophthalmos) or Scoliosis.

• 6-Optic gliomas are
• present in ≈15%• of patients ,
• ≈20% have visual
• disturbances .
7-A first-degree relative with NF-1.

Children with NF-1 are susceptible to:-
1.Neurologic complications & cognitive abnormalities like learning disabilities and abnormalities of speech.• These are common and occur in 40–60% of NF-1 children.
• Complex partial and generalized tonic-clonic seizures are a frequent complication.
• 2.The cerebral vessels may develop aneurysms, or stenosis.
• 3. Psychologic disturbances.• 4. Precocious puberty
• 5. Malignant neoplasms are a significant problem in patients with NF-1. A neurofibroma occasionally differentiates into a neurofibrosarcoma or malignant schwannoma.
• 6.Patients with NF-1 are at risk for hypertension, which may result from renal vascular stenosis or a pheochromocytoma.
• NF-2: accounts for 10% of all cases of NF . The gene for NF-2 is located near the center of the long arm of chromosome 22q1.11.
• It is diagnosed when one of the following two features is present:
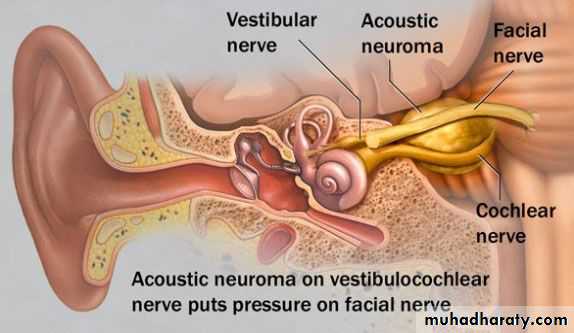
• 1- Bilateral eighth nerve masses
• (Bilateral acoustic neuromas)
• as demonstrated by CT scanning
• or MRI.
• 2- A parent, sibling, or child with
• NF-2

• Treatment &Prevention
• Because there is no specific treatment for NF, management includes:• 1-Genetic counseling: A parent with NF has a 50% chance of transmitting the disease with each pregnancy. each parent should be carefully examined before counseling for the risk of affected future pregnancies
• 2-Early detection of treatable conditions or complications.
• Tuberous Sclerosis
• Tuberous sclerosis (TS)• is inherited as an
• autosomal Dominant
• TS is an extremely heterogeneous disease with a wide
• clinical spectrum varying from severe mental retardation and seizures to normal intelligence and a lack of seizures.
• The disease affects many organ systems other than the skin and brain, including the heart, kidney, eyes, lungs, and bone.

• DIAGNOSIS
• TS is diagnosed when at least two major or one major plus two minor features are present.• *Major features include skin lesions, brain , eye lesions, and tumors in the heart, kidneys, or lungs.
• *Minor features include bone cysts, rectal polyps, dental enamel pits, CNS white matter abnormalities, gingival fibromas, retinal patches, and multiple renal cysts.
• Clinical manifestations:
• *Skin lesions• 1-Ash leaf spots which are hypomelanotic macules on the trunk and extremities. Present in more than 90% of cases. At least three macules must be present.
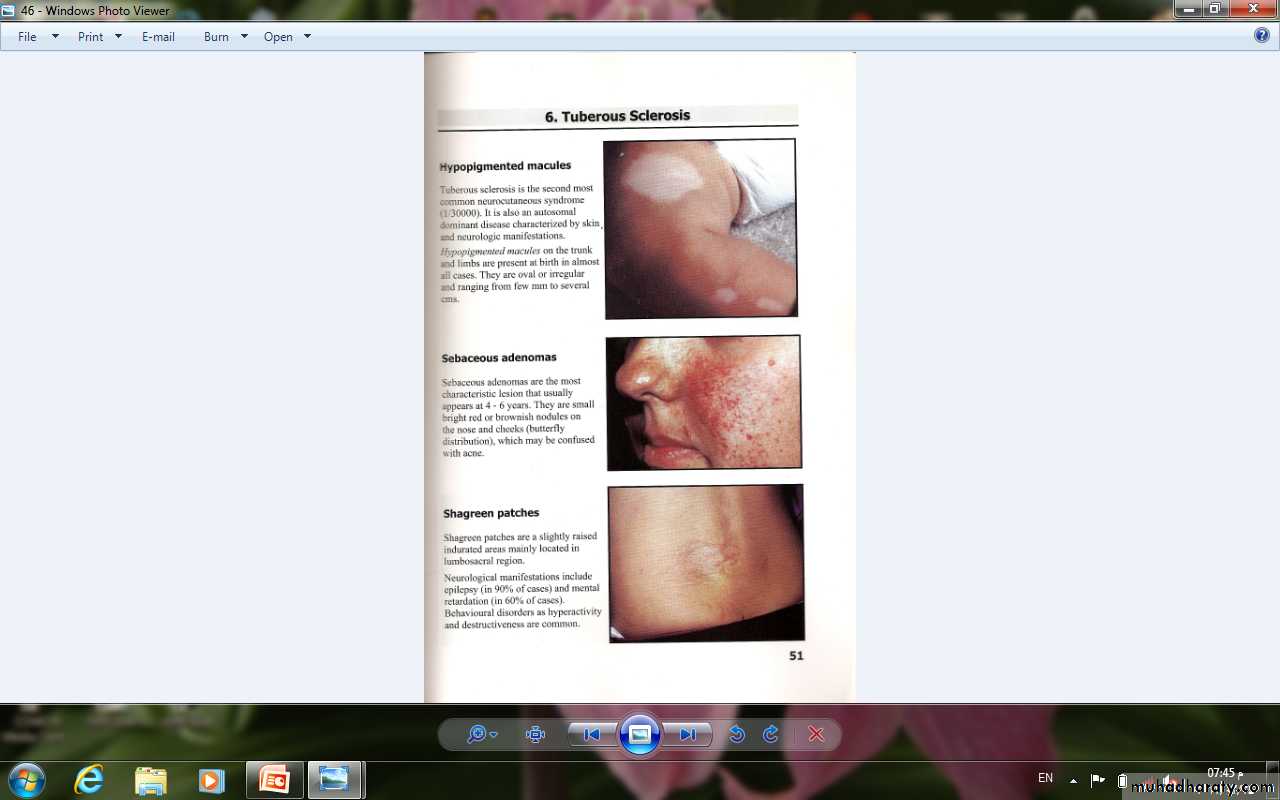

• 2-Sebaceous adenomas develop between 4 and 6 yr of age; they appear as tiny red nodules over the nose and cheeks and are sometimes confused with acne.
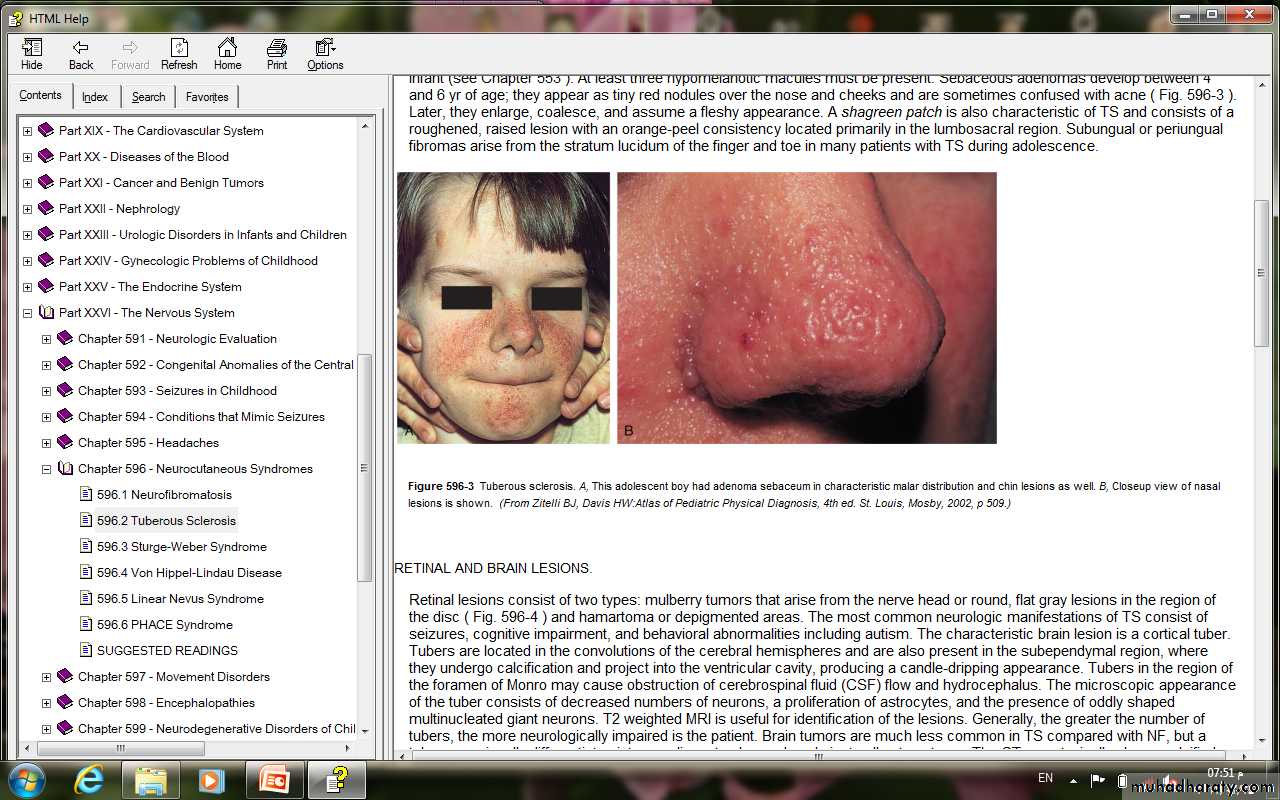
• 3-Shagreen patch is consists of a roughened, raised lesion located primarily in the lumbosacral region.


• 4-Subungual or periungual fibromas
• of the finger and toe in many patients with TS during adolescence.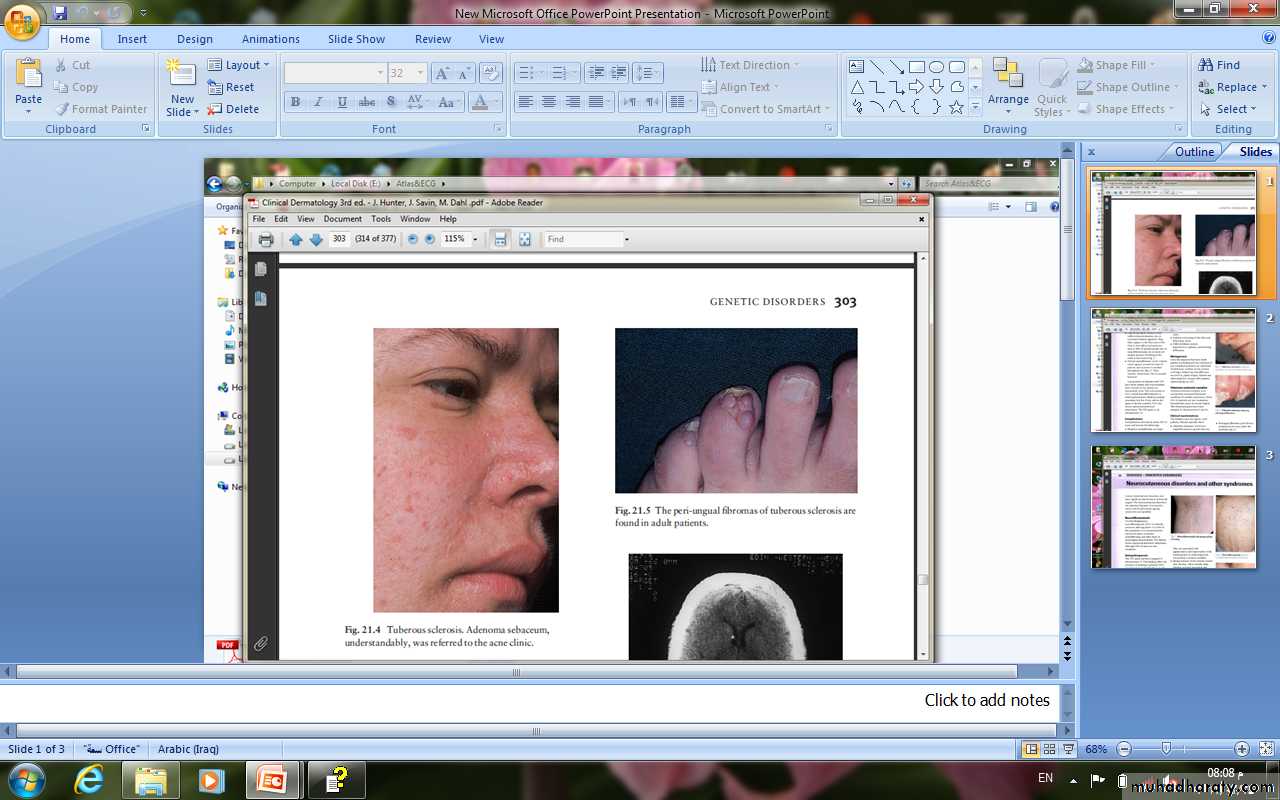
• 6.Retinal & Brain lesions
• Retinal lesions consist of two types: mulberry tumors that arise from the nerve head or round and hamartoma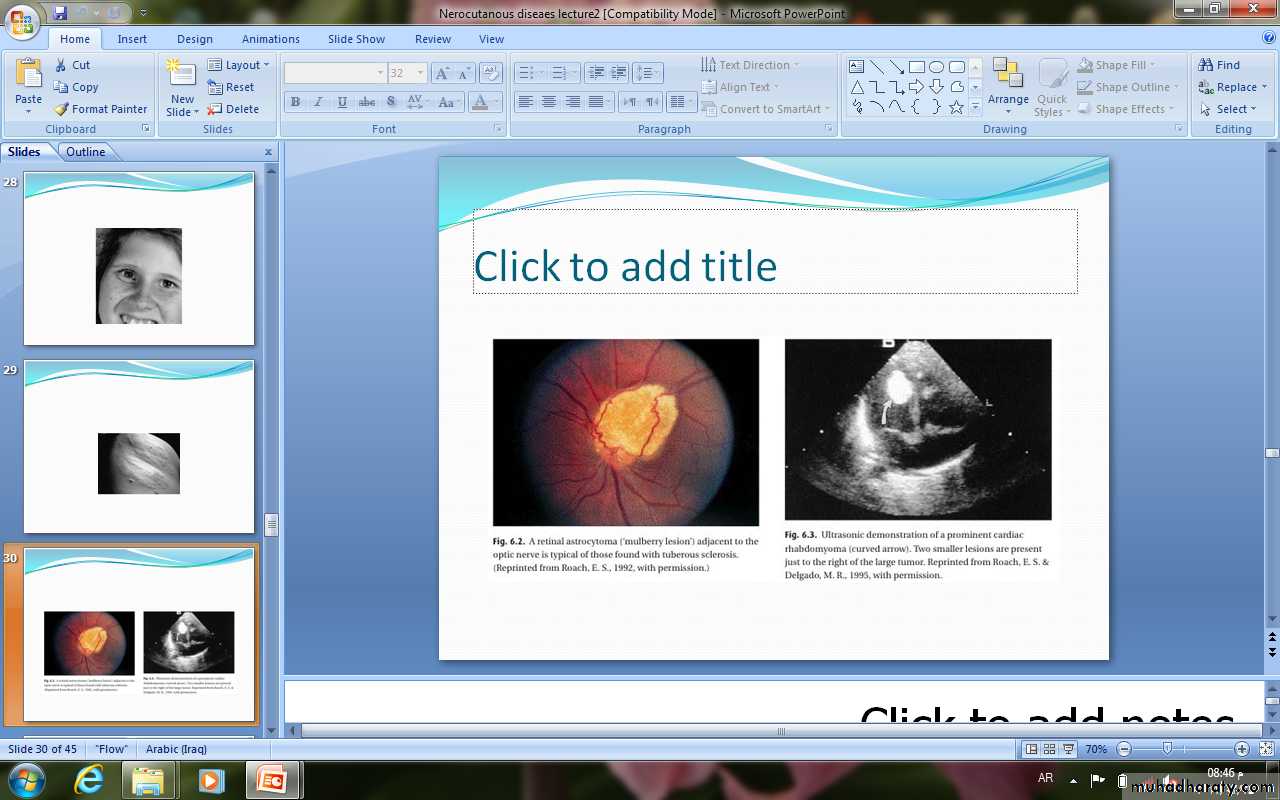
• The characteristic brain lesion is a cortical tuber.
• Tubers in the region of the foramen of Monro may cause obstruction of CSF flow and hydrocephalus.• MRI is useful for identification of the lesions.
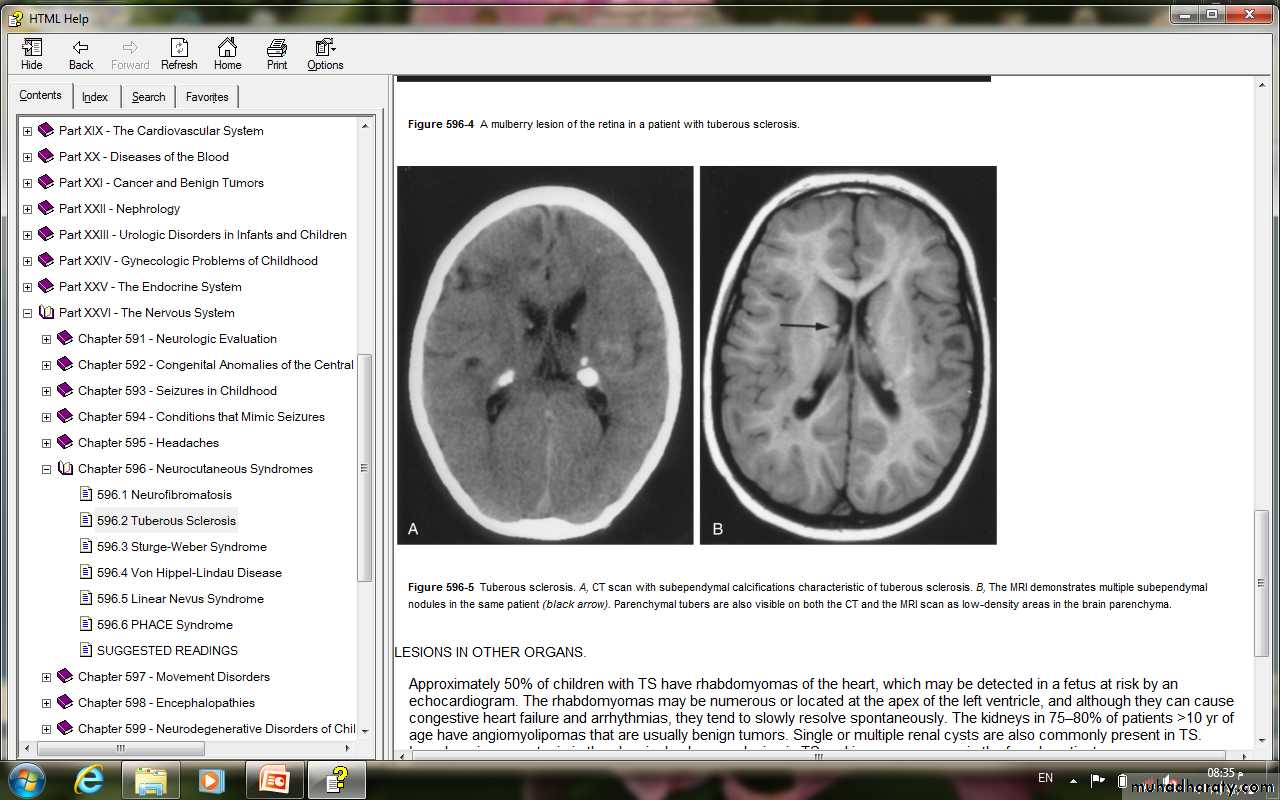
• Brain tumors are much less common in TS compared with NF
• Approximately 50% of children with TS have• rhabdomyomas of the heart.
• The kidneys in 75–80% of patients >10 yr of age have angiomyolipomas that are usually benign tumors. Single or multiple renal cysts are also commonly present in TS.
• Sturge-Weber Syndrome
• This syndrome is a sporadic disorder and consists of a constellation of symptoms and signs including a facial nevus (port-wine stain), seizures, hemiparesis, stroke like episodes, intracranial calcifications, and, in many cases, mental retardation.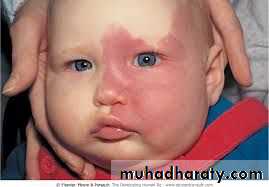
• Clinical manifestations
• *The facial nevus (port-wine stain)• is present at birth, tends to be
• unilateral, and always involves
• the upper face and eyelid.
• Glaucoma of the ipsilateral
• eye is common complication.
• *Seizures develop in most patients in the 1st year of life. They are typically focal tonic-clonic and contralateral to the side of the facial nevus. The seizures may become refractory to anticonvulsants and are associated with a slowly progressive hemiparesis in many cases.

• Neurodevelopment appears normal in the 1st year of life but mental retardation or severe learning disabilities are present in at least 50% in later childhood.
• Diagnosis
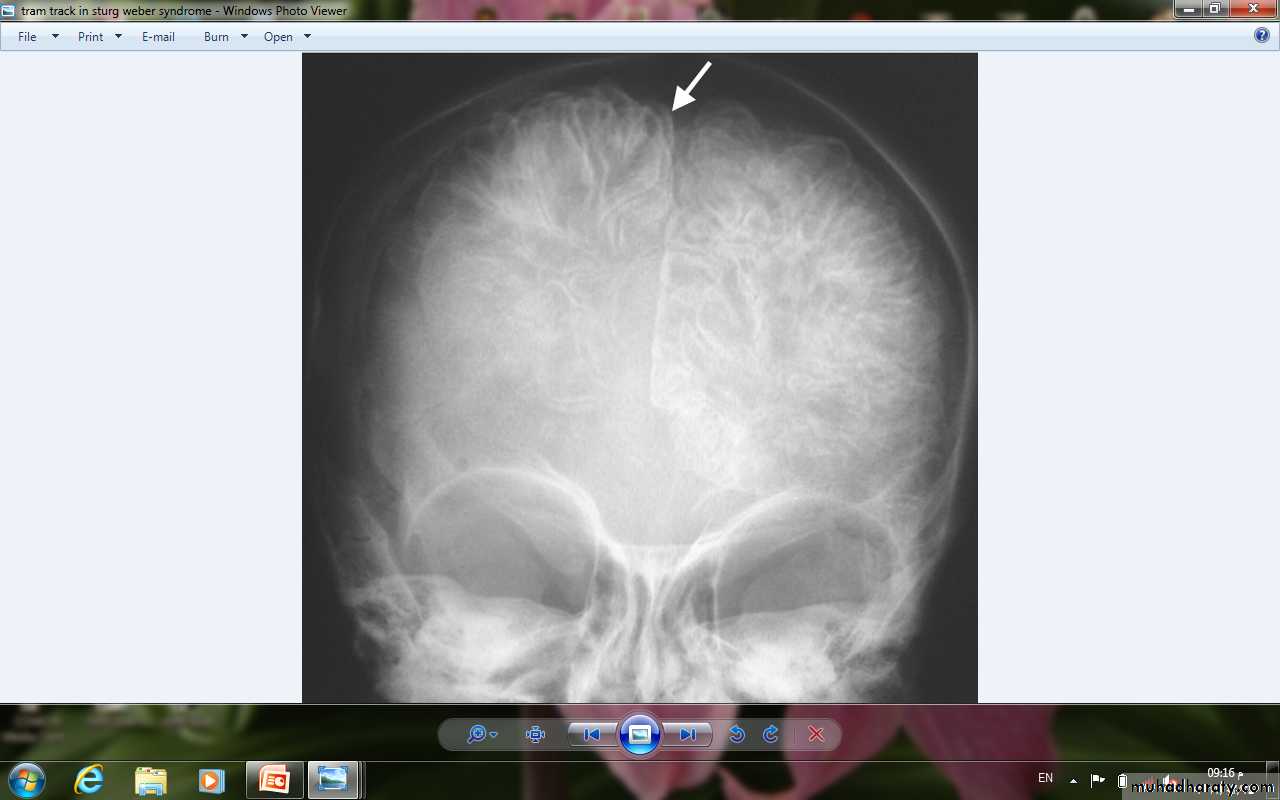
• 1- Skull x-ray: shows intracranial calcification in the occipitoparietal region in most patients. This characteristically assumes railroad-track appearance.
•
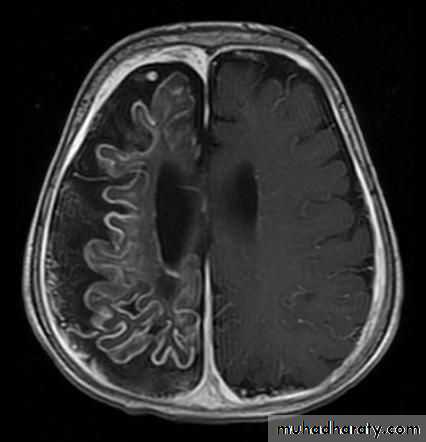
• 2- Brain CT scan: to detect the extent of the calcification that is usually associated with unilateral cortical atrophy and ipsilateral dilatation of the lateral ventricle.

CT
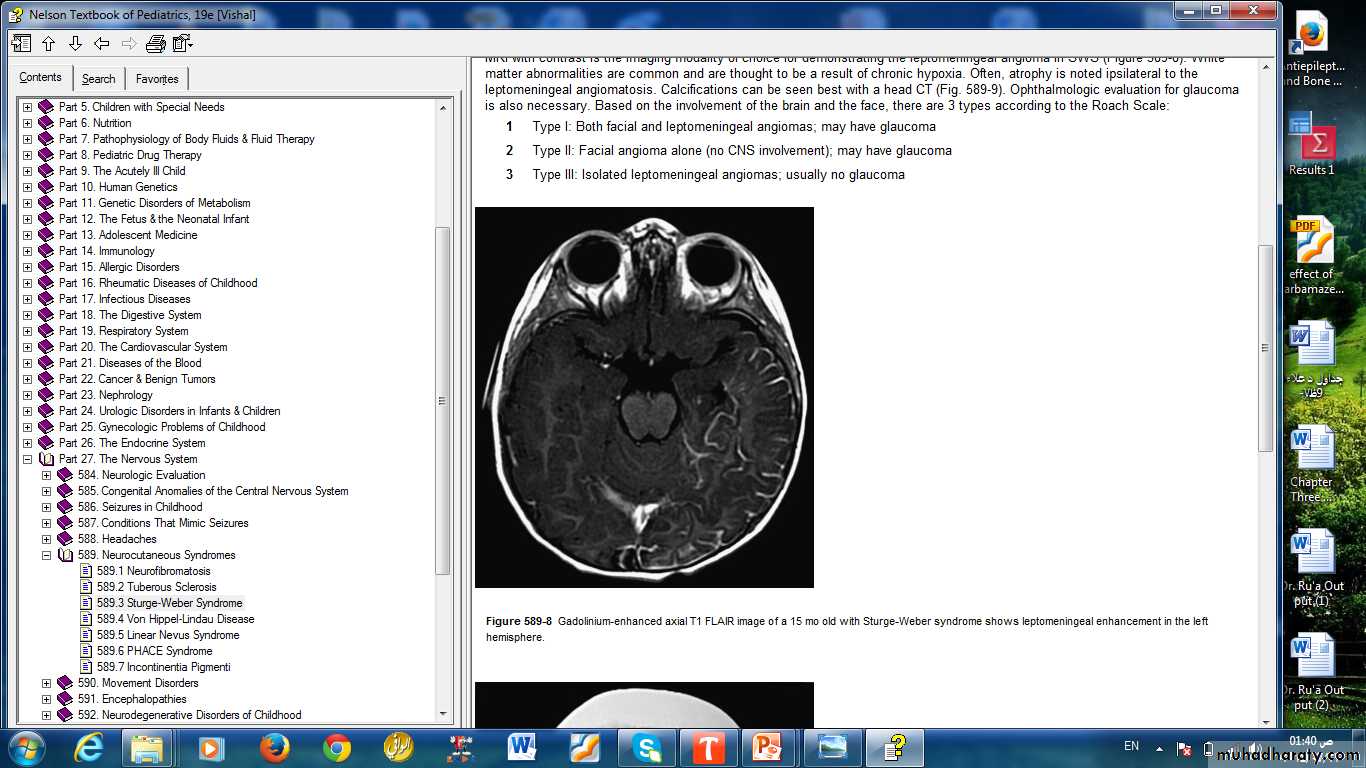
MRI
• X-Ray
• 3- MRI is a useful to detect the location of the vascular malformation and the presence of white matter lesions.
• Treatment
• 1. Seizure control: by anticonvulsants. If the seizures are refractory to anticonvulsant therapy, especially in infancy and the 1st 1–2 yr, and arise from primarily one hemisphere, most centers advise surgery (hemispherectomy).
• 2.The facial nevus treated by Laser therapy (it may cause psychologic trauma).
• 3. Because of the risk of glaucoma, regular measurements of intraocular pressure with is indicated.
1.A 7-mo-old girl is presented to the emergency department with gradual onset of fever, lethargy, and irritability. Her immunizations are up to date. Examination reveals a febrile infant who does not interact with the examiner and cries inconsolably. A lumbar puncture is performed, and the cerebrospinal fluid contains
1,500 white blood cells/mm3, 84% of which are granulocytes;
glucose concentration of 12 mg/dL;
a protein concentration of 100 mg/dL.
RBS 100 mg /dL
a. What is the dignosis ?
B What is imperical treatment can give?
2. A 19-yr-old girl presents with headache, unsteadiness, and poor hearing that has worsened over the past 5 yr. Her father's medical history includes some type of brain surgery, and he has been deaf since the age of 35 yr. The most likely diagnosis is:
• Neurofibromatosis type 2
• Optic glioma
• Neurofibromatosis type 1
• Tuberous sclerosis
• Late-onset congenital deafness
• 3.The most common cause of viral meningoencephalitis is:
• An enterovirus• Herpes simplex virus
• An arbovirus
• Mumps virus
• A respiratory virus
2.Neurofibromatosis type 1, an autosomal dominant disorder (gene on chromosome 17), is defined by six or more café-au-lait macules greater than 5 mm in diameter in prepubertal children or greater than 15 mm in postpubertal children plus at least one of the following except:
• Axillary or inguinal freckling
• Lisch nodules of the iris
• Two or more neurofibromas or one plexiform neurofibroma
• Ash leaf macule
• Osseous lesions (sphenoid dysplasia, scoliosis)
• Optic gliomas
• An affected first-degree relative
