د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
1
TONGUE
Anatomy of Tongue
Tongue is a muscular organ located in the floor of the mouth.
Parts
:
1. Tip: Anterior free end lies behind the upper incisor teeth.
2. Root: Attached to the mandible above and hyoid bone below.
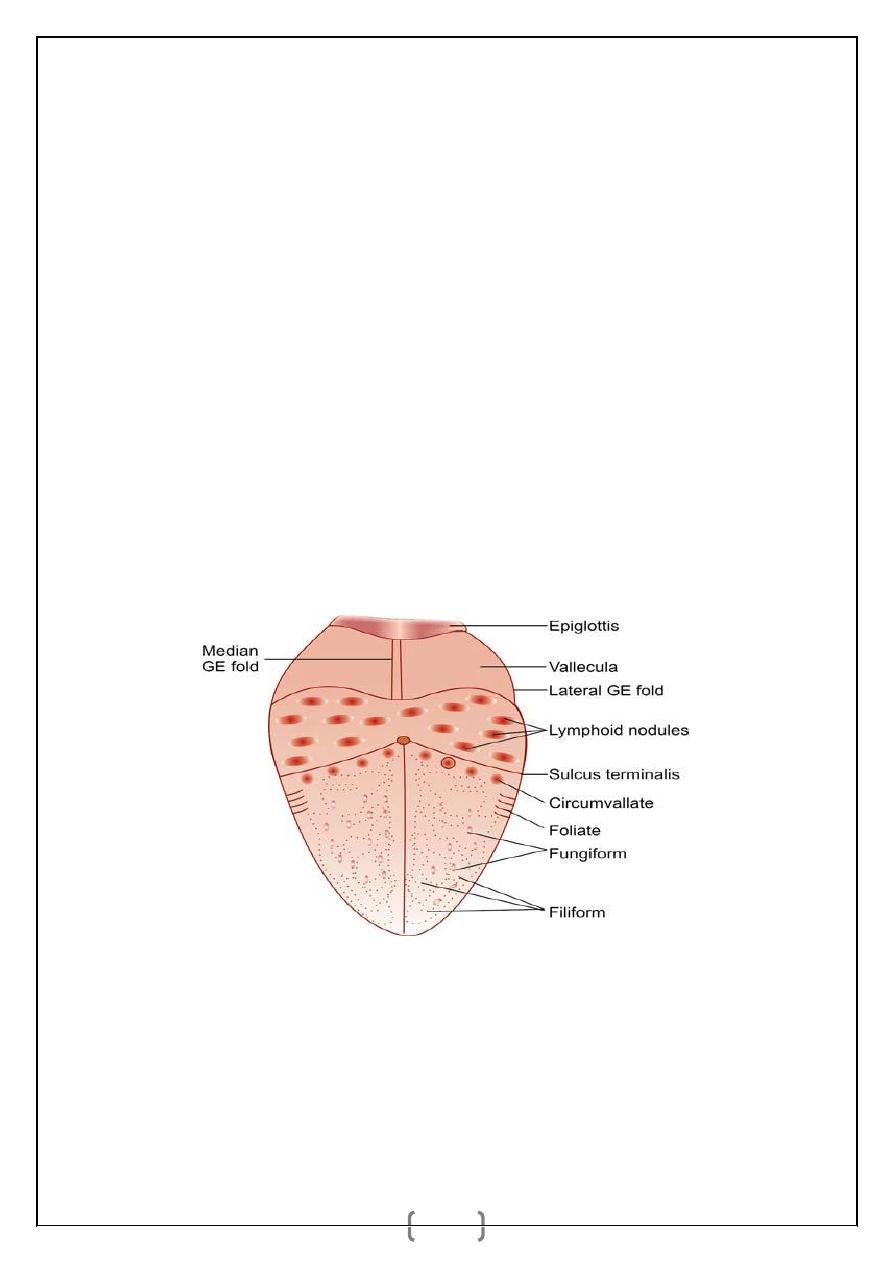
3. Body: Dorsal surface is rough due to papillae; and is divided into anterior 2/3rd (oral part)
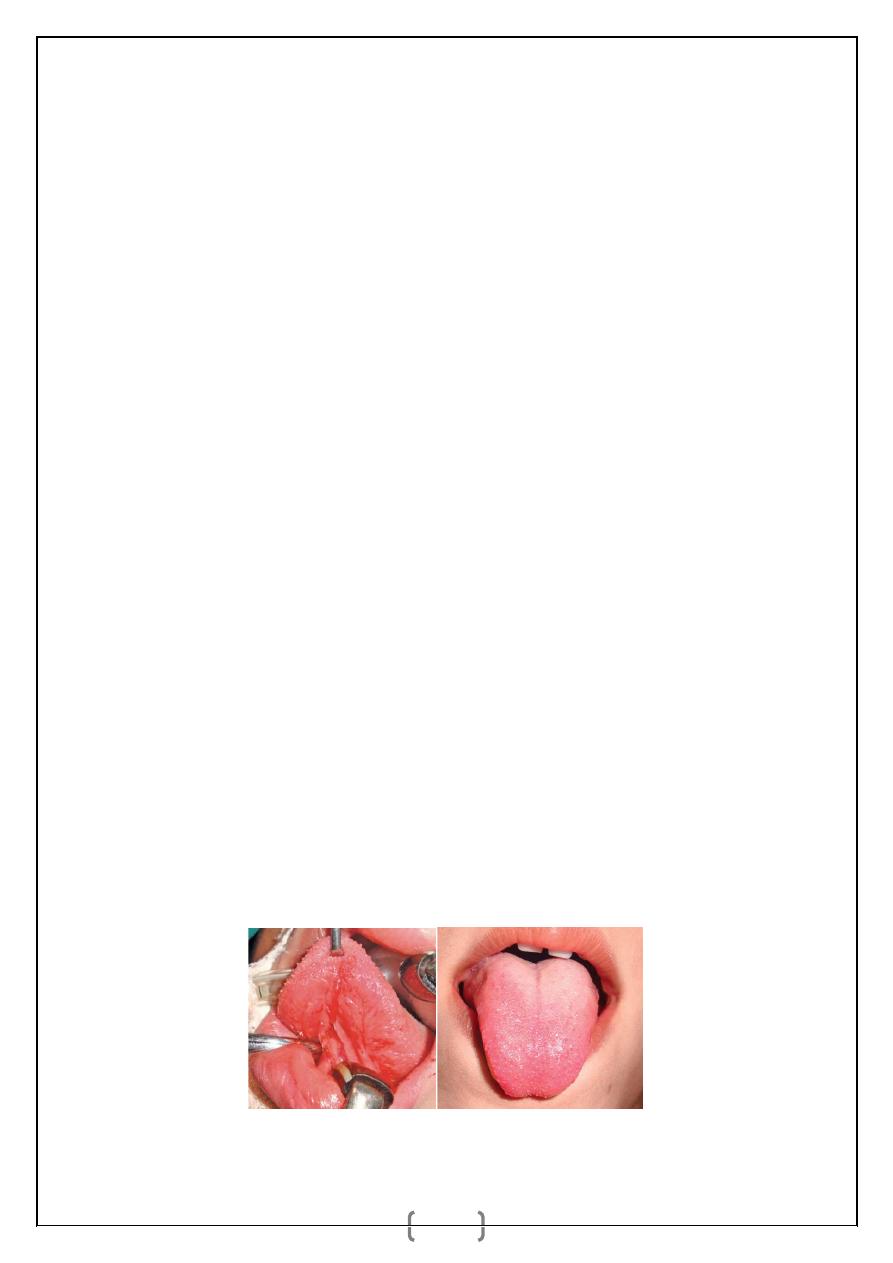
and posterior 1/3rd (pharyngeal part) by sulcus terminalis. Ventral surface is smooth, has a
median fold, ‘frenulum linguae’ and deep lingual vein on either side.
Papillae
:
1. Vallate—large, located in front of sulcus terminalis.
2. Fungiform—lies over the tip and margin of the tongue.
3. Filiform—lies over the dorsum of tongue, gives the velvety appearance—commonest.
4. Foliate—over the margin.
Muscles of Tongue
:
a. Intrinsic muscle: Superior and inferior longitudinal, transverse and vertical.
b. Extrinsic muscle: Genioglossus, hyoglossus, styloglossus, palatoglossus. Blood supply is
from lingual artery, a branch of external carotid artery. Venous drainage by deep lingual vein
which drains into fascial vein or internal jugular vein.
د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
2
Lymphatic Drainage of the Tongue
:
_ Tip of tongue drains into submental lymph nodes.
_ Lateral margin drains to submandibular lymph nodes and into upper deep cervical lymph
nodes. Many lymphatic vessels pass as subperiosteal lymphatics of mandible. So carcinoma
can involve the bone through this route.
_ Lymphatics in the midline of tongue freely cross communicate with each other and so
spread of malignancy can occur to both side neck lymph nodes.
_ Lymphatics from posterior third of tongue drain into pharyngeal group of lymph nodes, as
well as to the upper deep cervical lymph nodes. Early spread to the pharyngeal lymph nodes
from carcinoma of posterior third of tongue has a poor prognosis.
Lymphatic vessels are named as:
1. Apical vessels.
2. Central vessels.
3. Marginal vessels.
4. Basal vessels.
Development and Nerve Supply of the Tongue
:
_ Anterior 2/3rd develop from first branchial arch through two lingual swellings and one
tuberculum impar. It is supplied by lingual nerve for general sensation and by chorda
tympani for taste sensation.
_ Posterior 1/3rd develops from third arch from cranial half of hypobranchial eminence. It is
supplied by glossopharyngeal nerve for both general and taste sensations.
_ Posterior most part develops from the fourth arch. It is supplied by vagus nerve (internal
laryngeal nerve).
_ Muscles of the tongue are derived from occipital myotomes and are supplied by
hypoglossal nerve except palatoglossus, which is supplied by cranial part of accessory nerve.
د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
3
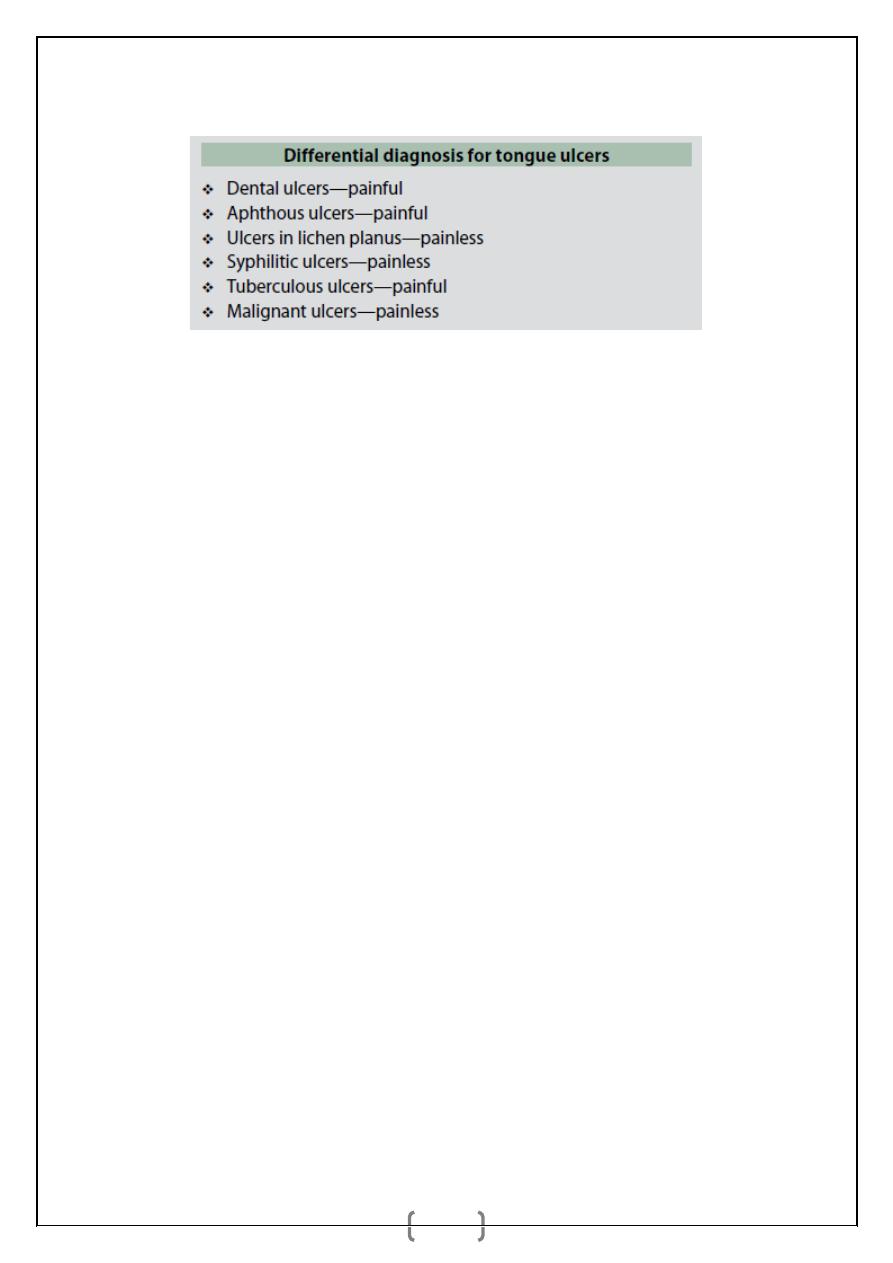
TONGUE ULCERS
:
Dental Ulcer
It is common on sides of tongue due to sharp tooth, denture, and broken tooth. Usually it is
acute painful, self-limiting ulcer. Occasionally repeated trauma form an indolent chronic
ulcer which mimic carcinoma; it should be excised to rule out carcinoma and to cure the
ulcer.
Aphthous Ulcer
It can be :
(1) Minor aphthous ulcer, common in menstruating women as a crop with painful, round,
yellow based ulcer with red margin. It regresses spontaneously in 2 weeks.
(2) Major aphthous ulcer, large and deep which often becomes chronic and takes more time
to subside with a scar. Chlorhexidine gluconate, local application of triamcinolone acetate,
choline salicylate gel are different local applicants used to promote healing.
(3) Behcet’s syndrome is genital ulcer, conjunctival ulcer and multiple oral ulcers. Reiter’s
syndrome is urethritis, arthritis, periarteritis nodosa, conjunctivitis, and oral ulcers.
(4) Herpetiform aphthous ulcer is not due to herpes simplex. They are small, 1-2 mm
diameter ulcers in crops which heal by usual drugs mentioned above.
Syphilitic Ulcer
Extragenital chancre often occurs in tongue in primary syphilis which is painless with shotty,
submental and submandibular lymph nodes. In secondary syphilis, multiple shallow snail
track ulcers in the margins and undersurface; mucous patches on the tongue and fauces;
Hutchinson’s condyloma wart in midline of tongue can occur. In tertiary syphilis,
gummatous ulcer occurs in anterior 2/3rd of tongue as a deep punched out painless ulcer as
gumma with wash leather slough. Endarteritis is the cause for the punched out look.
Interstitial glossitis with loss of papillae causes longitudinally fi ssured bald lobulated
tongue in tertiary syphilis. In carcinoma arising from syphilitic ulcer, RT is questionable as
د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
4
Blood supply is precarious due to endarteritis; RT further compromises it leading to tongue
necrosis.
Tuberculous Ulcer
It is undermined shallow, often multiple, painful ulcer. Ulcer can occur in margins, tip or
anterior 2/3rd of tongue. Neck nodes may be involved. Associated tuberculous larynx and
lung may be present.
Herpetic Lingual Ulcer
It is involvement of lingual nerve presenting as acute neuralgia with vesicles which form
multiple superficial painful ulcers.
Other Ulcers
Multiple ulcers in smokers due to glossitis (smoker’s ulcer), ulcers due to vasculitis,
eosinophilic granuloma. Post-pertussis ulcer in whooping cough occurs on upper part of
frenum linguae and under the tip of tongue.
TONGUE FISSURE
:
Congenital fissures are transverse which run laterally from midline with normal papillae in
between. Candida infection can occur on this. Syphilitic fissures are deep bald and
longitudinal.
TONGUE TIE
:
It is short, thick, fibrous frenum linguae. During protrusion lateral margin and tip of the
tongue is everted with dorsal mid part heaping. It causes speech defect, difficulty in cleaning
the inner part of lower teeth.
د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
5
GLOSSITIS
:
Median Rhomboid Glossitis
It is smooth, lobulated, triangular firm patch anterior to foramen caecum of tongue in midline
with deeper colour. Candida infection can occur in it.
It mimics carcinoma. Biopsy rules out
malignancy. Carcinoma is uncommon in midline.
Glossitis Migrans (Geographic Tongue)
It begins as benign small red patches with white furred margin which spread and recede in an
irregular way to appear as fresh patches. White margin contains keratinized epithelium and
inflamatory cells over filiform papillae. It is often seen in patients with congenital heart
diseases and acute gastrointestinal diseases. Etiology is unknown.
Other Glossitis
Hunter’s glossitis is seen in pernicious anaemia.
Hairy tongue is overgrowth of filiform papillae with black/ brown stain on it due to
bacteria, fungi, tobacco or drugs. There are no hairs. It is a misnomer. Cessation of
causative agent, mechanical scraping, cleaning are the treatment methods.
Agranulocytosis glossitis.
Nonspecific glossitis.
Pellagra glossitis, due to deficiency of nicotinamide (B3).
Chronic superficial glossitis in malnutrition, iron and vitamin B deficiencies.
LEUKOPLAKIA
It is a white patch in the mucosa of the oral cavity that cannot be characterized clinically or
pathologically to any other disease. It is a premalignant condition.
Types
1. Homogenous.
2. Nodular—more potentially malignant.
3. Speckled—more potentially malignant–highest.
Clinically
the lesion appears as white or greyish coloured, well-localised patch in the cheek,
tongue, palate or other areas of the oral cavity.
Incidence
of leukoplakia in those who smoke or chew pan is 20%, whereas incidence in
non-smokers is 1%. Incidence of its turning into malignancy is 2-4%. It increases with age,
duration of the pan chewing, smoking.
د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
6
Diagnosis
: Biopsy confirms the diagnosis as well as rules out the carcinoma.
Treatment
:
Pan chewing and smoking has to be stopped.
Excision, if required skin grafting has to be done.
Regular follow-up is necessary.
Isoretinoin is helpful. Beta-carotene, tocoferol are also used.
CO2 laser excision.
ERYTHROPLAKIA
It is red velvety appearance of the mucosa which cannot characterize any recognized
condition. It is 17-20 times more potentially malignant than leukoplakia. Histologically
parakeratosis with severe epithelial dysplasia is the typical feature. Red color is due to
decreased keratin causing shining and prominence of submucosal red vascularised
connective tissue.
_ It is equal in both sexes.
_ It is common in lower alveolar mucosa, gingivobuccal sulcus and floor of the mouth.
_ It can be homogenous/speckled/granular or erythroplakia interspersed with leukoplakia.
_ Diagnosis is done by biopsy.
_ Treatment: Biopsy and surgical excision.
CARCINOMA OF THE TONGUE
Incidence is equal in both sexes. Presently its incidence is increasing in females due to
increase in number of female smokers.
د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
7
Aetiology
Leukoplakia.
Erythroplakia.
All ‘S’s (as mentioned in leukoplakia).
Premalignant conditions mentioned earlier.
Types
Gross
1. Papillary.
2. Ulcerative or ulceroproliferative 60%.
3. Fissure with induration.
4. Lobulated indurated mass—frozen tongue.
Histologically
:
1. Squamous cell carcinoma—commonest.
2. Adenocarcinoma may arise from minor salivary glands or mucous glands.
3. Melanomas.
4. Transitional cell carcinoma and lymphoepithelioma rarely can occur in posterior 1/3rd of
tongue.
Sites
:
1. Lateral margin—commonest—47-50%.
2. Posterior third—20%.
3. Dorsum—6.5%.
4. Ventral surface—9%.
5. Tip—10%.
Clinical Features
:
Painless ulcer/swelling in the tongue which later may become painful. Pain in the
tongue due to infection or
ulceration or due to the involvement of lingual nerve (pain
is referred to ear). Pain on swallowing, in case of carcinoma of posterior third of
tongue.
Excessive salivation. Saliva is often blood stained.
Dysphagia either due to fixed tongue or due to the involvement of genioglossus or
growth in the posterior third of the tongue.
Visible ulcer in anterior two-thirds of tongue. Ulcer can bleed on touch; edge, base and
surrounding areas are indurated. Often indurated area is much more extensive than the
د.أشرف مزاحم الشاكر
كلية طب نينوى
tongue
8
primary tumour (it is also common in carcinoma penis). Edge is everted commonly.
Ulcer
may
cross
the
midline;
may
extend
into
the
floor
of
the
mouth/alveolus/mandible. Growth or ulcer in posterior third is usually not visible.
Ankyloglossia—involvement of muscles of the tongue. Movements of the tongue
especially forward protrusion are commonly affected.
Inability to articulate.
Foetor (Halitosis). Due to infection and necrosis in the oral cavity. It is due to release
of ammonia, butyric acid and mercaptan by tumour cells.
Change in voice. Occurs in posterior third tumours. Tumour in posterior third area is
more aggressive.
Palpable lymph nodes in the neck which are hard, nodular and get fixed to underlying
tissues in advanced stages.
Features of bronchopneumonia—due to aspiration during lying down/sleeping mainly
to lower segment of lung.
Spread of Carcinoma Tongue
Local spread
:
In case of anterior two-thirds of tongue, the spread occurs to genioglossus muscle, floor of
the mouth, opposite side and mandible. In case of posterior third of tongue it spreads locally
to tonsil, side of pharynx, soft palate, epiglottis, larynx and cervical spine.
Lymphatic spread
:
From tip of tongue it spreads to submental nodes. From lateral margin it spreads to
submandibular lymph nodes and later to deep cervical lymph nodes. Lymphatics in the
tongue are freely communicating, and so involvement of bilateral neck lymph nodes is
common. From posterior third it spreads to pharyngeal nodes and upper deep cervical lymph
nodes.
Investigations
1. Edge biopsy.
2. FNAC of lymph nodes.
3. Indirect and direct laryngoscopy to see posterior third growth.
4. CT scan to see the extension of posterior third growth or to see the status of advanced
secondaries. MRI is also very useful to assess the extent of primary tumour.
5. Chest X-ray to see bronchopneumonia.
6. Orthopantomogram.
Treatment
Surgery, radiotherapy, chemotherapy.