Delayed puberty
Normal puberty:Puberty is the process of reproductive and sexual development and maturation which changes a child into adult. During childhood, the HPO axis is suppressed and levels of GnRH, FSH and LH are very low. However, from the age of 8 to 9 years in girls and 2 years later in boys, GnRH is secreted in pulsations of increasing amplitude and frequency. These are initially sleep-related, but as puberty progresses, these extend throughout the day. This stimulates secretion of FSH and LH by the pituitary gland which in turn triggers follicular growth and steroidogenesis in the ovary. The oestrogen produced by the ovary then initiates the physical changes of puberty. The exact mechanism determining the onset of puberty is still unknown, but it is influenced by many factors including race, heredity, body weight and exercise. Leptin, growth hormone and thyroid hormone play a role in the onset of puberty.
The physical changes occurring in puberty are:
-breast development (thelarche)
-pubic and axillary hair growth (adrenarche)
-growth spurt
-onset of menstruation (menarche)
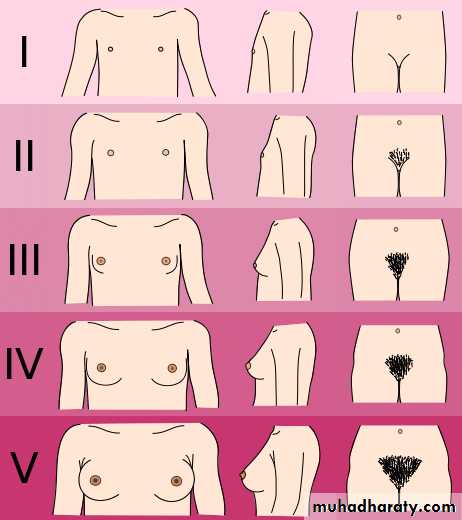
The first physical signs of puberty are breast budding and this is usually as an indicators of development and is often unequal between the 2 breast, thelarche occurs 2 or 3 years before menarche. The appearance of pubic hair is dependent on secretion of adrenal androgens and is usually after thelarche. The mean age of menarche is 12.8 years and it may take over 3 years before the m.c establishes a regular pattern. Initial cycles are usually anovulatory and can be unpredictable and irregular. Pubertal development was described by Tanner and the stages of breast and pubic hair development are having 5 stages, but the axillary hair only have 3 stages.
Delayed puberty:
This occurs when there are no signs of secondary sexual characteristics by the age of 14 years. Delay in puberty occurs in only 2.5% of the population. It is mandatory to take a detailed history as the presence of chronic medical conditions or excessive athletic, may be an obvious explanation for delay in the onset of puberty. In female, about 50% will have constitutional delay that is could be genetically based. It is due to either a central defect- hypogonadotrophic hypogonadism or to a failure of gonadal function- hypergonadotrophic hypogonadism.Hypogonadotrophic hypogonadism:
The majority of girls with low gonadotrophins have constitutional delay in puberty. This may be secondary to chronic illness such as diabetes or renal failure. Girls with anorexia nervosa have low levels of gonadotrophins also athletic girls have similar situation. Improvement in the underlying cause usually results in catch-up growth.
Congenital deficiency of gonadotrophins is more rarely seen, this problem often found in boys it may be also associated with anosmia, it is known as Kallman's syndrome (X-linked recessive), and usually treated by give the patient GnRH.
Acquired deficiency may follow damage to the hypothalamus or pituitary as a result of trauma, tumour such craniopharyngioma, irradiation or infection- secondary to hydrocephalus. Infiltration of these organs can also occur in haemochromatosis, which may be secondary to transfusions for sickle cell disease or thalassaemia, and treated by give the patient GnRH or the deficient gonadotrophins.
Hypergonadotrophic hypogonadism:
In this situation, the gonad does not function despite a high FSH. The most common cause is Turner syndrome (45X) and XX gonadal dysgenesis will also cause this. Premature ovarian failure can occur at any age and may be idiopathic, but can be also be of an autoimmune disorder or following chemo-or radiotherapy for childhood cancer. Other causes include damage to the ovaries by surgery or infection, and this usually treated by gonadotrophins.
Precocious puberty:
This is defined as the onset of puberty before the age of 8 in a girl or 9 in a boy. It is classified as either central or peripheral.
Central p.p. this refers to early onset of puberty due to early activation of the HPO axis, so it is gonadotrophins dependent. A positive family history of early onset puberty may be discovered but in the majority of cases the etiology is idiopathic. The etiology is often unknown, although up to 25% are due to CNS malformation or brain tumour. The majority of girls with central p.p. not required hormonal treatment, because most development is extremely slow and will result in maturity at an age which would be expected even though onset has been early.
Peripheral p.p this is far less common than central p.p. and is always pathological and can be caused by excess production of sex steroids, such as exogenous ingestion e.g. inadvertent ingestion of birth control pills by children, or a hormone- producing tumour like ovarian or adrenal tumour. Treatment of peripheral p.p. according to the cause if exogenous source usually treated by stop it, and if endogenous treated by surgical removal of ovarian or adrenal.