٠٤٤١/٢٠/٢١
Upper limb injuries
Dr. Ihsan Alshamy
Fracture clavicle
٠٤٤١/٢٠/٢١
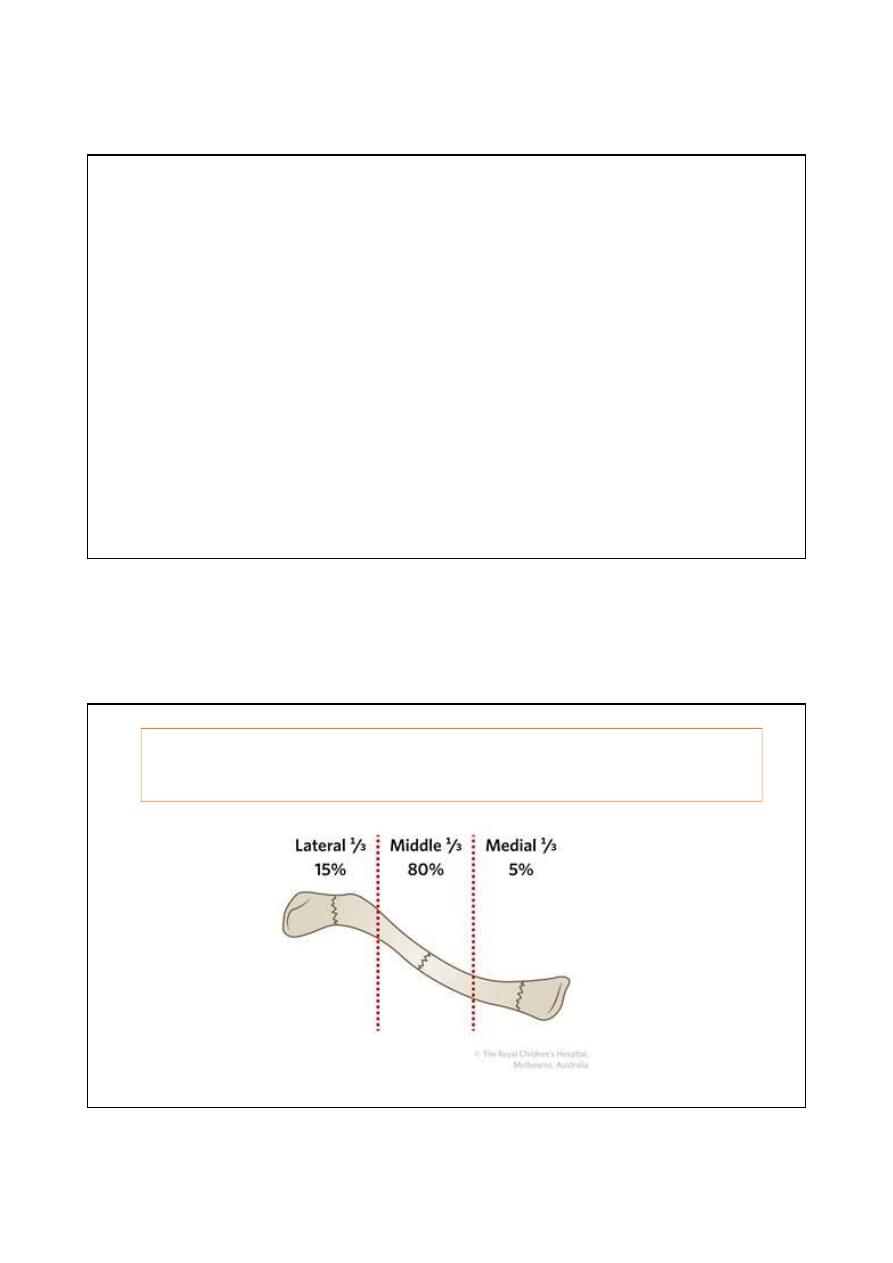
Allmans classification
Group I: fracture middle third
Group II: fracture lateral third
Group III: fracture medial third
middle third is the most common site of fracture clavicle

٠٤٤١/٢٠/٢١
Mechanism of injury
Falling on outstretched hand
Direct trauma to the shoulder
Group I
Middle third fracture
٠٤٤١/٢٠/٢١
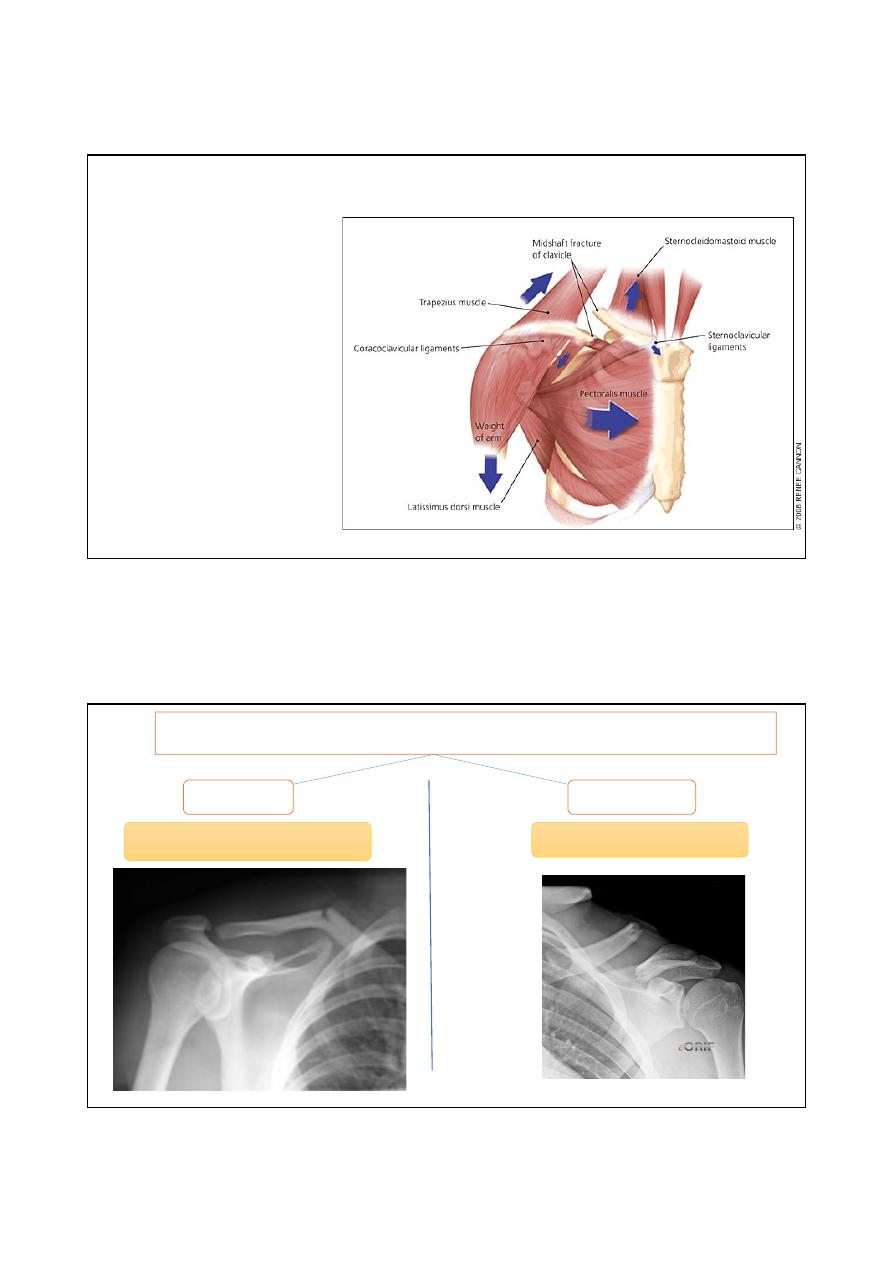
Pathoanatomy (displacement)
the medial fragment usually
pulled upward by
sternocleidomastoid muscle.
The lateral fragment pulled
downward by Wight of the
arm
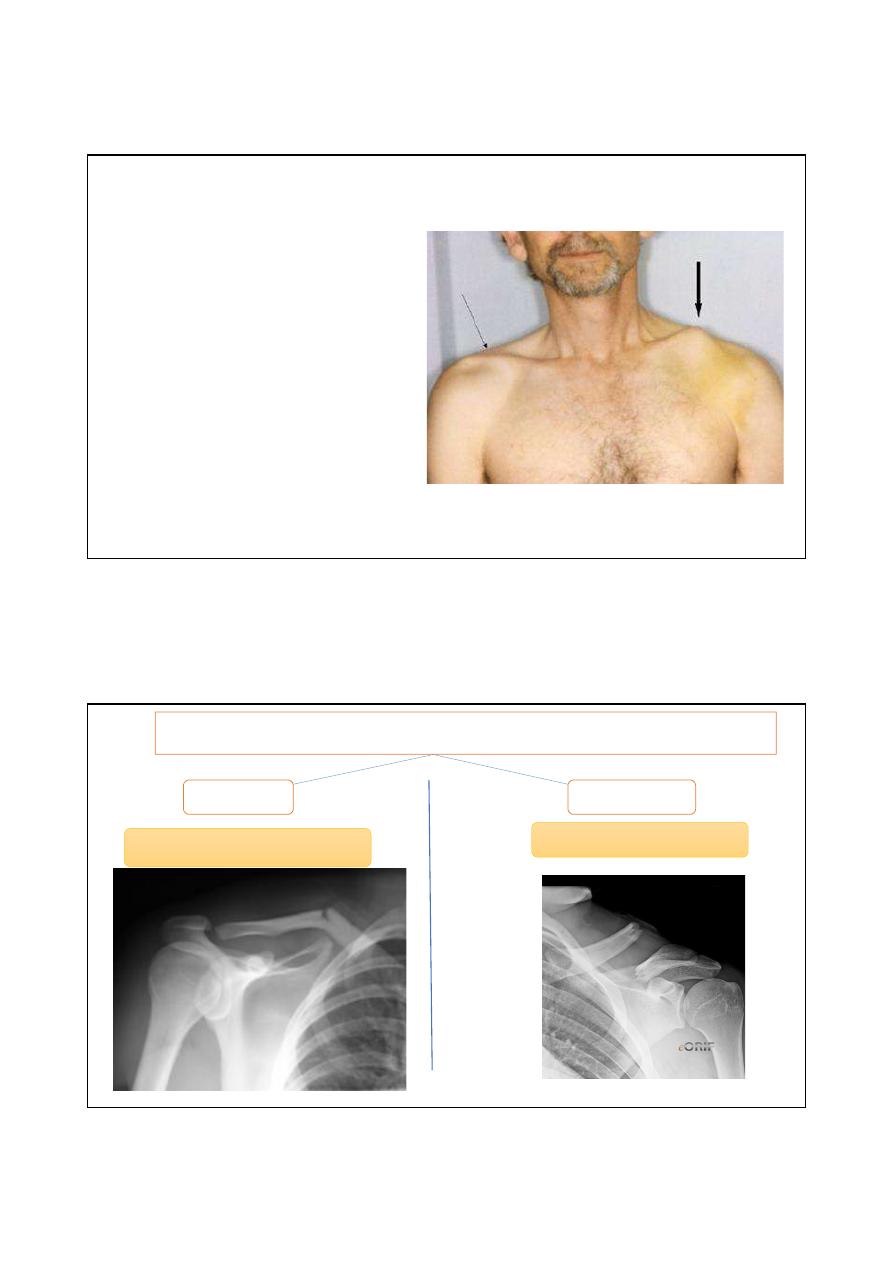
Neer classification for middle shaft fracture
Non displaced
displaced
Less than 100% displacement
Greater than 100% displacement
٠٤٤١/٢٠/٢١
Presentation
Pain
Deformity
Tenting of skin
Examine neurovascularity
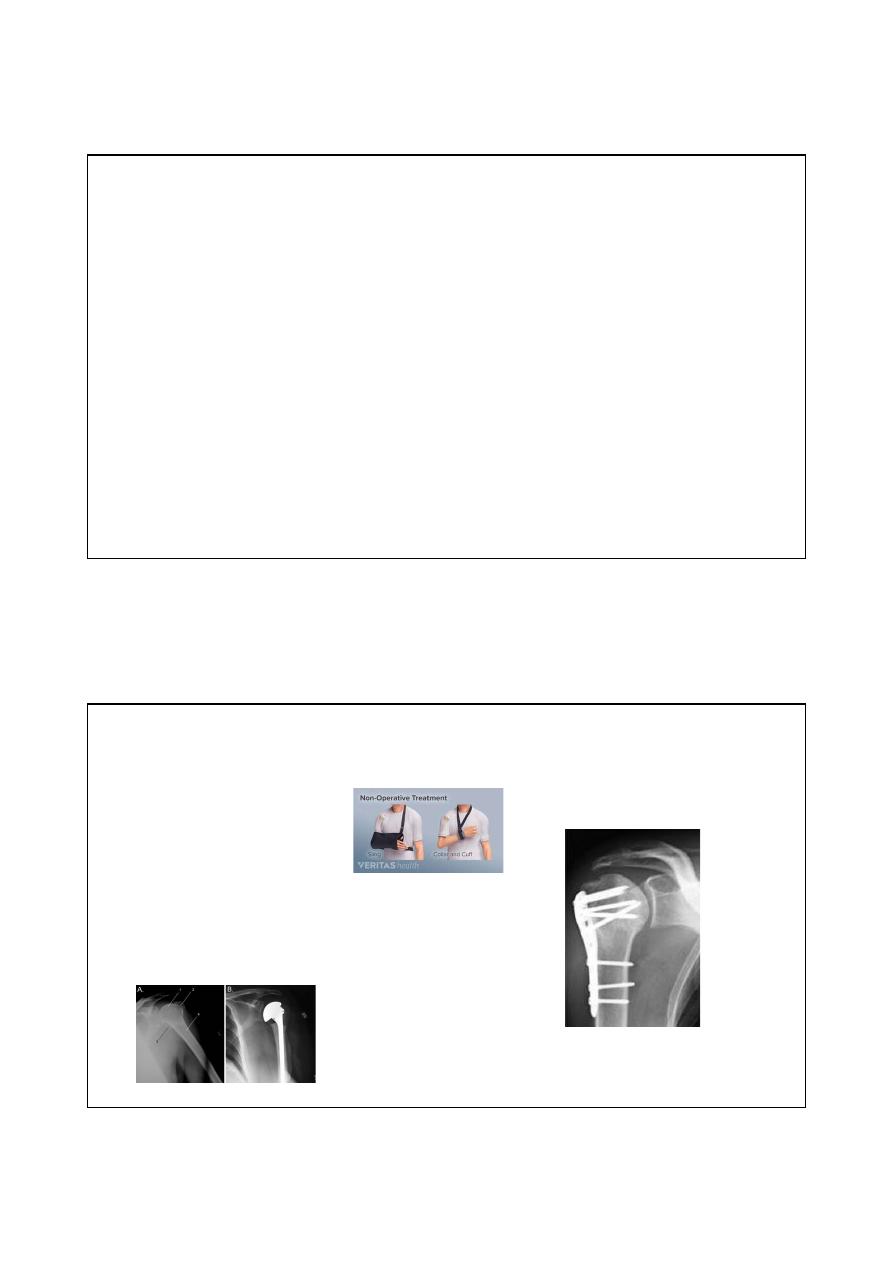
management
Non displaced
displaced
Non operative
operative
٠٤٤١/٢٠/٢١
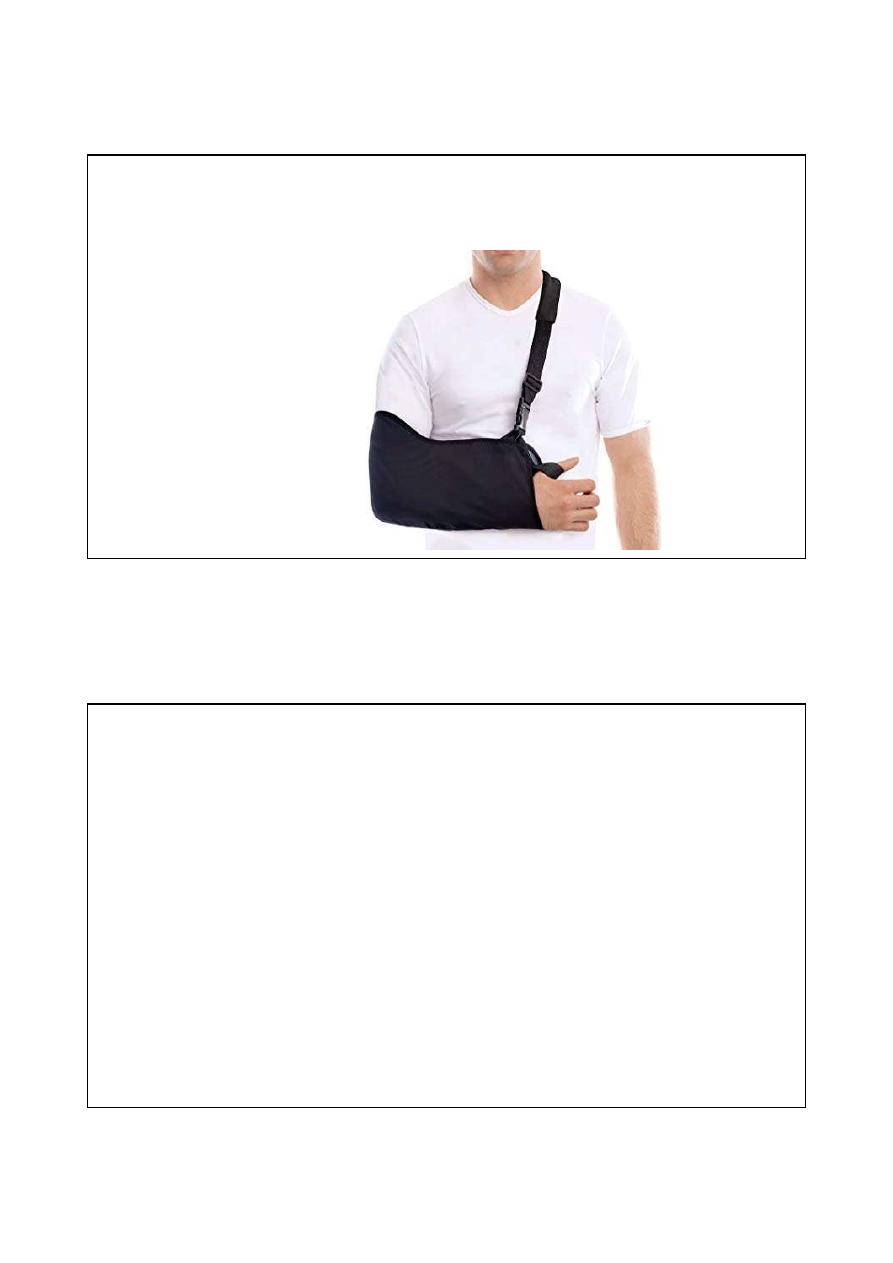
Non operative
sling immobilization with
gentle ROM exercises at 2-4
weeks
Indication for surgery
Displacement more than 100%
Tenting of skin
Open ( compound fracture)
Subclavian artery or vein injuries
Floating shoulder ( fracture clavicle and neck of scapula)
Non union
maleunion
٠٤٤١/٢٠/٢١
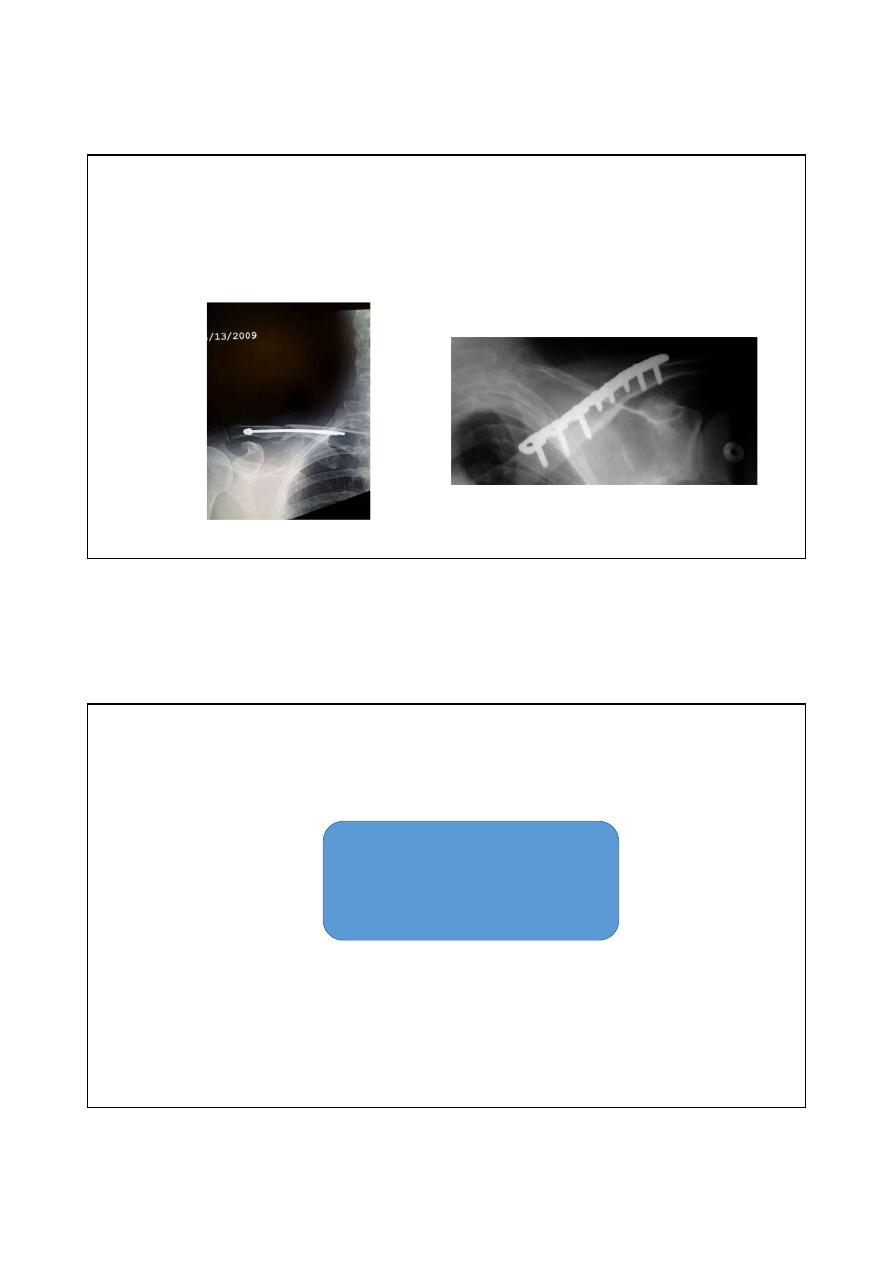
Option of surgery
Intramedullary nail
Plate and screws
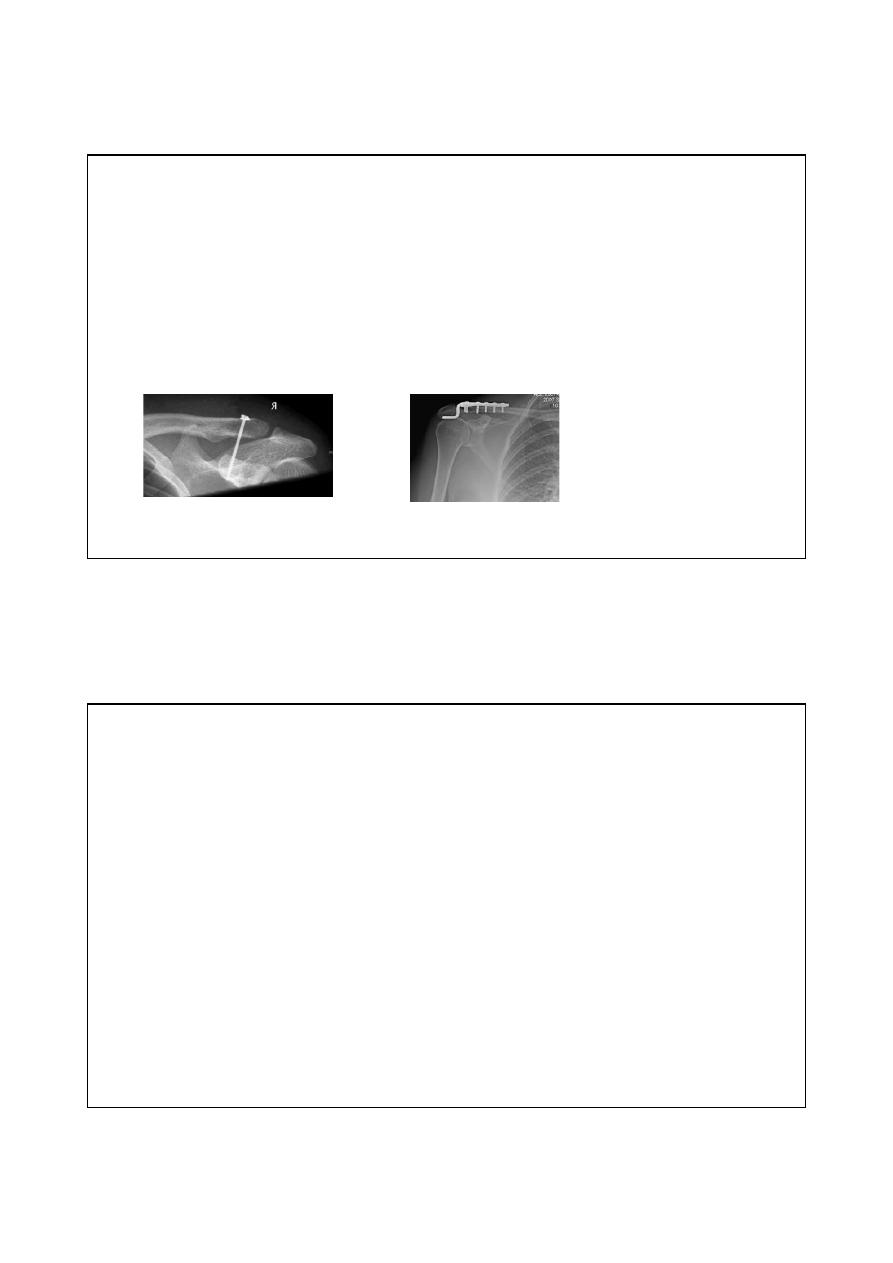
Group II
Lateral third fracture
٠٤٤١/٢٠/٢١
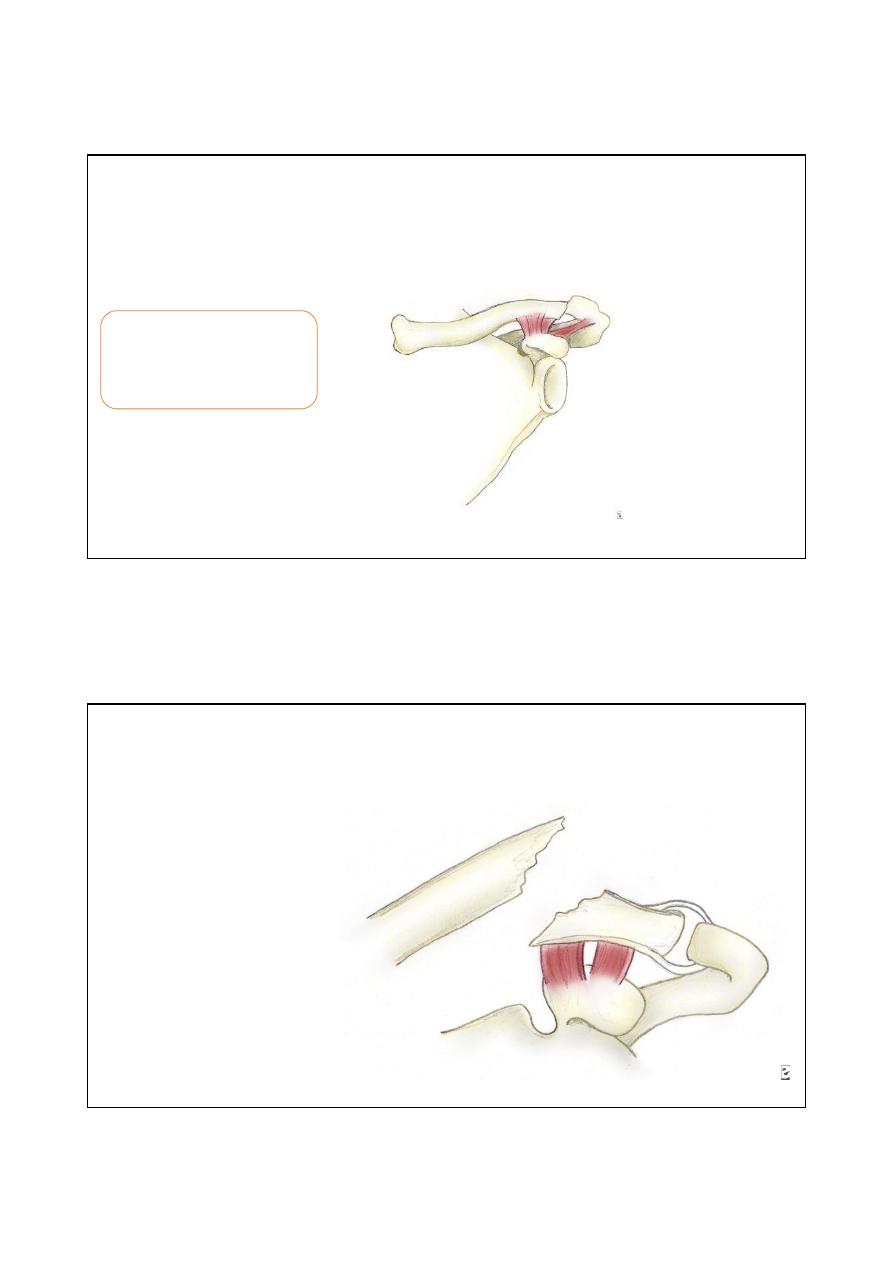
Group II subdivided into 2 subtypes
Type I fracture of the distal clavicle
(group II). The intact ligaments hold
the fragments in place.
Treatment conservative
Type II
•
A type II distal clavicle
fracture. In type IIA,
both
conoid
and
trapezoid ligaments are
on the distal segment,
while
the
proximal
segment,
without
ligamentous
attachments,
is
displaced, treatment is
operative.
٠٤٤١/٢٠/٢١
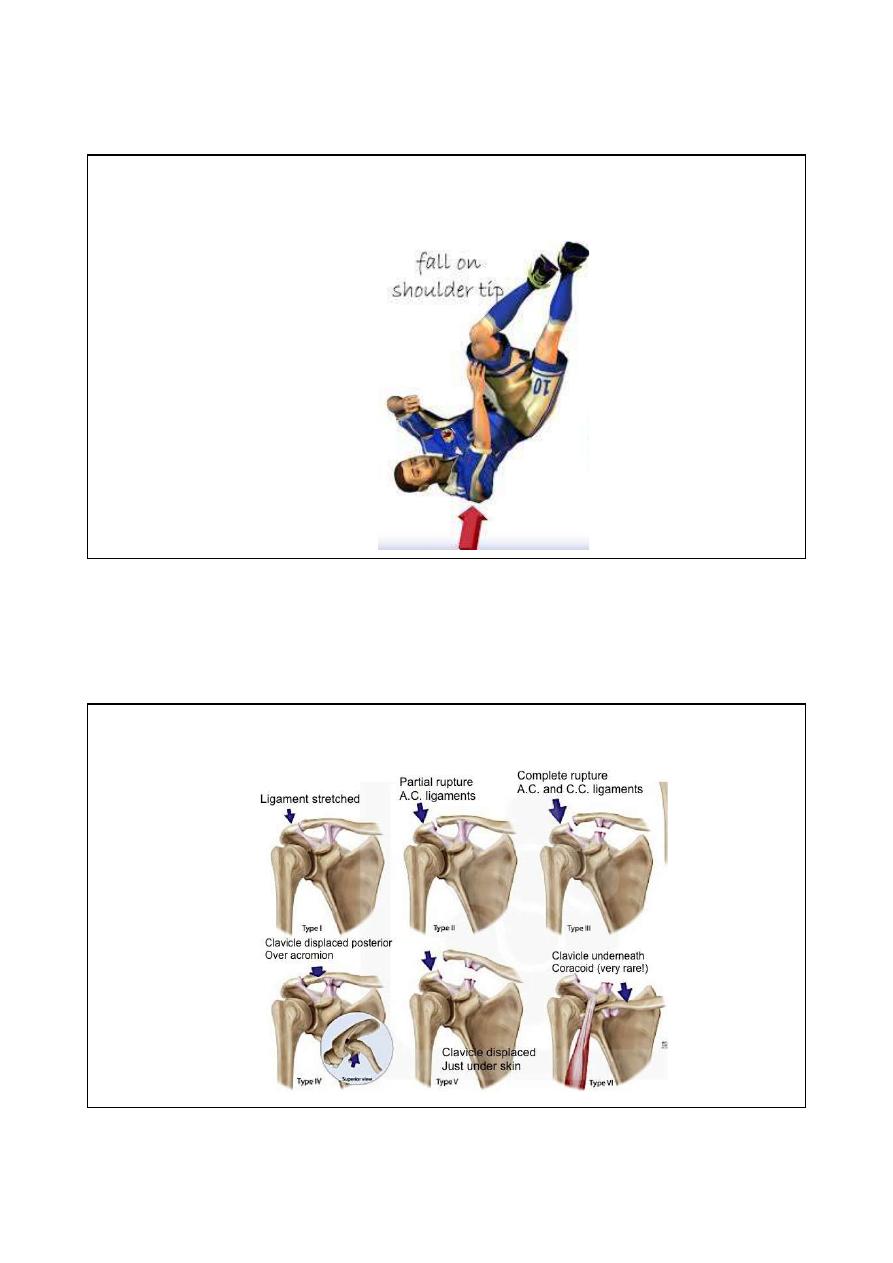
Acromioclavicular joint injuries
The most common mechanism
for an acromioclavicular joint
injury is a fall directly onto the
acromion, with the arm
adducted up against the body
Rockwood classification of AC joint injuries
٠٤٤١/٢٠/٢١
Management
Type I, type II , type III : conservative treatment by arm sling for 3-4
weeks followed by active shoulder exercises.
Type IV, V, VI need surgical fixation by coracoclavicular screw or hook
plate.
Shoulder dislocation

٠٤٤١/٢٠/٢١
types
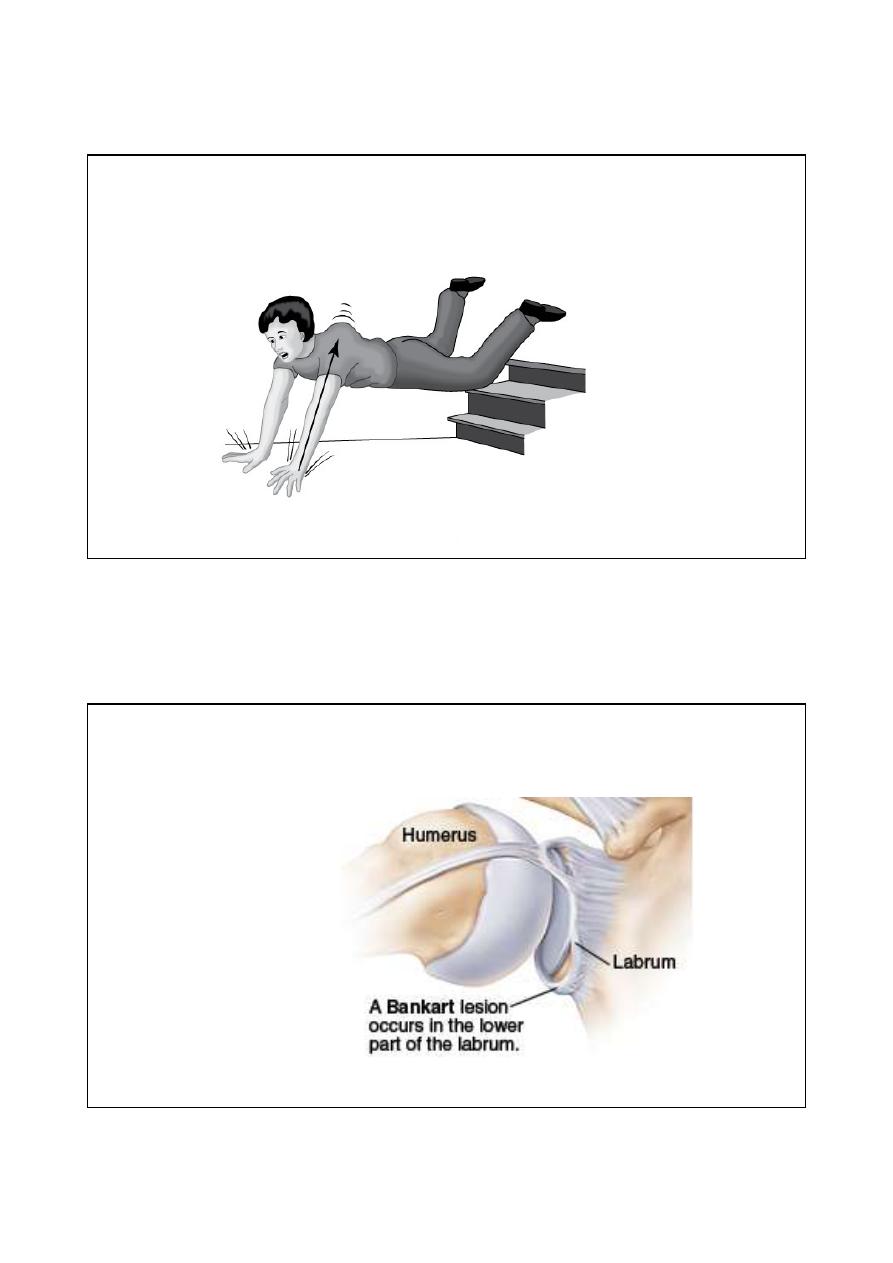
Anterior shoulder dislocation
٠٤٤١/٢٠/٢١
Mechanism of injury: Falling on out stretched hand.
Pathoanatomy
The head of humerus
driven forward tear the
capsule of the joint and
cause avulsion of glenoid
labrum ; this avulsion
called
Bankart lesion
٠٤٤١/٢٠/٢١
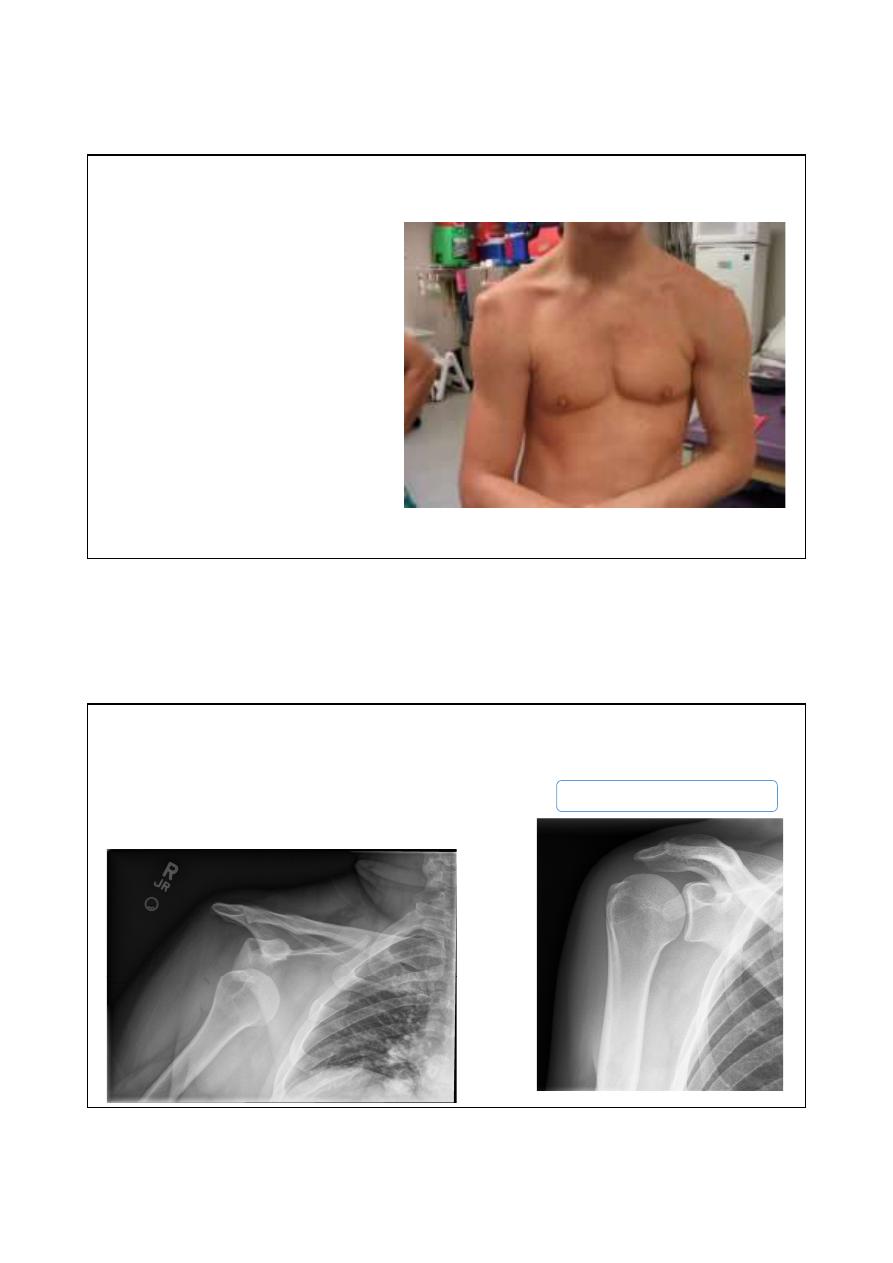
Clinical features
- Sever pain
- The patient supports the arm with
opposite hand
- Flattening of the shoulder contour
- Head of humerus can be felt below
the clavicle
X- ray AP view
X ray will show overlapping shadows of
humeral head and glenoid fossa with
head usually lying below and medial to
the socket
Normal x ray
٠٤٤١/٢٠/٢١
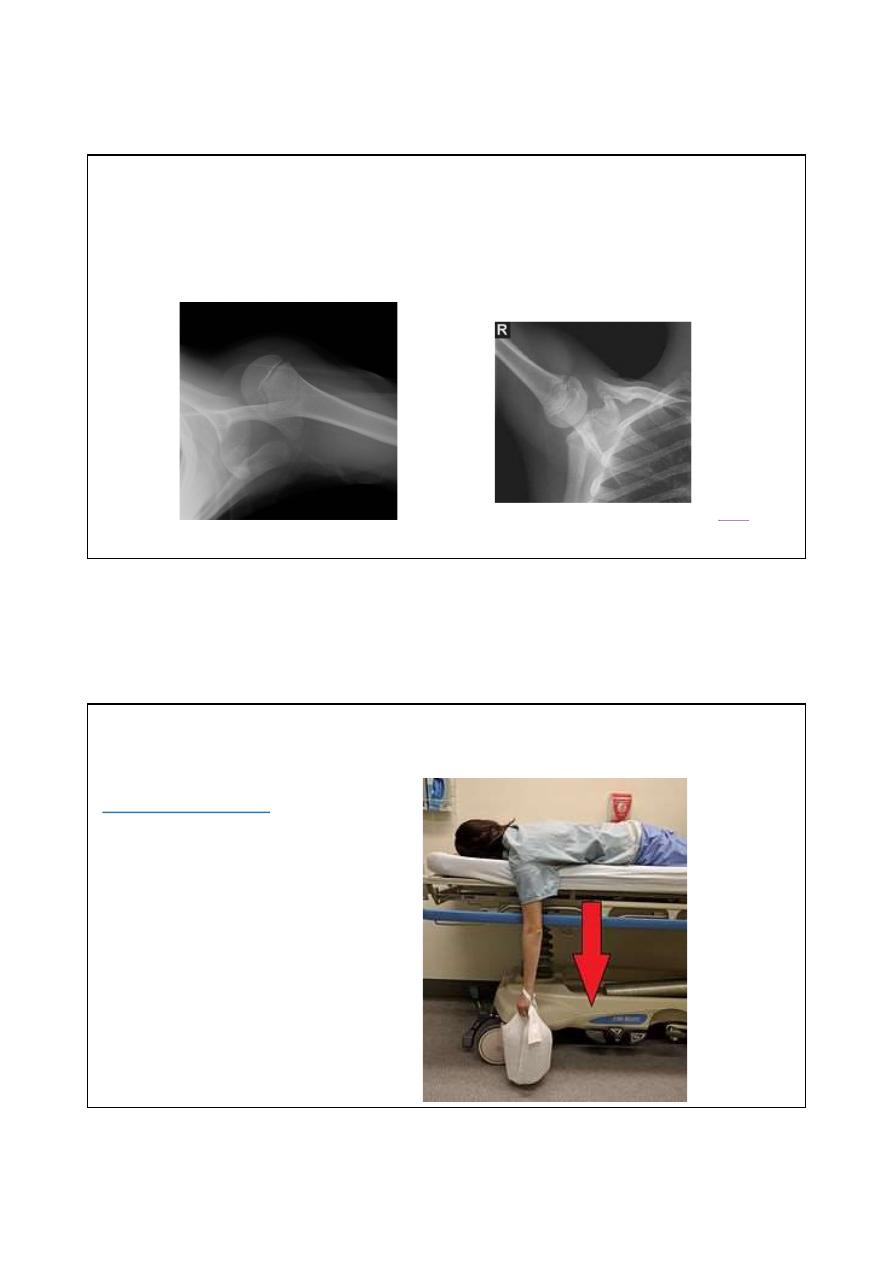
Lateral view
Anterior dislocation
Normal lateral view
Treatment is immediate reduction of the dislocation either by sedation
or by general anesthesia by one of the following methods:
:
the
Stimson
method
patient in prone position
with arm hanging over the
side of the bed after 15-20
minutes the shoulder may
reduces.
٠٤٤١/٢٠/٢١
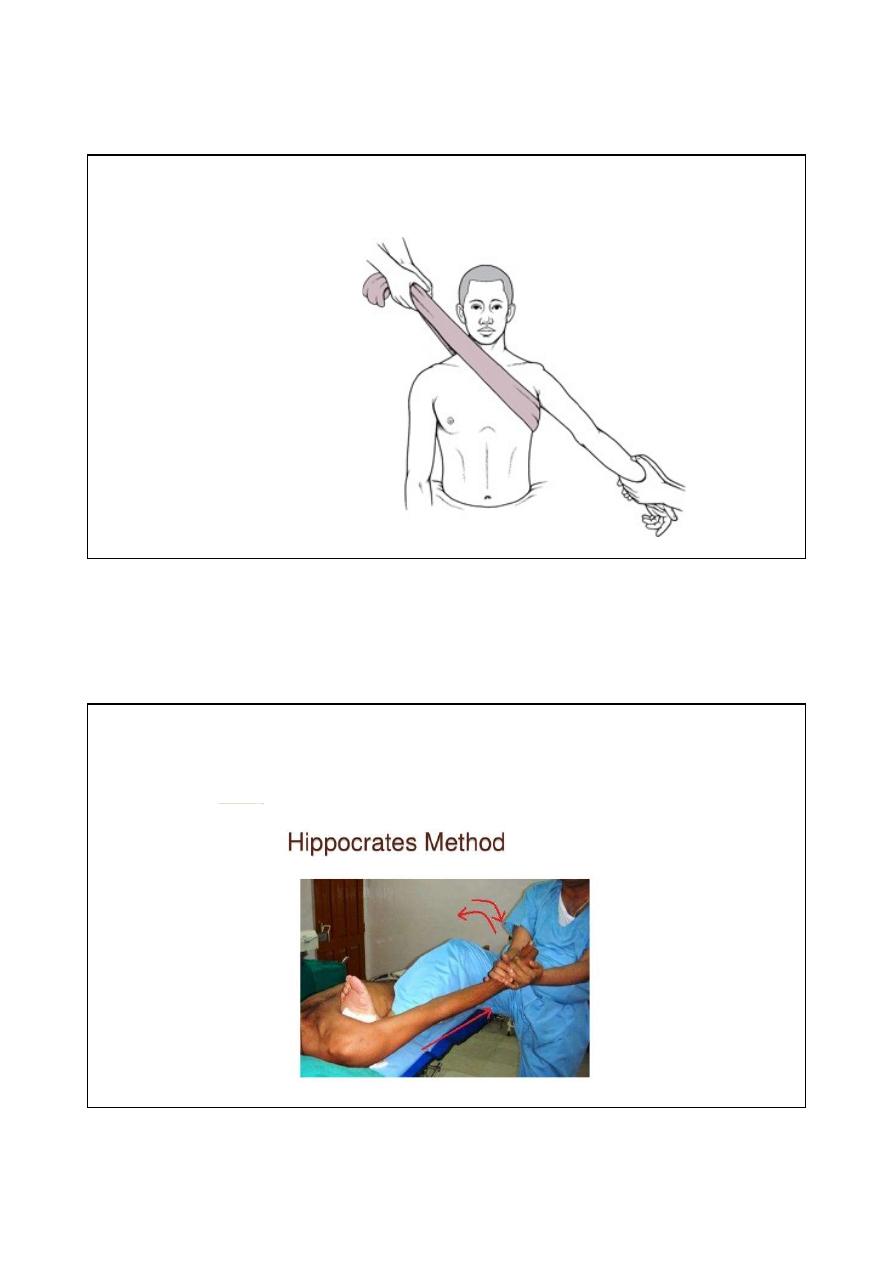
Reduction by
Hippocratic method
Supine patient ; Gently
increasing traction on
abducted arm with firm
countertraction by hand
or towel under the axilla
٠٤٤١/٢٠/٢١
After reduction
Check the neurovascularity
Take post reduction x ray
Arm sling for 3 weeks
Complication
Early
Rotator cuff tear
Axillary nerve injury
Axillary artery damage
Late
Shoulder stiffness
Unreduced dislocation
Recurrent dislocation
٠٤٤١/٢٠/٢١
Posterior shoulder dislocation
Mechanism of injury
: force causing marked internal rotation and adduction
most commonly during convulsion or electric shock.
Clinical features
: sever pain, the arm locked in internal rotation, prominent
coracoid process
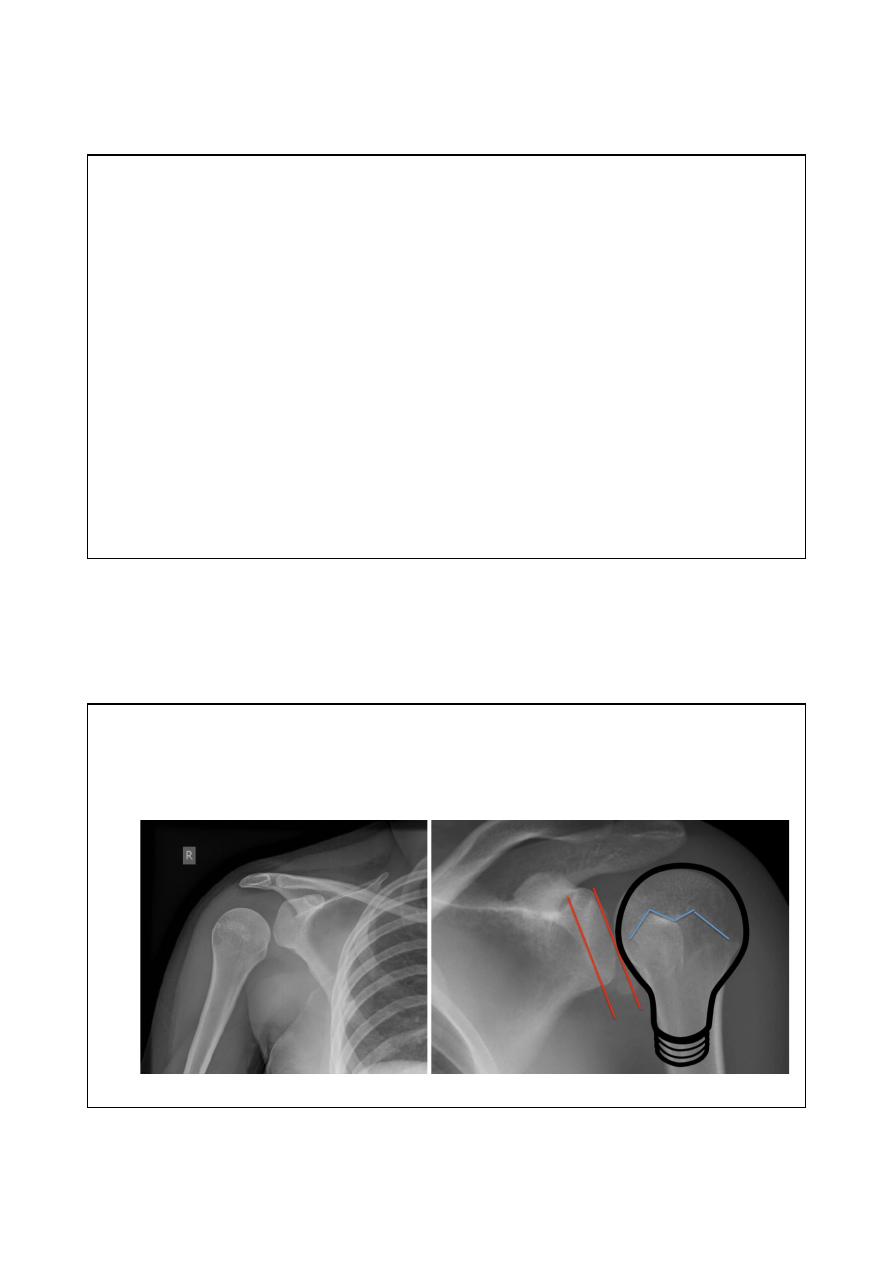
X ray
The humeral head like electric light bulb and stand away from the glenoid fossa ( empty glenoid sign).
٠٤٤١/٢٠/٢١
Treatment
Under general anesthesia, pulling on the arm with shoulder in adduction with gentle lateral rotation of the arm.
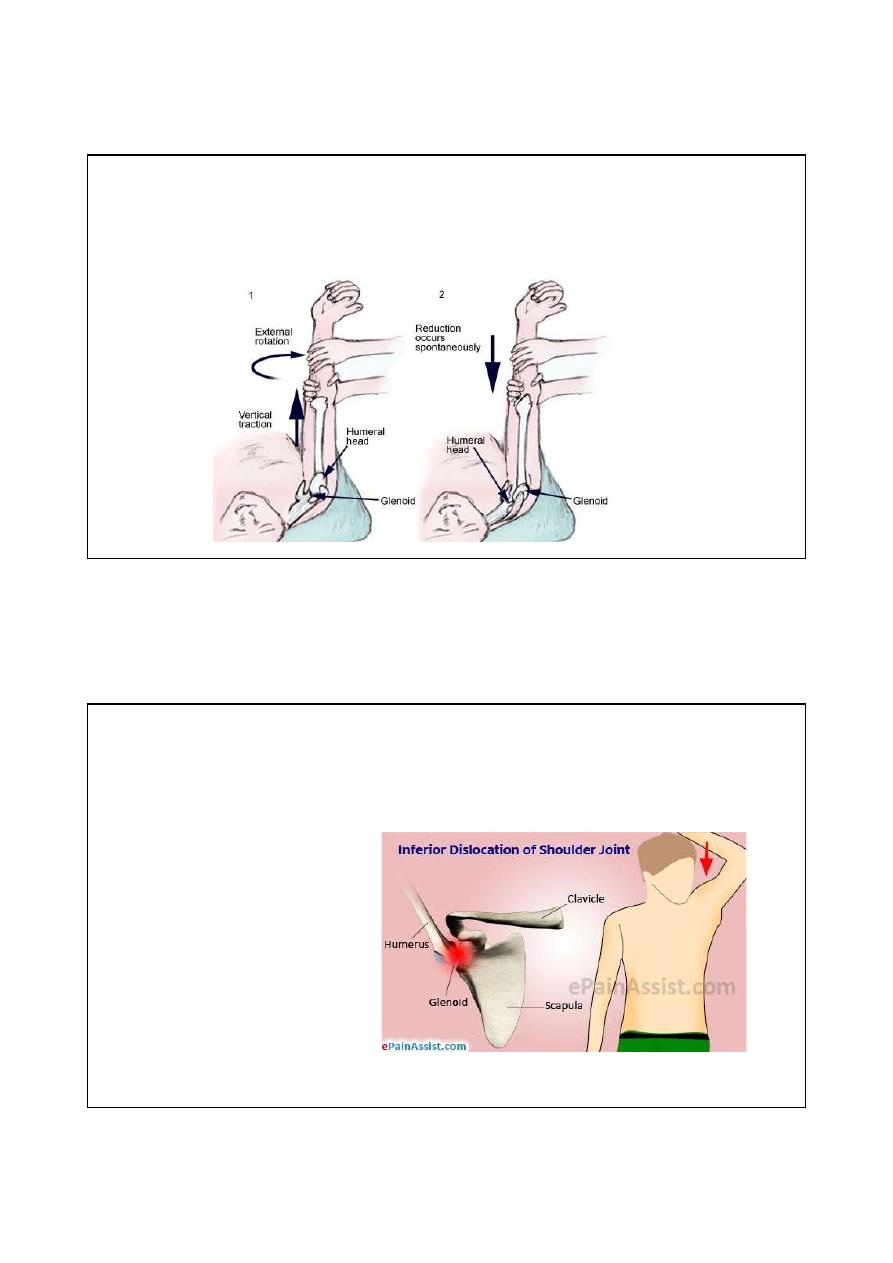
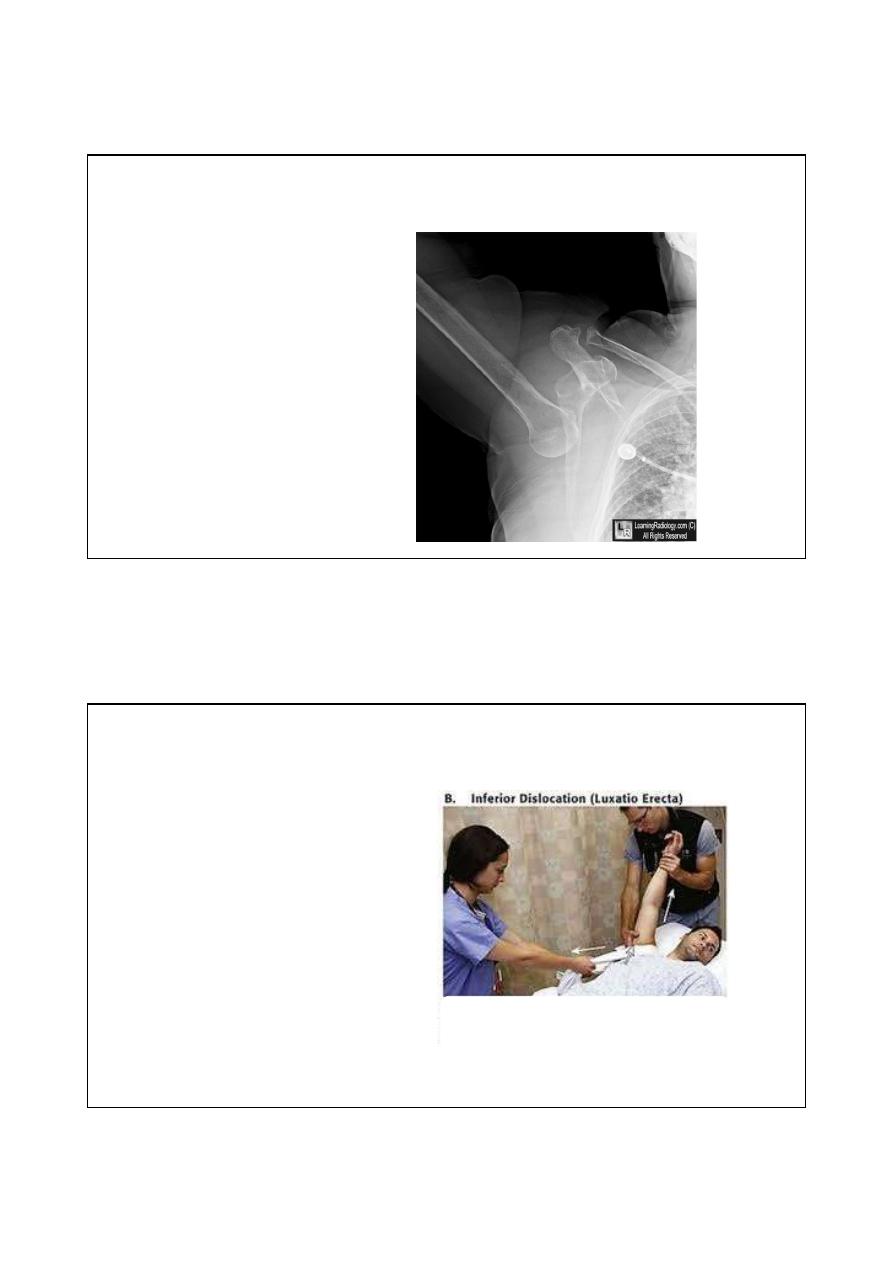
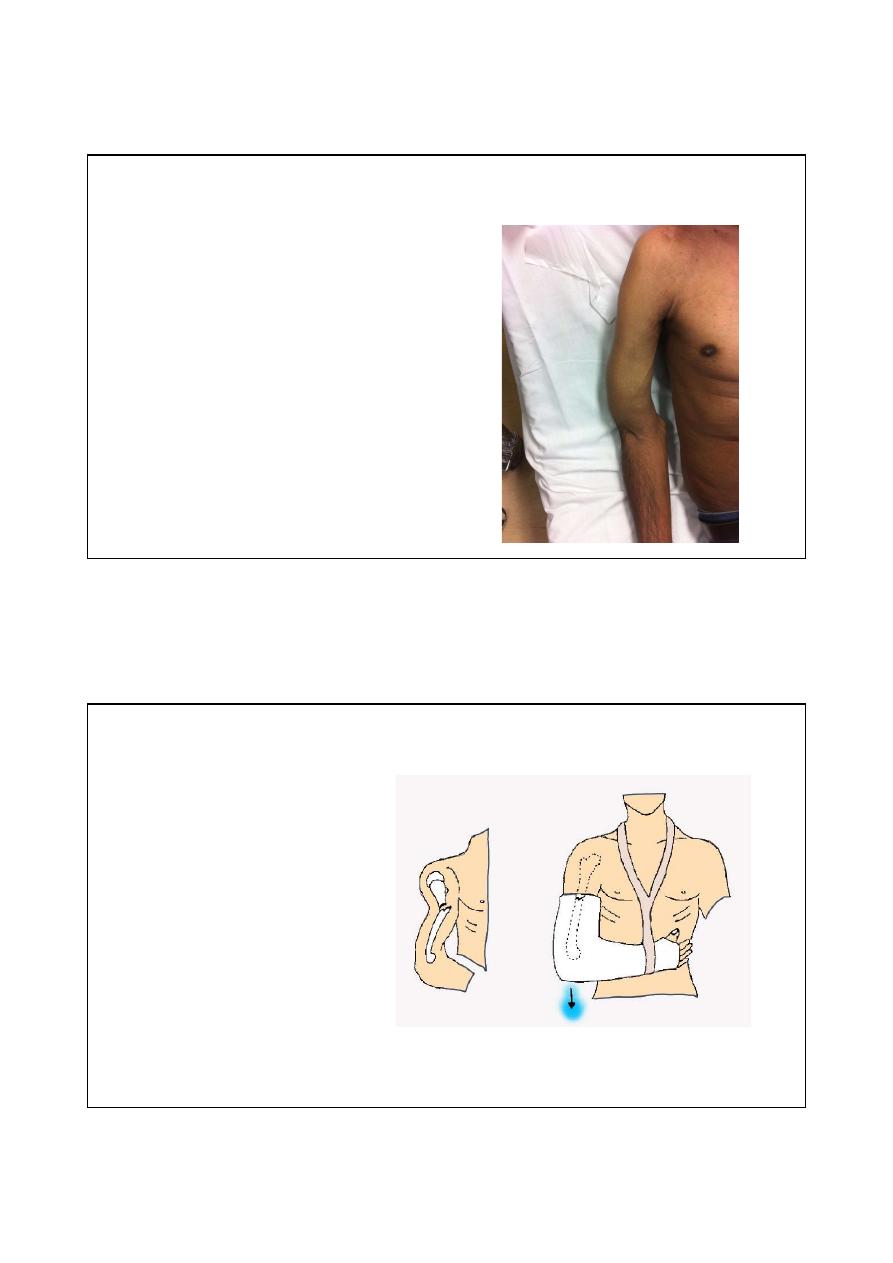
Inferior dislocation ( LUXATION ERECTA )
It is very rare; but it has
very serious complications
especially neurovascular
damage.

٠٤٤١/٢٠/٢١
Mechanism
Sever hyperabduction
force, the head of humerus
will driven below the
glenoid fossa.
Clinical features
The arm is locked in full
abduction and the head of
humerus can be palpated in the
axilla.
Checking of neurovascularity is
very important
٠٤٤١/٢٠/٢١
X ray
The humerus shaft is in
hyperabduction with
head below the glenoid
fossa
Treatment
Reduction
under
general
anesthesia by pulling upward in
the line of abducted arm with
countertraction by pulling down
over the top of the shoulder.
٠٤٤١/٢٠/٢١
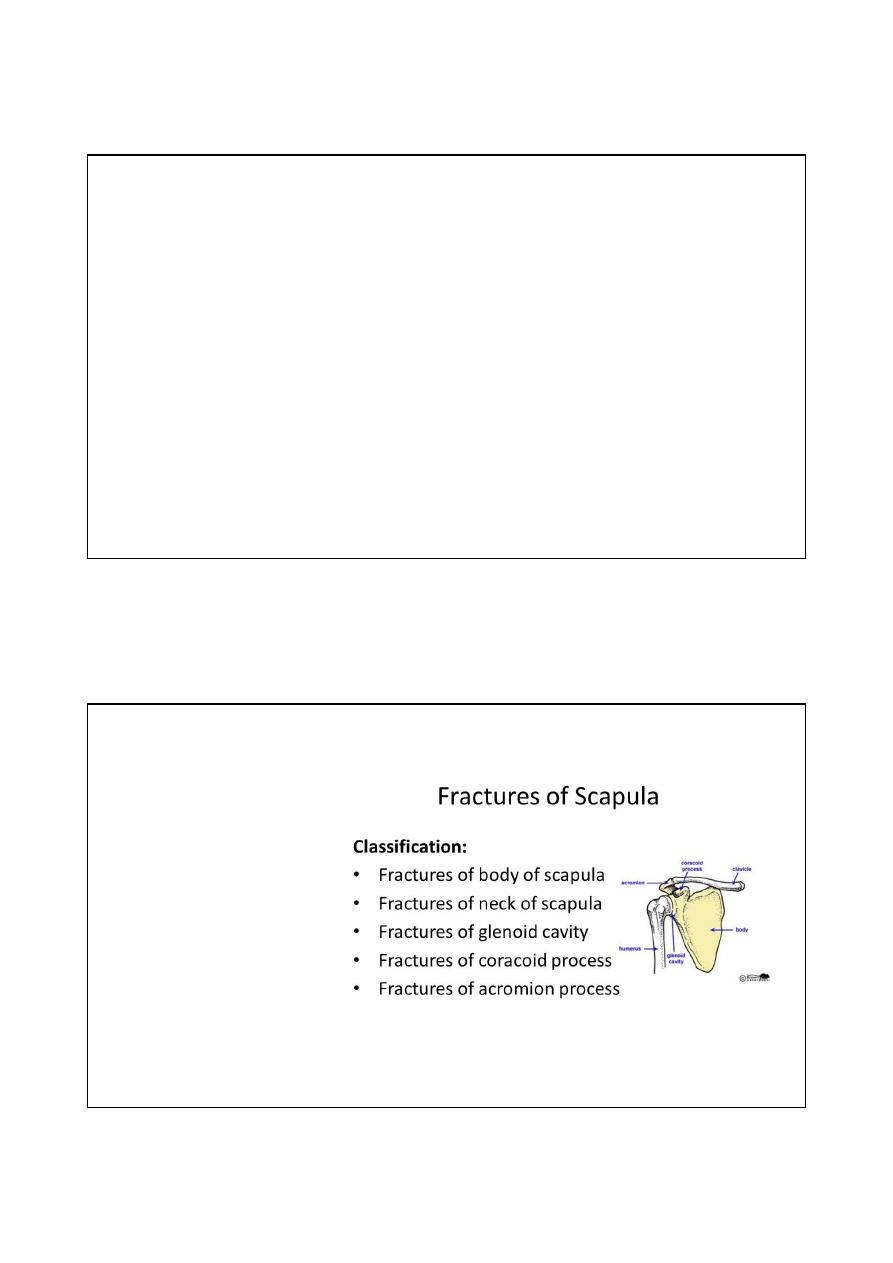
Fracture scapula
Mechanism of injury : mostly it is dueto direct crushing force to the
shoulder
.
Because it is caused by high energy trauma; many associated injuries may
occur like
:
Chest wall and rib fracture
Pneumothorax and hemothorax
Brachial plexus injury
Spine injury
Head injury
classification
٠٤٤١/٢٠/٢١
Treatment
Body fracture: arm sling for 2-3 weeks followed by physiotherapy.
glenoid fracture: arm sling for 2-3 weeks followed by physiotherapy
Intraarticular fracture: usually treated by surgery
Fracture acromion: Undisplaced fracture treated by arm sling, greatly displaced fracture treated by
fixation.
Fracture coracoid process: fracture distal to coracoclavicular ( CC) ligament treated arm sling; fracture
proximal to ( CC) ligament need fixation. a
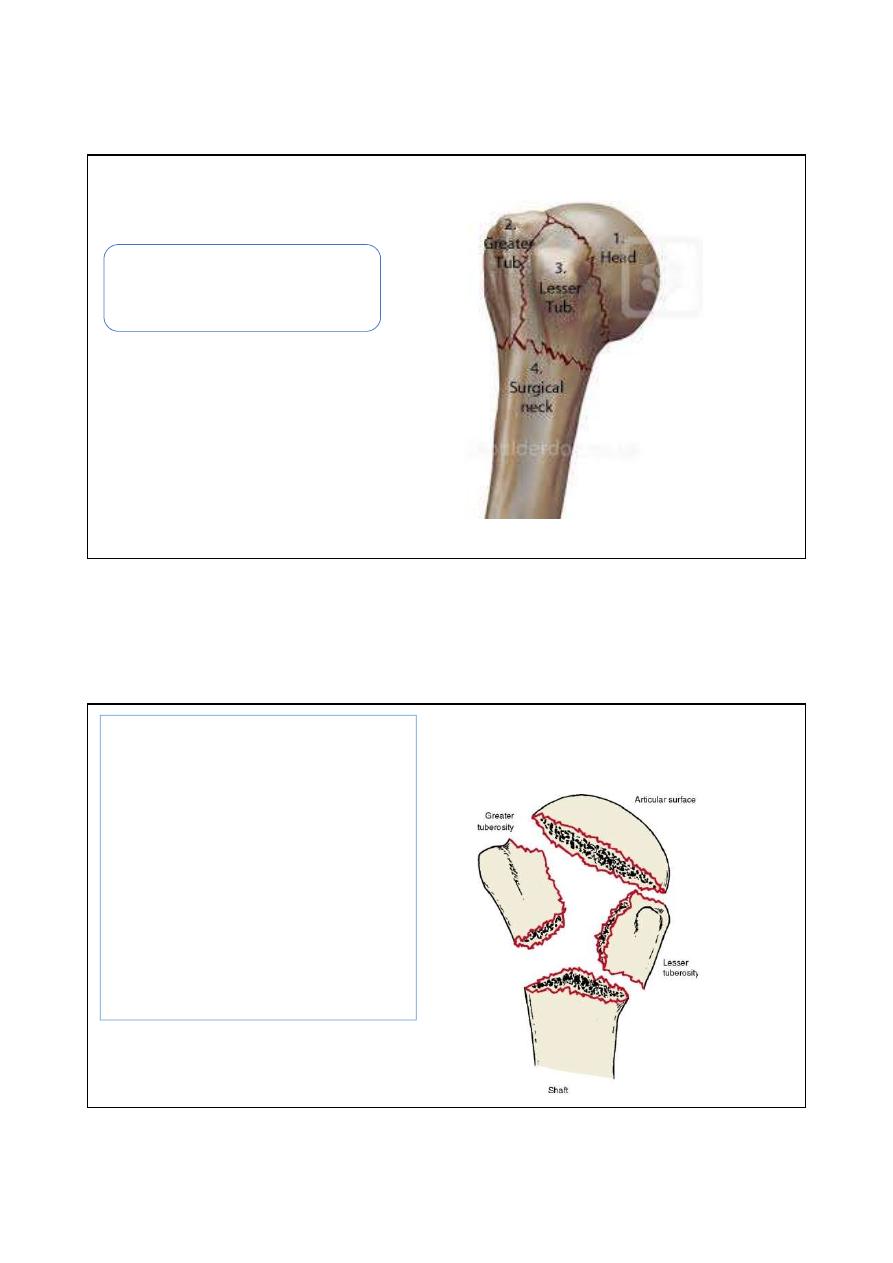
Fracture proximal humerus
٠٤٤١/٢٠/٢١
It is one of osteoporotic fracture which occurs
in elderly patients. Usually caused by falling on
outstretched hand.
Neer classification
It depends on whomany major fragment is displaced among
the following 4 major fragment constituting the head of
humerus :
-Head of humerus
-Greater tuberosity
-Lesser tuberosity
-Shaft
Displacement defined as angulation more than 45 degree or
1cm separation.
So if no displaced fragment it classified as one part fracture, if
one fragment is displaced it classified 2 parts fragment;
likewise 3 part and 4 parts fracture.
٠٤٤١/٢٠/٢١
Clinical features
Pain
Bruises over the shoulder
Check for axillary nerve injury
Management
One part fracture treated by rest in arm sling for 3-4 weeks followed by active shoulder exercises after 6 weeks.
2parts and 3 parts fractures usually treated by open reduction and internal fixation.
4 parts fracture treated by shoulder arthroplasty
٠٤٤١/٢٠/٢١
Fracture shaft of humerus
Mechanism of injury
Direct trauma by bullet, RTA
Indirect by falling on the hand or elbow
Pathological fracture ( metastasis or infection)
٠٤٤١/٢٠/٢١
Clinical features
The arm is bruised; swollen and deformed.
Asses radial nerve injury by asking the patient to do
active dorsiflexion of fingers.
Dorsiflexion of the wrist may be misleading because
extensor carpiradialis sometimes supplied by a branch
arising proximal to injury.
Treatment
Usually treated by hanging
cast with elbow flexed 90
degree for 8-10 weeks, the
weight of the cast is enough
to pull the fragments into
alignment.
٠٤٤١/٢٠/٢١
Indications of surgery
Multiple injuries
Open fracture
Segmental fracture
Intraarticular extension of the fracture
Pathological fracture
Floating elbow( fracture humerus and forearm bones)
Radial nerve palsy after manipulation
Non union
Radial nerve palsy in fracture humerus shaft
Radial nerve palsy in fracture humerus usually is neuropraxia ( temporary) ;
so we should wait up to 12 weeks as spontaneous recovery may occurs.
Radial nerve palsy which occurs after manipulation of fracture should be
treated by immediate nerve exploration.
٠٤٤١/٢٠/٢١
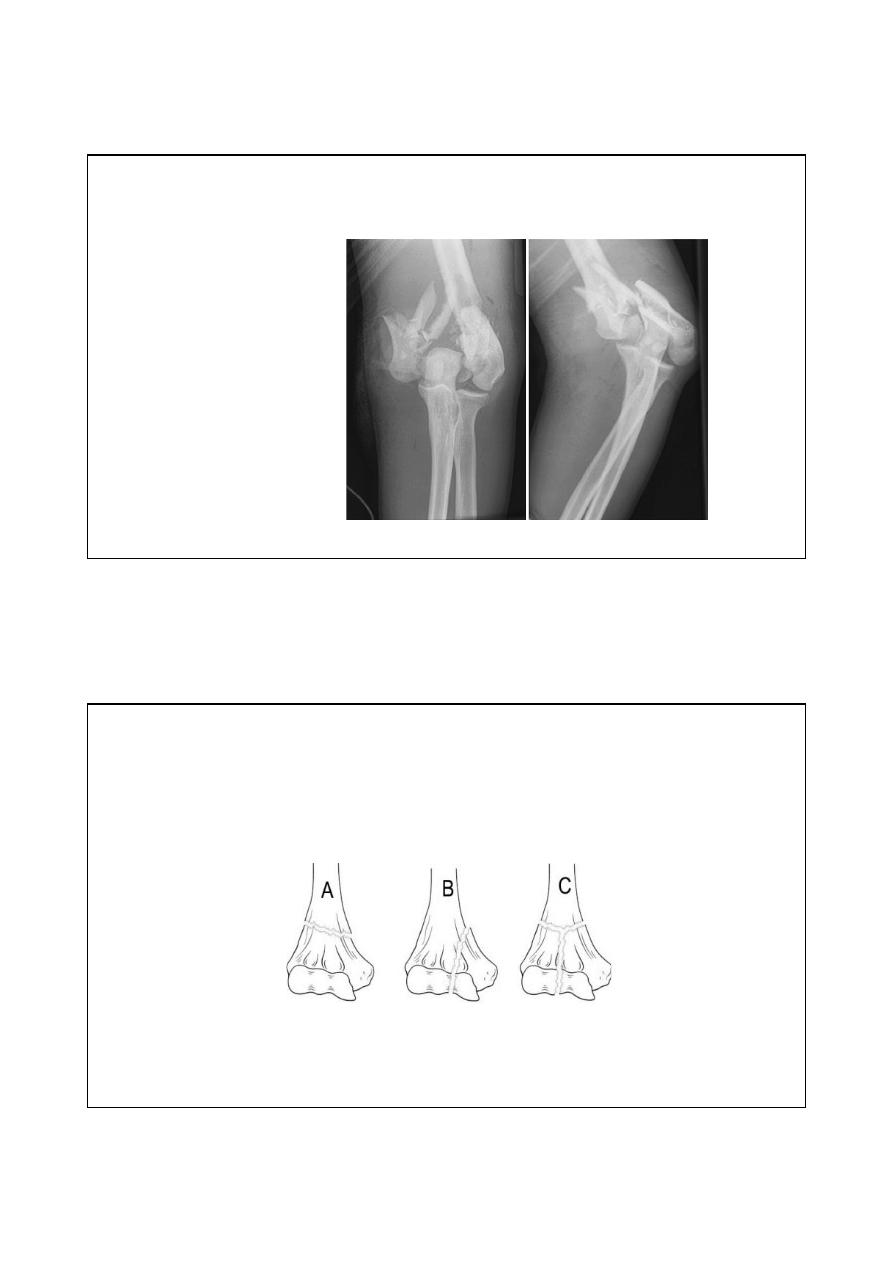
Supracondylar fracture in adult
It is a high energy
fracture associated
with vascular and
nerve injuries.
AO classification of distal humerus fracture in adult
Type-A: extraarticular supracondylar fracture
.
Type-B: Intraarticular unicondylar fracture
Type-C: Intraarticular bicondylar fracture
.
٠٤٤١/٢٠/٢١
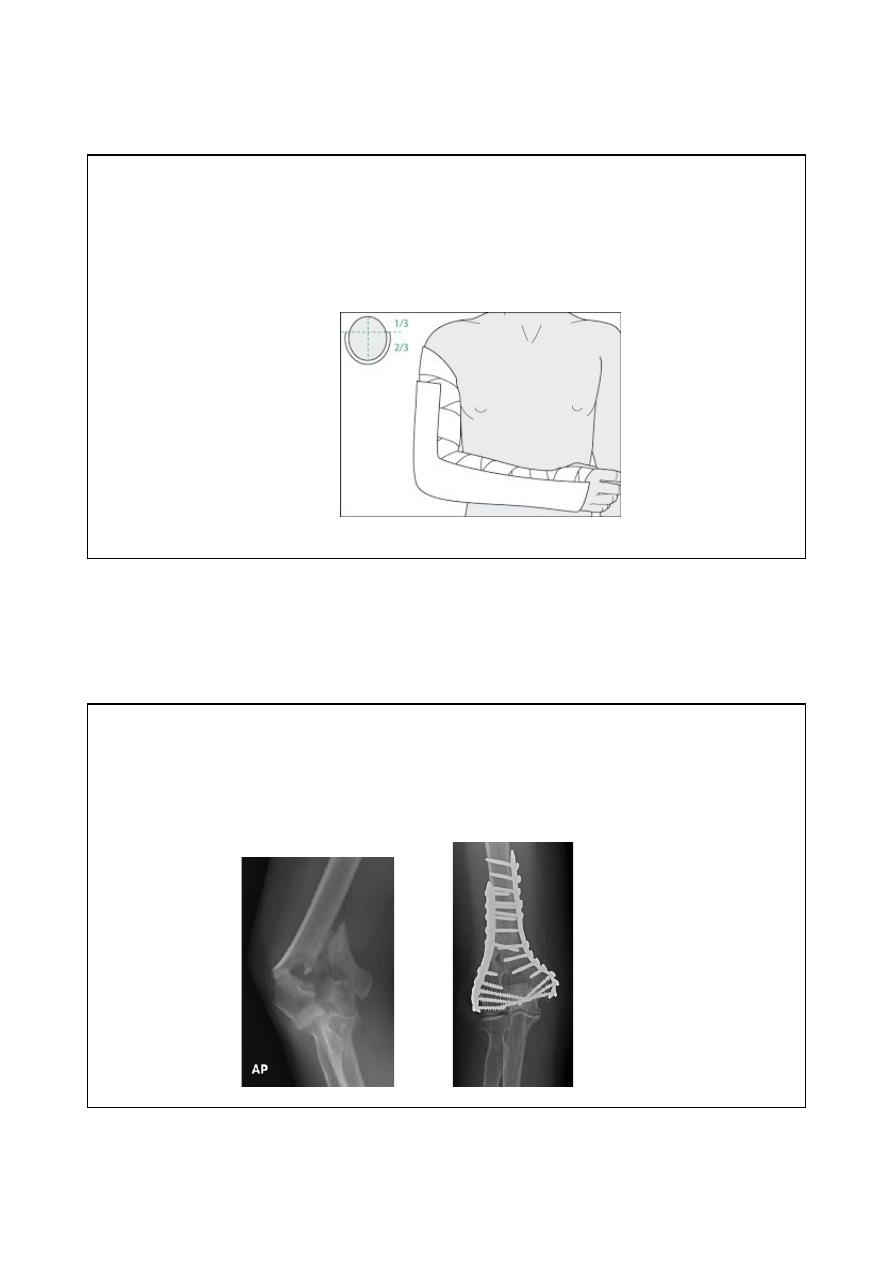
treatment
Undisplaced fracture treated by a posterior slab with elbow 90 degree
flexed for 2 weeks followed by early physiotherapy to prevent elbow
stiffness.
Displaced fracture
Open reduction and internal fixation by countered plates and screws
٠٤٤١/٢٠/٢١
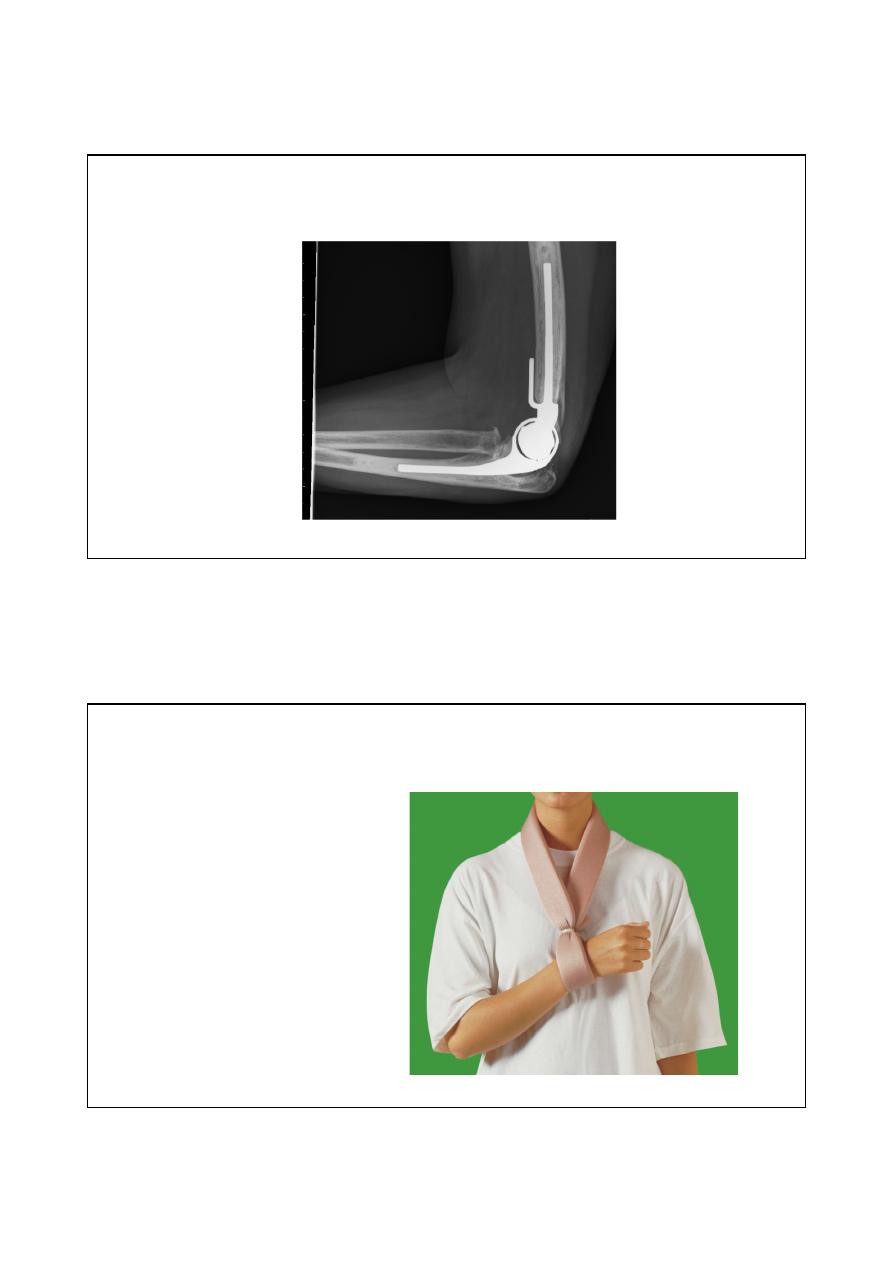
Comminuted fracture in elderly osteoporotic patient treated by
elbow replacement
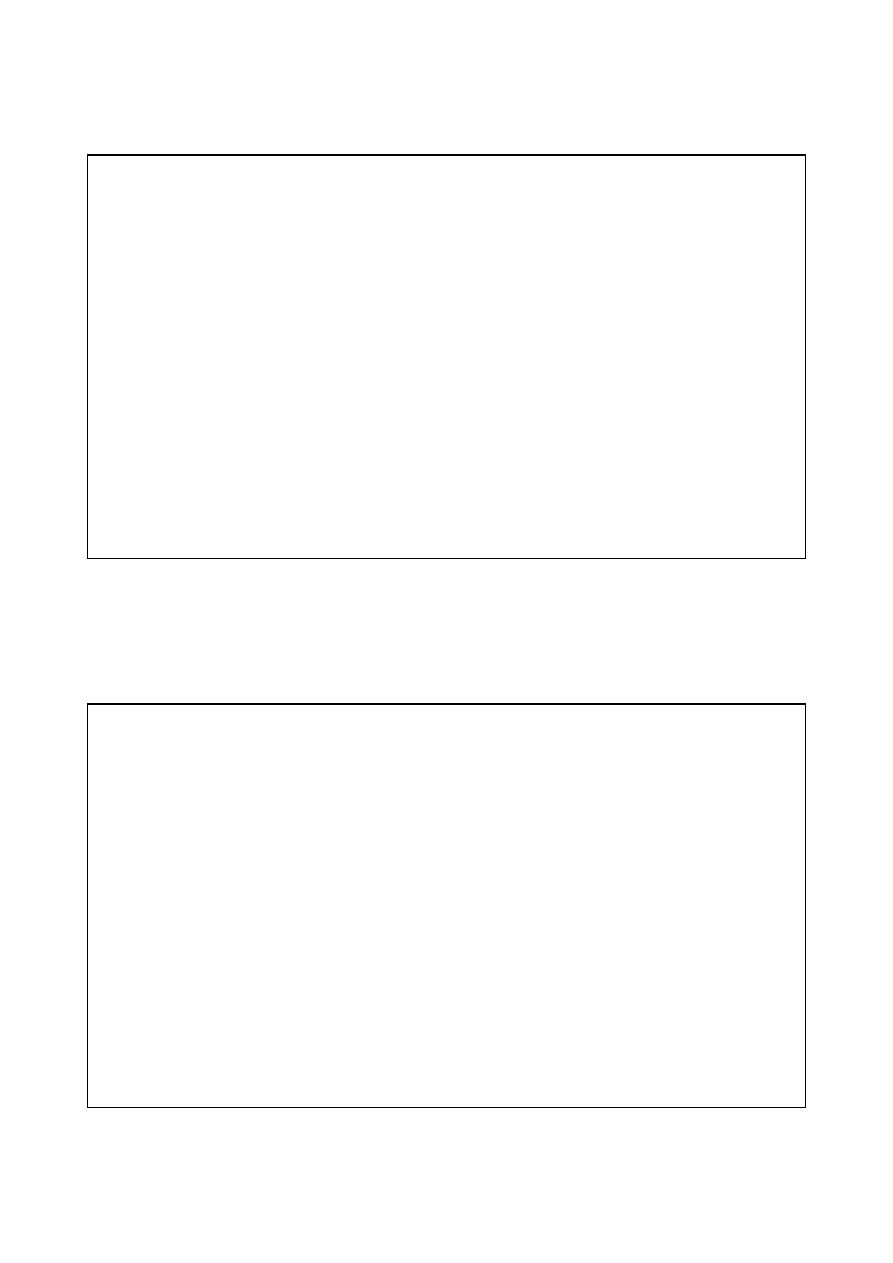
Bag of bone technique
The arm is held in a collar and cuff with elbow
flexed above 90 degree for 6-8 weeks, used also
for severely comminuted fracture
٠٤٤١/٢٠/٢١
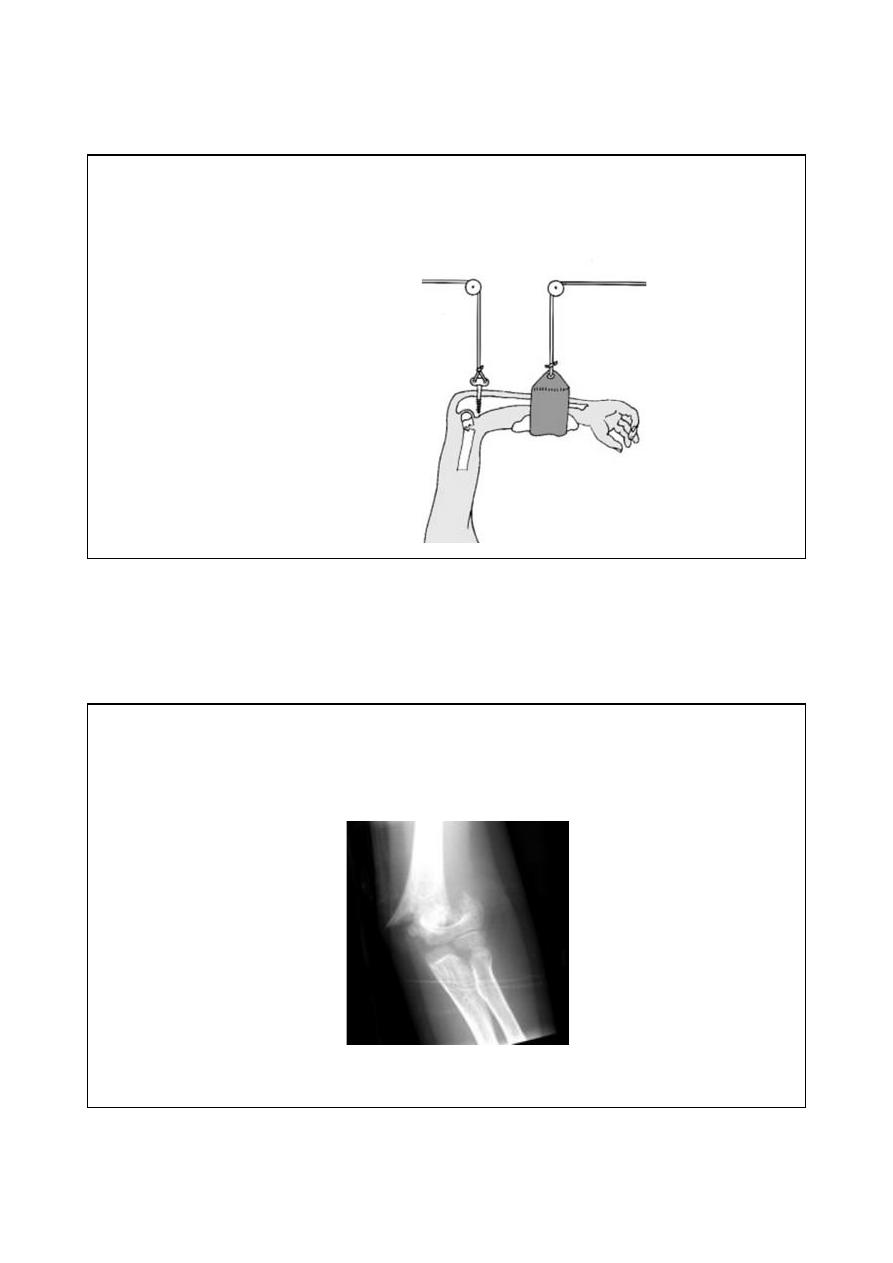
Skeletal traction
Other option for severely
comminuted fracture is skeletal
traction through olecranon
process.
Supracondylar fracture in children
It is the one of the most common fracture in pediatric age group
٠٤٤١/٢٠/٢١
Mechanism of injury
Fall on out stretched hand
95% displaced posteriorly
May cause injury to brachial artery or median nerve.
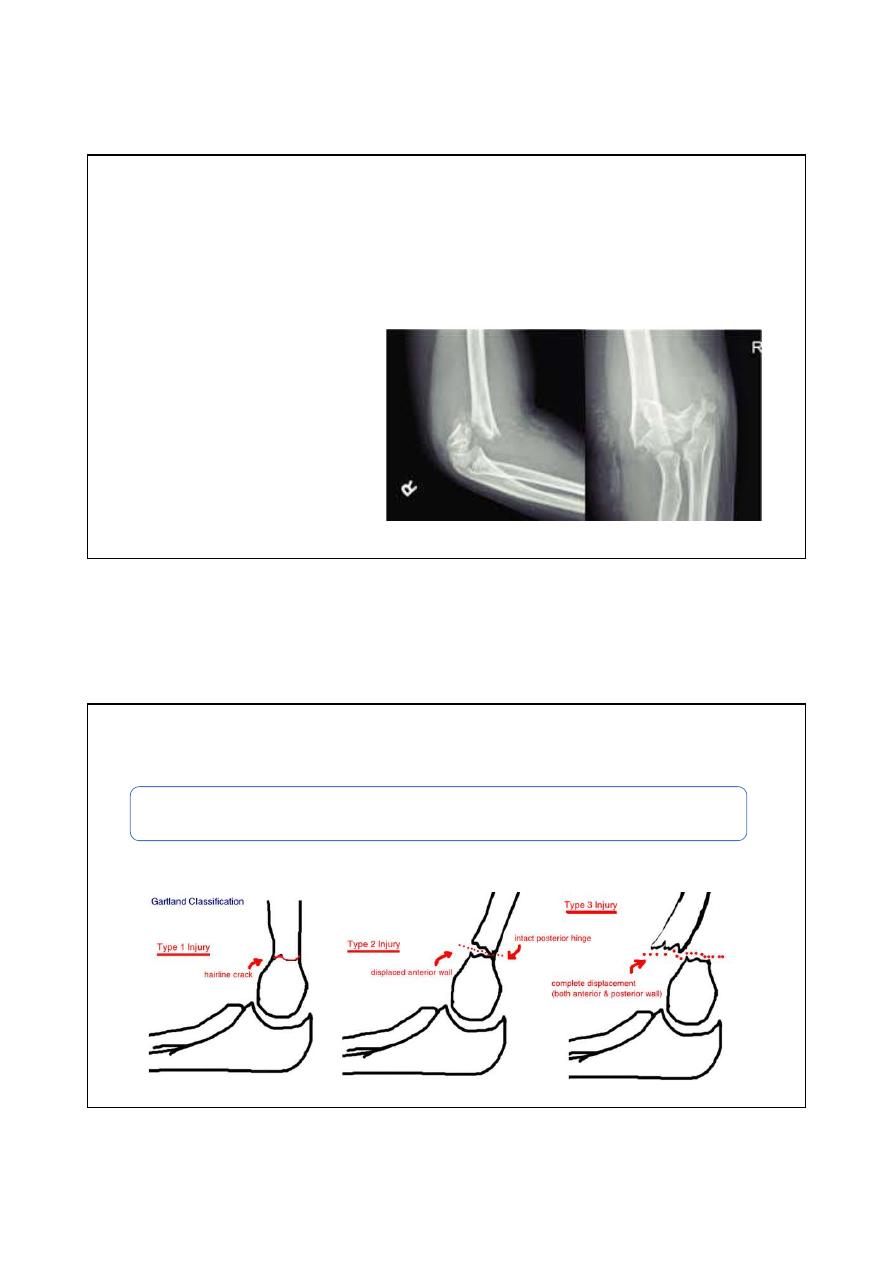
Gartlands classification
Type-I: Undisplaced
Type-II: displaced but the posterior cortex still in contact
Type-III: completely displaced
٠٤٤١/٢٠/٢١
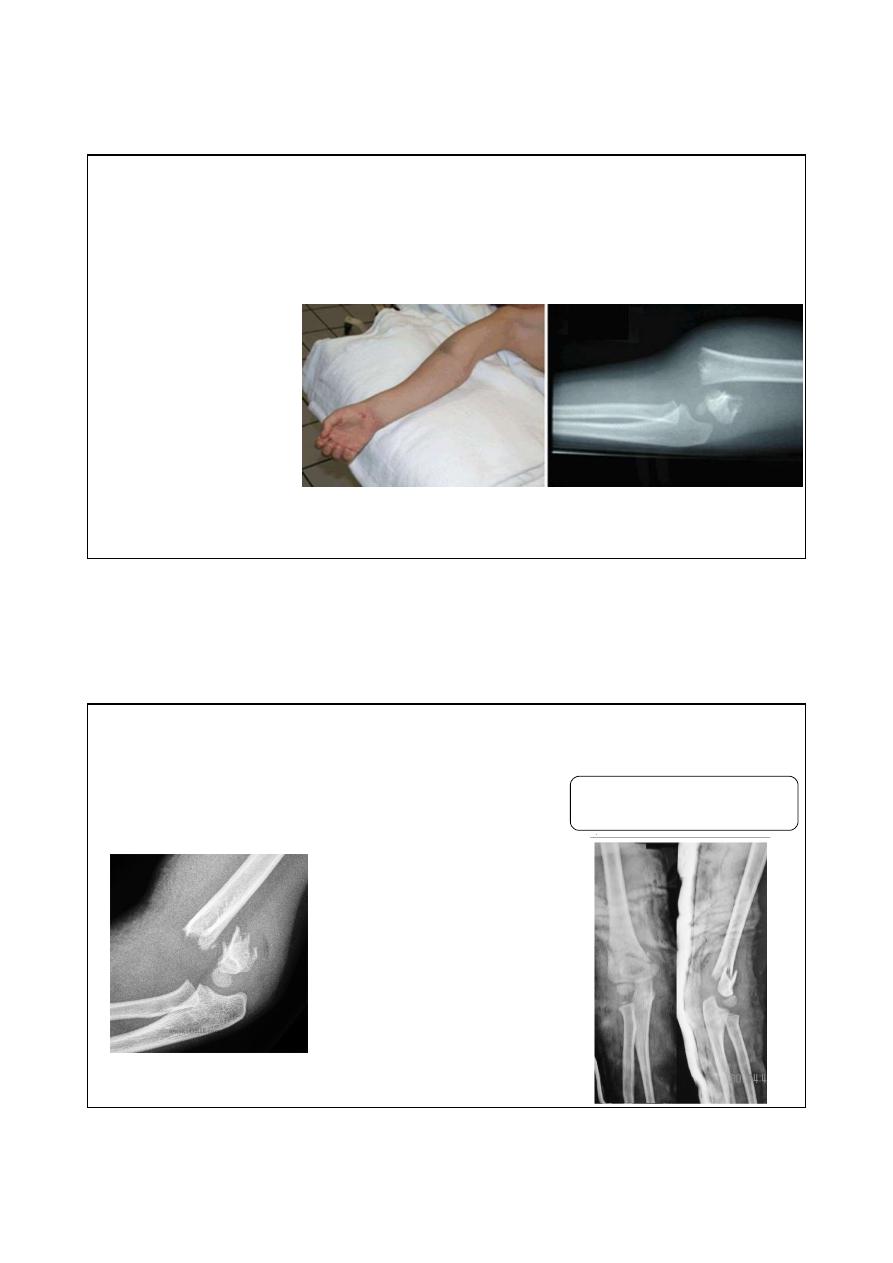
Clinical features
Swollen elbow
S shape deformity
Check the vascularity
Check for nerve injury
X-ray
Best view is lateral view: posteriorly
displaced distal fragment in 95%.
5% anteriorly displaced fragment
٠٤٤١/٢٠/٢١
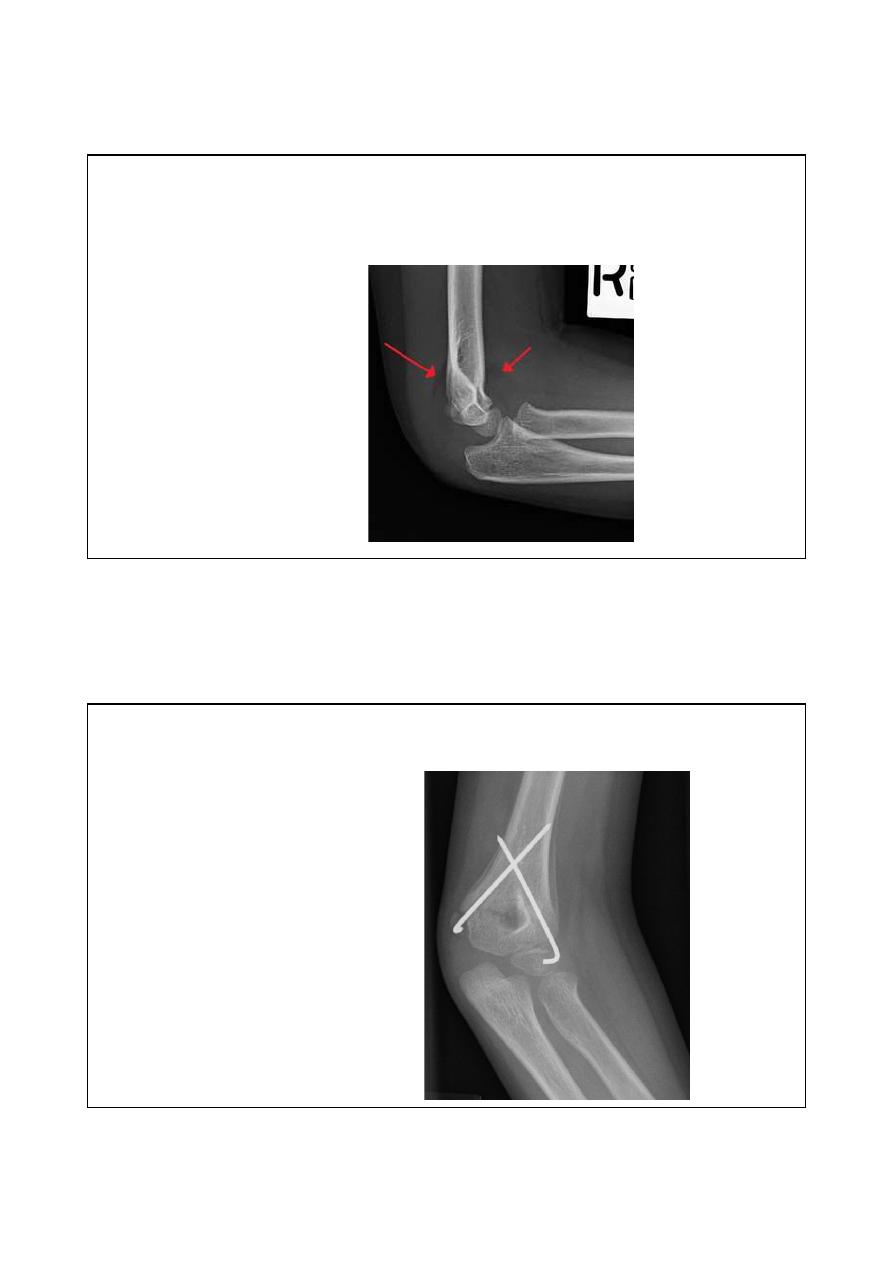
X-ray
Undisplaced fracture : fat bad sign
Treatment
Type-I : backslap for 3 weeks
followed by physiotherapy.
Type-II: reduction under general
anesthesia by following steps 1.
traction for 3 minutes 2.
correction of sideway shift 3.
gradual flexion of the elbow to
120 degree.; failure of closed
reduction is indication for open
reduction and fixation.
Type-3: open reduction and
fixation by crossed k- wires
٠٤٤١/٢٠/٢١
complications
Early
1. Vascular injury ( brachial artery): 5%
2. Nerve injury: anterior interosseous
branch of median nerve.
Late
1. Maleunion (cubitus Varus deformity):
treated by supracondylar osteotomy.
2. Elbow stiffness: treated by physiotherapy.