د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
1
Oral Cavity Diseases
RANULA
(Rana = Frog, Ranula looks like belly of frog, hence the name—Latin).
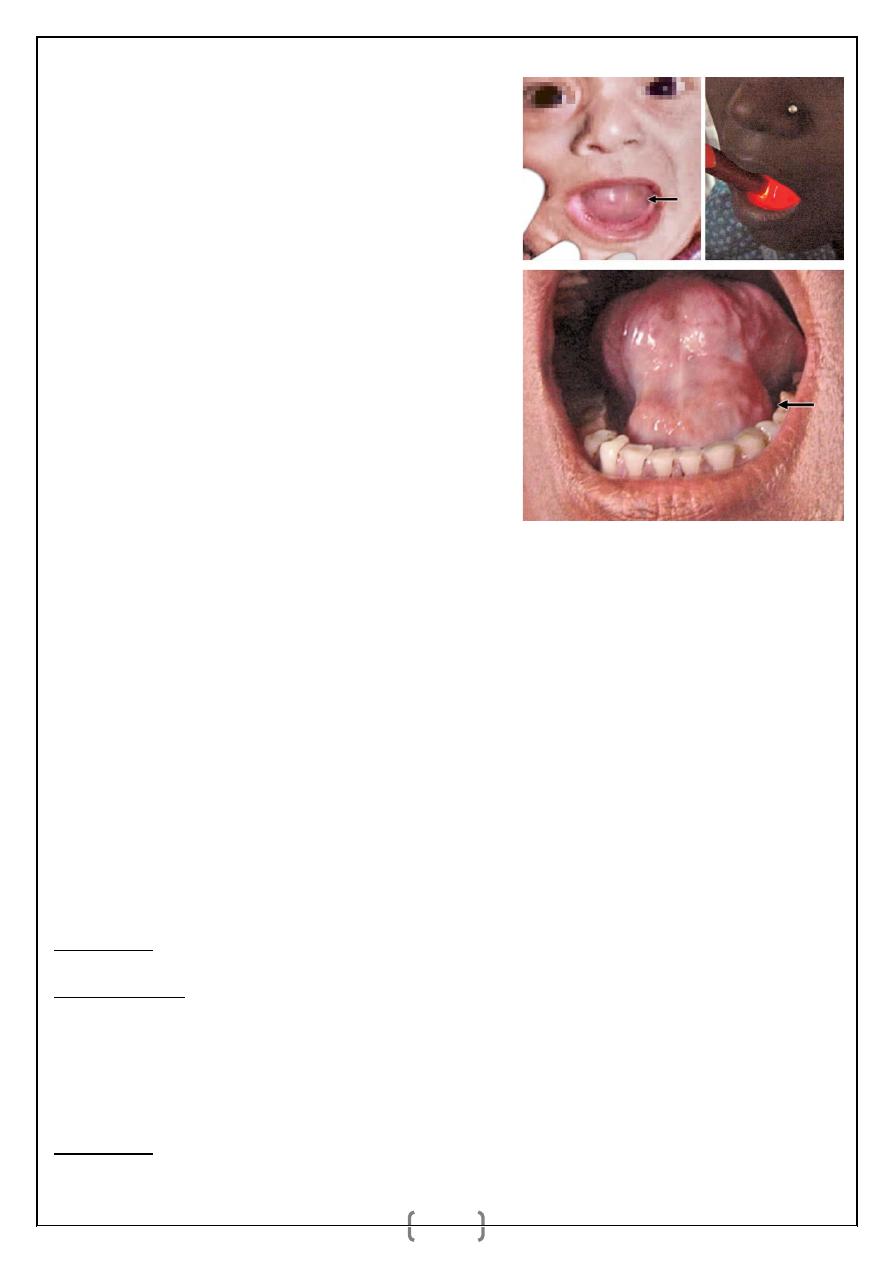
_ Ranula is an extravasation cyst arising from sublingual gland or mucous
glands of Nuhn or glands of Blandin in the floor of the mouth. Occasionally it
can occur in submandibular salivary gland also.
_ initially there is blockage of the duct (of sublingual gland) causing retention
cyst, which causes rupture of the acini due to increased pressure leading into
extravasation cyst.
plunging ranula:
It is intraoral ranula with cervical extension, It often extends
into the submandibular region through the deeper part of the posterior margin of
mylohyoid muscle as soft,
fl uctuant, nontender, dumbbell shaped swelling in the
submandibular region. It is bidigitally palpable. US and/or MRI is diagnostic. It
is treated by surgical excision through neck approach along with excision of
submandibular and sublingual salivary glands. Small plunging ranula is often
excised per orally along with excision of sublingual salivary gland.
Complications:
It may damage the Wharton’s duct.
It may rupture.
it may get infected.
It may interfere with speech and swallowing occasionally.
Differential Diagnosis
Lymph cyst.
Sublingual dermoid.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
2
Treatment
_
Marsupialisation can be done initially and
later once the wall of the ranula is thickened it
is excised (Marsupial means pouch where
baby is kept, carried and sucked on the
mother’s belly, like in Kangaroo).
_
If ranula is small it can be excised without
marsupialisation.
_
Excision of sublingual salivary gland is often
needed. In plunging ranula submandibular
salivary
gland
needs
to
be
excised.
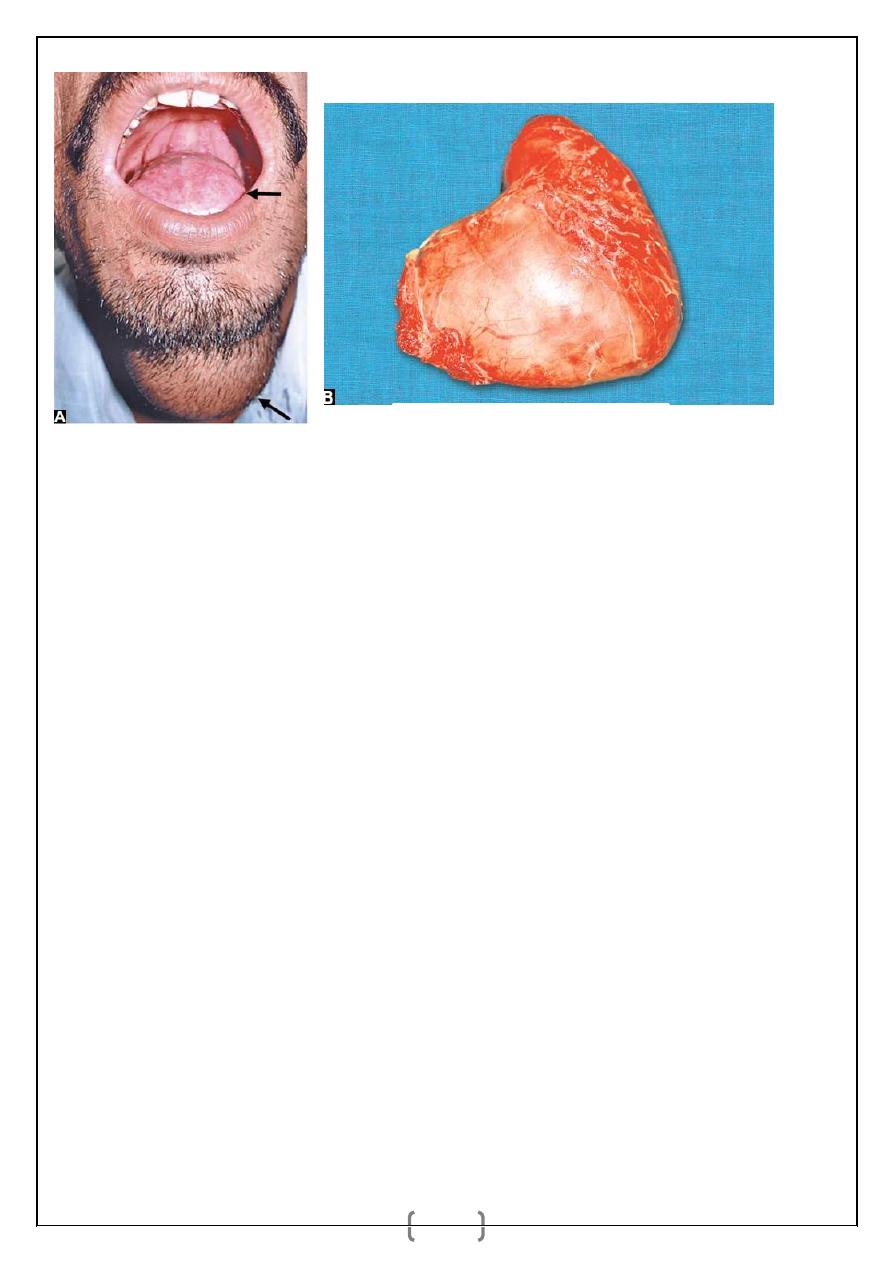
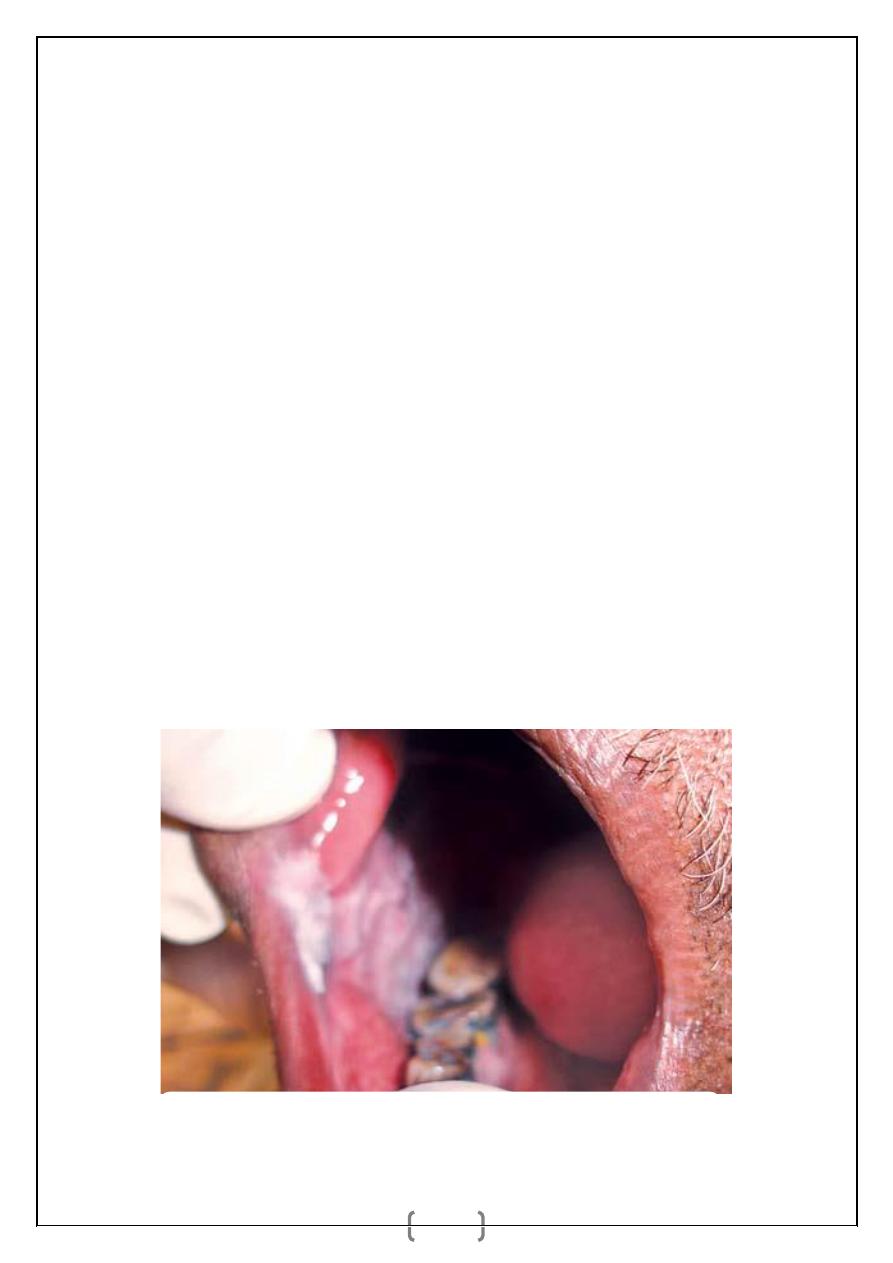
SUBLINGUAL DERMOIDS
They are sequestration dermoids lined by squamous epithelium containing
keratin. It is smooth, soft, fluctuant, nontransilluminant bidigitally palpable
swelling.
Types
1. Median sublingual dermoid: It is derived from epithelial cell rests at the level
of fusion of two mandibular arches. It may be supramylohyoid or
inframylohyoid. It is located between two genial muscles, in relation to
mylohyoid muscle. It is a midline swelling which is smooth, soft, cystic,
nontender, nontransilluminant.
Treatment is excision through oral approach.
Complication is abscess formation.
2. Lateral sublingual dermoid: It develops in relation to submandibular duct,
lingual nerve and stylohyoid ligament. It is derived from first branchial arch. It
forms a swelling in the lateral aspect of the floor of the mouth.
Treatment: Small one is removed per orally. Larger one, through submandibular
incision.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
3
STOMATITIS
_ It is inflammation of oral mucosa by trauma, radiotherapy, chemicals,
nutritional deficiency or infection.
1. Traumatic stomatitis may be due to dentures, teeth bite, and brushing of teeth
harshly which presents as painful thin covering of furr with increased salivation.
Proper mouth wash will cure the condition.
2. Aphthous stomatitis is seen in malnutrition, debility, steroid usage. Present as
multiple hyperaemic painful vesicles later forming deep round painful ulcers. It
is treated with mouth wash and if needed by antibiotics. Recurrent aphthous
stomatitis with ulcers is often familial, more common in women, common in lip,
cheek, tongue which are very painful with more salivation. It heals
spontaneously. But during active period, it interferes with speech, swallowing
distressfully. It is treated by many drugs like levamisole, antibiotics, vitamin B
and
C,
local
applications
of
anaesthetics
(xylocaine)/choline
salicylate/benzalkonium chloride.
3. Candida stomatitis (Monilial thrush) is due to fungal infection, Candida
albicans which is seen in diabetics, individuals on steroid therapy, long-term
antibiotics, patients who are bedridden, on prolonged ICU care, in infants, and
debilitated patients. Initially multiple red spots which are painful appear in the
tongue and buccal area which later turn into curdy white patches. Often it
A and B: Sublingual dermoid.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
4
extends into pharynx and esophagus causing dysphagia. It is treated with
antifungal drugs like clotrimazole or fluconazole.
4. Vincent’s ulcerative stomatitis (Vincent’s angina/trench mouth) is due to
infection by Gram –ve anaerobic bacteria Borrelia vincentii and Fusiformis
fusiformis. It is common in adolescents and young adults below the age of 35
years. Presents with fever, excessive salivation, red swollen gums with painful
ulcers covered with yellow slough (pseudomembrane) which can be removed
like membrane – ulcerative gingivitis. From the gums it spreads to cheek, palate,
and pharynx. Tongue involvement is uncommon. Tender neck lymph nodes are
palpable. Musty foetor oris is typical. Edentulous patients will not develop this
infection. Infection in tonsillar crypts is called as Vincent’s angina. It is
confirmed by swab culture. It is treated by antibiotics (penicillin group); peeling
of membrane, mouth wash, supportive measures, vitamin B and C.
5. Nutritional stomatitis is due to—(1) vitamin B deficiency like nicotinic acid
(pellagra), riboflavin deficiency. It is common in tongue presenting as red area
with atrophy of papillae. (2) Vitamin C deficiency is commonly seen as bleeding
gums and loosening of teeth. (3) Iron deficiency anaemia causes superficial
glossitis mainly in females.
6. Angular stomatitis is superficial lengthy red brown fissures/ ulcers in and
around the angle of the mouth with cracks. Candida and streptococci infections
are common. It is often called as cheilosis/perleche. It is treated with vitamin B,
C, iron and protein supplements with adequate oral hygiene. Perleche is seen in
children who suck their finger.
SYPHILITIC LESIONS OF ORAL CAVITY
Chancre in lip: It is highly contagious primary chancre, presents as painless
macule later forming painful superficial ulcer. Ulcer eventually heals with a scar.
It can be on both upper and lower lip—primary syphilis. Mucous patches which
are greyish white contagious patches seen on lip, cheek and fauces. Mucous
patches fuse together to form linear snail track ulcers in fauces, pillars—
secondary syphilis. Hutchinson’s contagious condyloma in midline tongue can
occur. Gummatous painless ulcer is seen in anterior 2/3rd of tongue, palate and
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
5
nasal septum (causes perforation and collapse of nasal bridge). Syphilitic chronic
glossitis is seen in tertiary syphilis which is a precancerous condition.
ORAL SUBMUCOSAL FIBROSIS
_ It is a progressive fibrosis deep to the mucosa of the oral cavity which causes
trismus and ankyloglossia.
_ The mucosa of cheek, gingivae, palate and tongue shows a mottled/marbled
pallor.
_ It is common among Asians and Indians.
_ Aetiology: Hypersensitivity to chilli, betelnut, tobacco and vitamin deficiencies
probably alter the collagen metabolism leading to juxtaepithelial fibrosis,
epithelial atrophy and dysplasia.
_ 4.5-7.6% of oral submucosal fi brosis turns into malignancy (Paymaster—1956
study shows 30-33% incidence—very high).
_ Treatment: Precipitating factors has to be avoided.
_ Surgical excision when required, followed by skin grafting, has to be done.
Submucosal fibrosis of right cheek. Note the stiff fibrotic bands and scarring.
bands and scarring.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
6
PREMALIGNANT CONDITIONS OF ORAL CAVITY
High risks—lesions with definite risk of malignant change
_ Leukoplakia.
_ Erythroplakia.
_ Chronic hyperplastic candidiasis: It is common in commissures of the mouth
and tongue. Dense plaque of leukoplakia is common with curdy white patches
due to Candida albicans infection. It often may not respond to drugs, surgery or
laser. Immunodeficiency is often associated with this. It is treated by topical or
systemic antifungal drugs/surgical excision or laser therapy.
Medium risks—premalignant but not associated with higher incidence of
carcinoma:
_ Oral submucosal fibrosis.
_ Syphilitic glossitis.
_ Sideropenic dysphagia (Sideropenia is iron deficiency without anaemia); or
Plummer-Vinson syndrome. Sideropenia is common in Scandinavian females. It
causes atrophy of epithelium and becomes potentially malignant. Proper iron
therapy controls the disease and reduces the risk.
DON’T FORGET
"We are weaving the future on the loom of today"