Approach to the adult patient with anemia
Dr. Khalid N M AL-KHEROFRCP(LONDON),CABMS.DM.ASH,EHA
Consultant hematologist/Physician
• DEFINITIONS
Anemia defined as a reduction in one or more of the major red blood cell (RBC) measurements obtained as a part of the complete blood count (CBC): hemoglobin concentration, hematocrit (HCT), or RBC count. In practice, however, a low hemoglobin concentration or a low hematocrit is most widely employed for this purpose.Hemoglobin the major oxygen-carrying molecule in whole blood. Values may be expressed as grams of hemoglobin per 100 mL of whole blood (g/dL) or per liter of blood (g/L).
Hematocrit – (HCT), also called packed cell volume(PCV), is the packed spun volume of blood that consists of intact RBCs, expressed as a percentage. HCT can be measured directly following centrifugation of a blood sample or calculated (HCT = [RBC x MCV]/10).
RBC count – RBC count is the number of RBCs contained in a specified volume of whole blood, usually expressed as millions of cells per microL of whole blood.
Normal ranges for hemoglobin/HCT
a hemoglobin <13.5 g/dL (<135 g/L) or a HCT <41.0 percent represents anemia in men, and a value <12.0 g/dL (<120 g/L) or <36.0 percent, respectively, represents anemia in women.Red blood cell indices — The RBC indices describe the size, shape, and hemoglobin content of RBCs, as well as the uniformity of the RBC population.
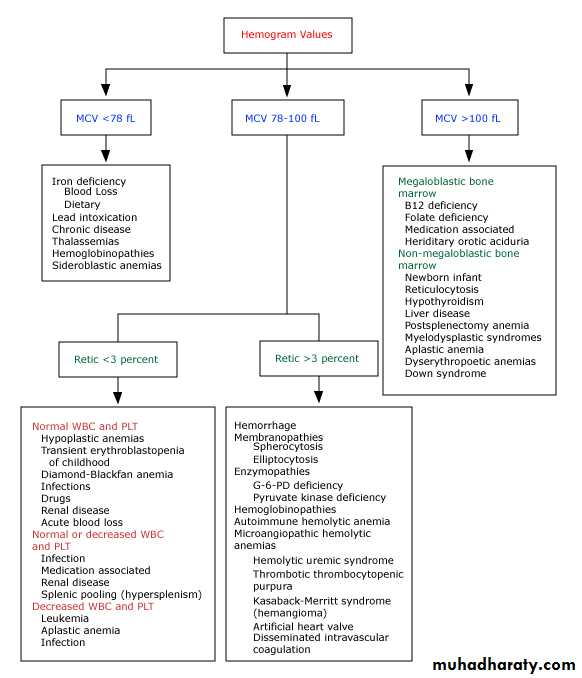
MCV – Mean corpuscular volume (MCV) is the average volume (size) of the patient's RBCs. It can be measured or calculated (MCV in femtoliters [fL] = 10 x HCT[in percent]÷RBC[in millions/microL]).
Anemia can be classified based on whether the MCV is low, normal, or elevated
MCH – Mean corpuscular hemoglobin (MCH) is the average hemoglobin content in a RBC. It is calculated (MCH in picograms [pg]/cell = hemoglobin [in g/dL] x 10 ÷ RBC [in millions/microL]. A low MCH indicates decreased hemoglobin content per cell, and is typically reflected in hypochromia on the peripheral blood smear
Red blood cell indices;continue
MCHC – Mean corpuscular hemoglobin concentration (MCHC) is the average hemoglobin concentration per RBC. It is calculated as (MCHC in grams [g]/dL = hemoglobin [in g/dL] X 100 ÷ HCT [in percent]).
Red cell distribution width (RDW) is a measure of the variation in RBC size, which is reflected in the degree of anisocytosis on the peripheral blood smear. A high RDW implies a large variation in RBC sizes, and a low RDW implies a more homogeneous population of RBCs. RDW is calculated as the coefficient of variation (CV) of the red cell volume distribution (RDW = [standard deviation/MCV] x 100)
Reticulocytes can be enumerated manually after supravital staining of a blood sample with dyes such as new methylene blueThe normal range (ie, percent of RBC with positive staining) in adults is 0.5 to 2.0 percent Reticulocytes can be appreciated on a standard blood smear stained with Wright-Giemsa as RBC with a blue tint (polychromatophilia) that are larger than mature RBC, with irregular borders and a lack of central pallor
CLINICAL CONSEQUENCES
with each gram of hemoglobin capable of carrying 1.3 mL of oxygen. Thus, approximately 20mL/dL (or 20 volumes percent) can be carried by 15 g/dL of hemoglobin at full saturation.Symptoms — Symptoms related to anemia can result from two factors:
1-decreased oxygen delivery to tissues and,
2-in patients with acute and marked bleeding, the added insult of hypovolemia.
oxygen delivery can be maintained at rest at a hemoglobin concentration as low as 5 g/dL
CLINICAL CONSEQUENCES -continue
Symptoms will occur when the hemoglobin concentration falls below this level at rest, at higher hemoglobin concentrations during exertion, or when cardiac compensation is impaired because of underlying heart diseaseExertional dyspnea, dyspnea at rest ,Fatigue
S/S of the hyperdynamic state such as bounding pulses, palpitations, and a roaring pulsatile sound in the ears.More severe anemia may lead to lethargy, confusion, and potentially life-threatening complications such as congestive failure, angina, arrhythmia, and/or myocardial infarction
EVALUATION OF THE PATIENT
‘Anemia is one of the major signs of disease. It is never normal and its cause(s) should always be sough’
The workup should be directed towards answering the following questions concerning whether one or more of the major processes leading to anemia may be operative:
●Is the patient bleeding (now or in the past)?
●Is there evidence for increased red blood cell (RBC) destruction (either intravascular or extravascular)?
●Is the bone marrow suppressed?
●Is the patient iron deficient? If so, why?
●Is the patient deficient in folate or vitamin B12? If so, why?
History
1-Is there a recent history of loss of appetite, weight loss, fever, and/or night sweats that might indicate the presence of infection or malignancy?2-Is there a history of, or symptoms related to, a medical condition that is known to result in anemia (eg, tarry stools in a patient with ulcer-type pain, significant blood loss from other sites, rheumatoid arthritis, renal failure)?
3-Is the anemia of recent origin, subacute, or lifelong? Recent anemia is almost always an acquired disorder, while lifelong anemia, particularly if accompanied by a positive family history, is likely to be inherited (eg, the hemoglobinopathies, thalassemia, hereditary spherocytosis).
Physical examination
1-Pallor — The sensitivity and specificity for pallor in the palms, nail beds, face, or conjunctivae as a predictor for anemia varies from 19 to 70 percent and 70 to 100 percent, respectively2-Jaundice
3-Other physical findings —the presence or absence of lymphadenopathy, hepatosplenomegaly, and bone tenderness, especially over the sternum. Bone pain may signify expansion of the marrow space due to infiltrative disease, as in chronic myeloid leukemia, or lytic lesions, as in multiple myeloma or metastatic cancer
SYMPTOMS & SIGNS Specific To IRON deficiency
1- Atrophic changes in the epithelium;a- oral lesions;
I- Angular cheilosis; soreness & cracking in the corners of the lips.
II-Atrophy of the tongue papillae with intermittent glossitis
III-Stomatitis ; inflammation & soreness of of the tongue & mouth.
2-DYSPHAGIA.
3- Nail lesions; thinning & flattening of the nails progress to brittle & spoon-shaped nail ( koilonychia)





Hemorrhage in Oral Surgery
