Fifth Stage
Internal Medicine
Dr. Abbas / Lec . 4
1
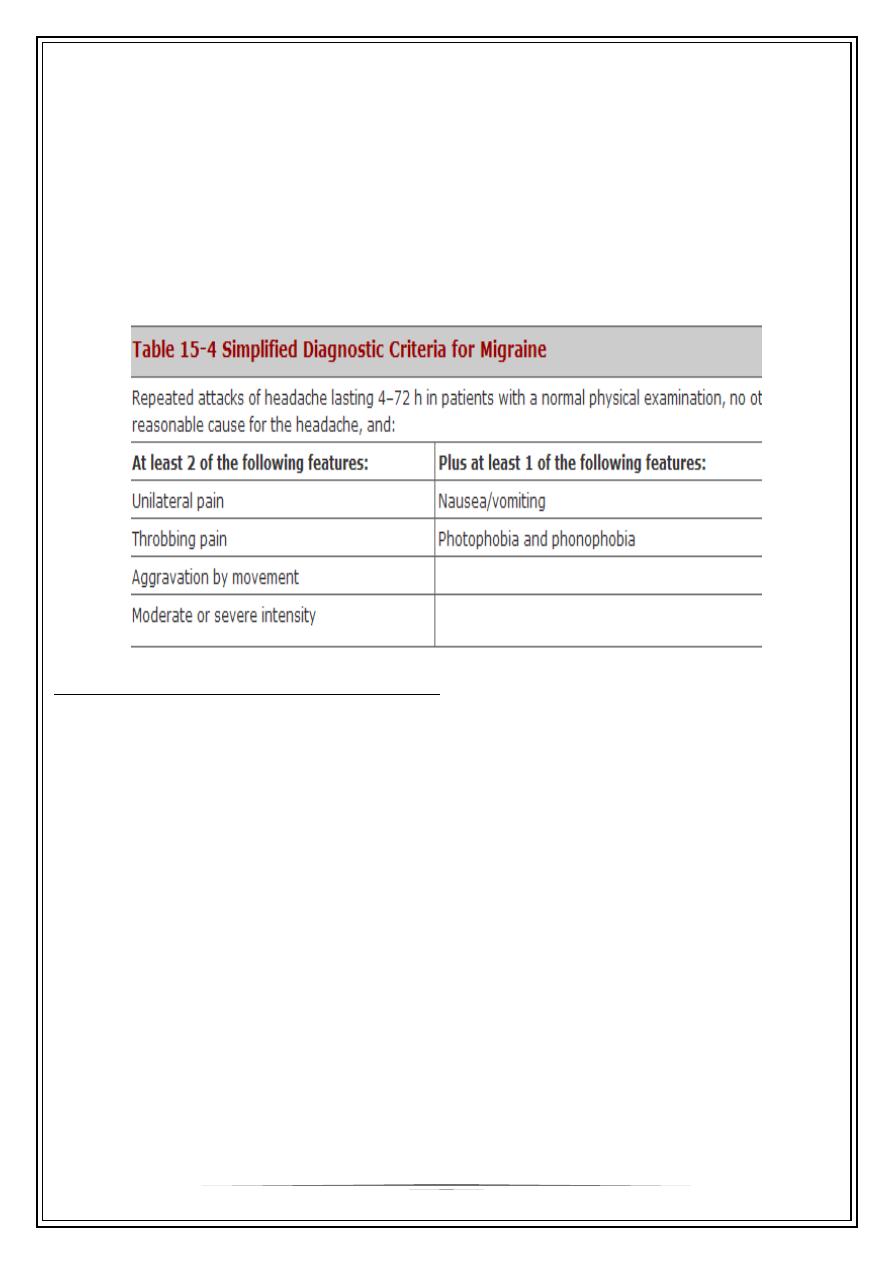
Migraine
Migraine is recurrent headache associated with visual and gastrointestinal
disturbance. The borderline between migraine and tension headaches is vague. Over
12% of any population world-wide report these symptoms
The prevalence of migraine is about 20% in women and 6% in men. All varieties of
migraine may begin at any age from early childhood on, although peak ages at onset
are adolescence and early adulthood
The term migraine is derived from the Greek word hemikrania. This term was
corrupted into low Latin as hemigranea, which eventually was accepted by the French
translation as migraine..
Mechanisms
1- Precise mechanisms of migraine remain unknown.
Genetic factors play some part - a rare form of familial migraine is associated with
mutation chromosome 19.
2- The release of the neuropeptide calcitonin-gene-related peptide (CGRP) is thought
to play a central role as it is a potent dilator of cerebral and dural vessels
3- The headache of migraine, often throbbing, is due to vasodilatation or oedema of
blood vessels, with stimulation of nearby nerve endings.
4- Release of vasoactive substances such as nitric oxide has a role
5- Serum 5-hydroxytryptamine rises with prodromal symptoms and falls during the
headache.
6- Cerebral features, such as tingling limbs, aphasia and weakness, are caused by
focal depression of cortical function.
Some patients recognize precipitating factors
•
week-end migraine (a time of relaxation)
•
chocolate (high in phenylethylamine)
•
cheese (high in tyramine)
•
noise and irritating lights
•
with premenstrual symptoms.
2
Clinical features
Migraine is common around puberty and at the menopause and sometimes
increases in severity or frequency with hormonal contraceptives, in pregnancy and with
the onset of hypertension. There is no reason to suppose that the development of
migraine is suggestive of any serious intracranial lesion. However, since migraine is so
common, an intracranial mass and migraine sometimes occur together by coincidence.
Migraine sometimes follows a blow to the head - often minor.
Migraine with aura (classical migraine)
Prodromal symptoms are usually visual and related to depression of visual cortical
function or retinal function. Unilateral patchy scotomata (retina), hemianopic
symptoms (cortex), teichopsia (flashes) and fortification spectra (jagged lines
resembling battlements) are common.
Transient aphasia sometimes occurs, with tingling, numbness, vague weakness of
one side and nausea.
The prodrome persists for a few minutes to about an hour. Headache then follows.
This is occasionally hemicranial (i.e. splitting the head) but often begins locally
and becomes generalized. Nausea increases and vomiting follows. The patient is
irritable and prefers a darkened room. Superficial temporal arteries are engorged
and pulsating. After several hours the migraine settles, sometimes with a diuresis.
Deep sleep often ensues.
3
Migraine without aura (common migraine)
This is the usual variety. Prodromal visual symptoms are vague. There is recurrent
headache accompanied by nausea and malaise.
Rare types
Basilar migraine
Hemi paretic migraine
Ophthalmoplegic migraine
Facioplegic migraine
Differential diagnosis
The sudden headache may resemble meningitis or SAH.
Hemiplegic, visual and hemi sensory symptoms must be distinguished from
thromboembolic T.I.As In T.I.As maximum deficit is present immediately and
headache is unusual
Unilateral tingling or numbness may resemble sensory epilepsy (partial seizures).
In epilepsy, distinct march (progression) of symptoms is usual.
Management
General measures include:
•
reassurance and relief of anxiety
•
avoidance of dietary factors - rarely helpful.
•
Patients taking hormonal contraceptives may benefit from a brand change, or
trying without. Premenstrual migraine may respond to diuretics. Depot estrogens
are sometimes used. Severe hemi plegic symptoms are an indication for stopping
hormonal contraceptives
Treatment:
•
Treatment of an acute attack consists of simple analgesia with aspirin or
paracetamol, often combined with an antiemetic such as metoclopramide or
domperidone.
4
•
Severe attacks can be treated with one of the 'triptans' (e.g. sumatriptan), 5-HT
agonists that are potent vasoconstrictors of the extracranial arteries. These can
be administered orally, sublingually, by subcutaneous injection or by nasal spray.
•
Ergotamine preparations should be avoided since they easily lead to dependence.
This is less likely to happen with the triptans, but it can occur. Women should be
warned that the small risk of ischaemic stroke attributable to taking oral
contraception is increased if they have migraine (), especially if they also smoke.
•
Triptans should be avoided when there is vascular disease, and not overused. A
recent study has shown that an i.v. CGRP antagonist was effective in treating
severe attacks.
Prophylaxis:
•
The following are used when attacks are frequent:[more than 3-4 attacks per
month]
•
pizotifen (antihistamine and 5-HT antagonist) 0.5 mg at night for several days,
increasing to 1.5 mg (common side-effects: weight gain and drowsiness)
•
propranolol 10 mg three times daily, increasing to 40-80 mg three times daily
•
amitriptyline: 10 mg (or more) at night.
•
Sodium valproate, methysergide, SSRIs, verapamil, topiramate, nifedipine and
naproxen are also used
Complications of Migraine
•
Include chronic migraine, migraine-triggered seizures, migrainous infarction
(stroke with migraine), and persistent aura (eg, 30-60 minutes) without infarction.
•
Ischemic stroke may occur as a rare but serious complication of migraine.
•
In migraines with aura, the risk for hemorrhagic stroke may be possible, but rare.
•
Risk factors for stroke include migraine with aura, female sex, cigarette smoking,
and estrogen use.
Cluster headache (migrainous neuralgia)
This is some less common than migraine. There is a 5:1 predominance of males
and onset is usually in the third decade. The characteristic syndrome comprises
5
periodic, severe, unilateral peri-orbital pain accompanied by unilateral lacrimation, nasal
congestion and conjunctiva injection, often with the other features of Horner's
syndrome.
The pain, whilst being very severe, is characteristically brief (30-90 minutes).
Typically, the patient develops these symptoms at a particular time of day (often in the
early hours of the morning). The syndrome may occur repeatedly for a number of
weeks, followed by a respite for a number of months before another cluster occurs
Despite intense pain there are no serious squeal. Attacks recur at intervals over
several years but tend to disappear after the age of 55. Analgesics are unhelpful.
Subcutaneous sumatriptan is the drug of choice. Alternatively oxygen inhalation 7.12
L/min may abort an attack. Most prophylactic migraine drugs are unhelpful. Verapamil,
topiramate and lithium carbonate sometimes prevent 'cluster'
Trigeminal neuralgia
•
Trigeminal neuralgia (tic douloureux) is of unknown cause, seen most commonly
in old age.
•
It is almost always unilateral. Symptoms Severe paroxysms of knife-like or electric
shock-like pain, lasting seconds, occur in the distribution of the fifth nerve.
•
Spasms occur many times a day. Each paroxysm is stereotyped, brought on by
stimulation of one or more trigger zones in the face. Washing, shaving, a cold
wind or eating are examples of trivial stimuli that provoke pain. The face may be
screwed up in agony (hence the term tic).
•
Pain characteristically does not occur at night. Spontaneous remissions last
months or years before recurrence, which is almost inevitable.
•
Signs There are no signs of trigeminal nerve dysfunction. The corneal reflex is
preserved. The history alone make the diagnosis.
•
Treatment The anticonvulsant carbamazepine 600-1200 mg daily reduces severity
of attacks in the majority. Phenytoin, gabapentin and clonazepam are used, but
are less effective. If drug therapy fails, surgical procedures (radiofrequency
extirpation of the ganglion, neurovascular decompression or sectioning of the
sensory root) are useful. Alcohol injection into the trigeminal ganglion or
peripheral fifth nerve branches can also be carried out.
Thank you,,,