Fifth Stage
Internal Medicine
Dr. Abbas / Lec . 5
1
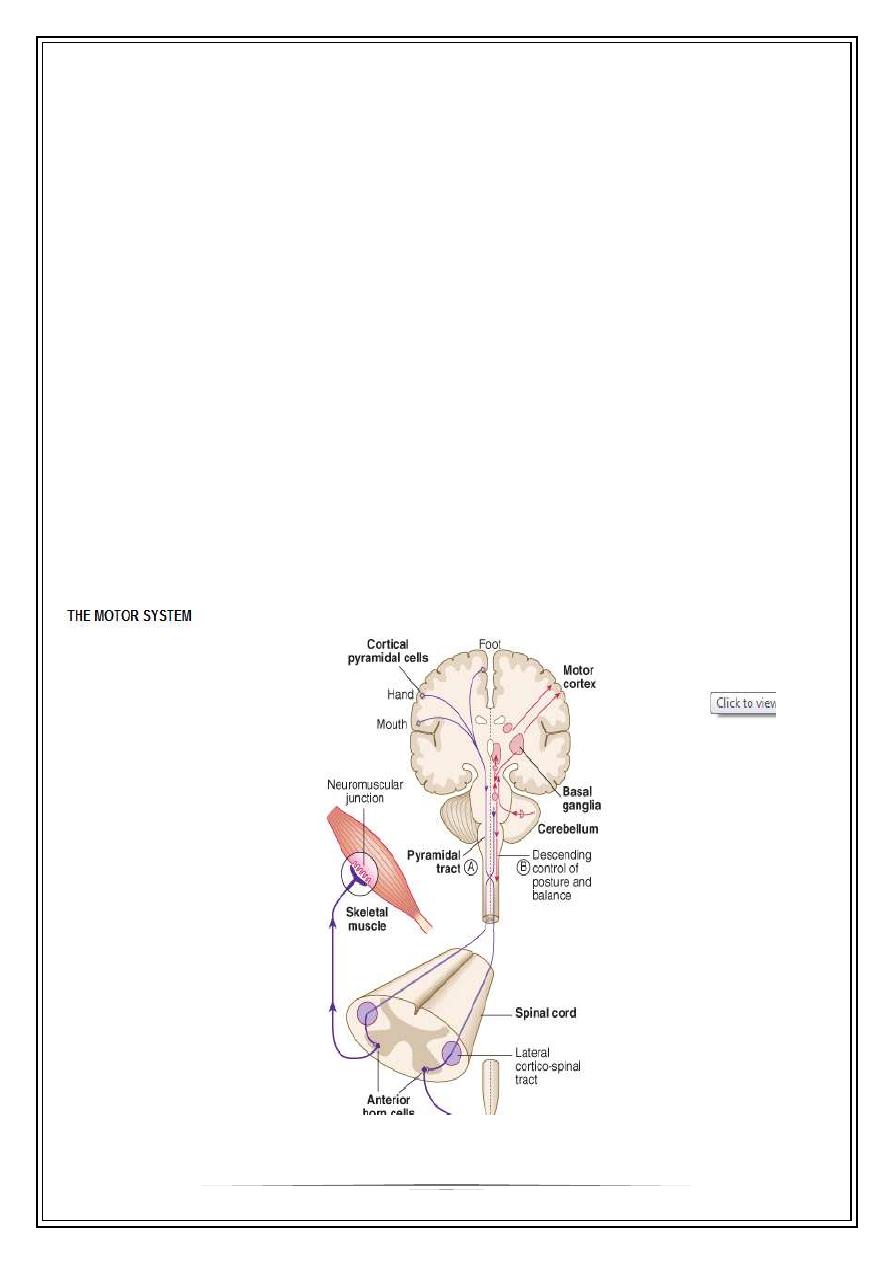
Motor Control Systems
CORTICOSPINAL OR PYRAMIDAL SYSTEM
The corticospinal tracts originate in neurones of the fifth cortical layer and terminate
at motor nuclei of cranial nerves or at the lower border of L1 in spinal cord [anterior
horn cells]. The nerve pathways of particular clinical significance) congregate in the
internal capsule and cross in the medulla (decussation of the pyramids), passing to
the contralateral halves of the spinal cord as the lateral corticospinal tracts. This is
the pyramidal system, disease of which causes upper motor neuron (UMN) lesions
This system enables purposive, skilled, strong and organized movement to take
place. Defective function is recognized by a distinct pattern of loss of skilled
voluntary movement, spasticity and reflex change. This is seen, for example, in a
hemi paresis or hemiplegic
2
1-pyramidal drift
Normally, the outstretched upper limbs are held symmetrically, even when the eyes
are closed. With a pyramidal (UMN) lesion, when both upper limbs are held
outstretched, palms uppermost, the affected limb drifts downwards and medially.
The forearm tends to pronate and the fingers flex slightly. This sign is often first to
occur, sometimes before weakness or reflex changes become obvious
2-Weakness and loss of skilled movement
unilateral pyramidal (UMN) lesion above the decussating in the medulla (e.g. an
internal capsule infarct) causes weakness of the opposite limbs, i.e. contra lateral
hemi paresis.. In the upper limb flexors remain stronger than extensors, while in the
lower limb extensors remain stronger than flexors. In addition to weakness, there is
loss of skilled movement. For example, fine finger and toe control diminishes. Muscle
wasting (except from disuse) is not a feature of pyramidal lesions. Muscles remain
normally excitable electrically.
3-Increase in tone [spasticity ]
acute lesion of one pyramidal tract (e.g. the internal capsule stroke) causes initially
flaccid paralysis, and loss of tendon reflexes.
Increase in tone follows within several days owing to loss of the inhibitory effect of
the corticospinal pathways and an increase in spinal reflex activity. The pattern is
characterized by changing resistance to passive movement - the sudden clasp-knife
effect. The relevant tendon reflexes become exaggerated and clonus evident.
4-Changes in superficial reflexes
The normal flexor plantar response becomes extensor (a positive Babinski). The
stimulus should be unpleasant (an orange-stick is the correct instrument). An
extensor plantar is certain when dorsiflexion of the great toe is accompanied by
fanning (abduction) of adjacent toes. Abdominal (and cremasteric reflexes) are
abolished on the affected side.
3
EXTRAPYRAMIDAL SYSTEM
The extrapyramidal system facilitates fast, fluid movements that the corticospinal
system has generated. Defective function is recognized usually by slowness
(bradykinesia), stiffness (rigidity) and/or disorders of movement (rest tremor, chorea
and other dyskinesias). Frequently, one sign (e.g. stiffness, tremor or chorea) will
predominate.
The extrapyramidal system is a general term without an absolute definition for motor
structures of the basal ganglia, i.e. corpus striatum (caudate nucleus + globus
pallidus + putamen), subthalamic nucleus, substantia nigra and parts of the
thalamus.
In basal ganglia/extrapyramidal disorders, either or both of two features become
apparent in the limbs and axial muscles:
reduction in speed, known as bradykinesia (slow movement) or akinesia (no
movement), with muscle rigidity
involuntary movements (e.g. tremor, chorea, hemiballismus, athetosis, dystonia).
Lesions of the extrapyramidal system produce an increase in tone, which is not an
exaggerated response to stretch but is continuous throughout the range of
movement at any speed of stretch ('lead pipe' rigidity). Involuntary movements are
also a feature of extrapyramidal lesions
tremor combined with rigidity produces typical 'cogwheel' rigidity.
Rapid movements are slowed and clumsy (bradykinesia).
Extrapyramidal lesions also cause postural instability, precipitating falls.
Chorea, athetosis, ballism and dystonia
Jerky, small-amplitude, purposeless involuntary movements are termed 'chorea' (the
Greek for 'dance').; they suggest disease in the caudate nucleus
More dramatic ballistic movements of the limbs usually occur unilaterally
(hemiballismus) in vascular lesions of the subthalamic structures.
Slower writhing movements of the limbs are called athetosis. These are often
combined with chorea (and have a similar list of causes) and are then termed
'choreo-athetoid' movements.
4
CEREBELLUM
The cerebellum and its connections have a role in coordinating smooth movement
initiated by the corticospinal system, and in the regulation of balance.
Cerebellar lesions
Expanding mass lesions within the cerebellum
1. obstruct the aqueduct to cause hydrocephalus, with severe pressure headaches,
vomiting and papilloedema.
2. Coning of the cerebellar tonsils) through the foramen magnum and respiratory
arrest occur, often within hours. Rarely,
3. tonic seizures (sudden attacks of limb stiffness) occur.
Lateral cerebellar lobes lesions
1-causes disruption of the normal sequence of movements (dyssynergia) on the
same side
2-The outstretched arm is held still in the early stages of a cerebellar lesion (cf. the
drift of a pyramidal lesion) but there is rebound upward overshoot when the limb is
pressed downwards and released.
3-Gait becomes broad and ataxic; the patient falters towards the lesion, tremor and
ataxia.
4-Movement is imprecise in direction, in force and in distance (dysmetria). Rapid
alternating movements (tapping, clapping or rotary hand movements) are clumsy
and disorganized (dysdiadochokinesis). Intention tremor (action tremor, with past-
pointing) is seen. Speed of movement is preserved, cf. extrapyramidal disease
5-Nystagmus: Coarse horizontal nystagmus develops with lateral cerebellar lobe
lesions - the fast component towards the lesion.
6-Dysarthria: A halting, jerking dysarthria occurs - the scanning speech of cerebellar
lesions (usually bilateral).
Other signs
Titubation - rhythmic head tremor in either to and fro ('yes-yes') movements or
rotary ('no-no') movements - also occurs,
5
Hypotonia (floppy limbs) and depression of reflexes (and slow, pendular reflexes) are
also sometimes seen with cerebellar disease
Midline cerebellar lesions
Midline cerebellar vermis lesions have a dramatic effect on trunk and axial
musculature-difficulty standing and sitting unsupported, with a rolling, broad, ataxic
gait (truncal ataxia).
The LMN is the motor pathway from anterior horn cell (or cranial nerve nucleus) via
peripheral nerve to motor endplate
Signs of a lower motor neurone lesion
1) Weakness
2) Wasting
3) Hypotonia
4) Reflex loss
5) Fasciculation
long term effects:
6) Contractures of muscle
7) Trophic changes in skin and nails
Signs of lower motor neurone lesion
These are seen in voluntary muscles, which depend upon an intact nerve supply to
produce movement and for metabolic integrity. Signs follow rapidly if the LMN is
interrupted (). Muscle wasting appears within 3 weeks. Fasciculation (visible
twitching) occurs - due to contractions of denervated single motor units. Fibrillation
potentials are seen when denervated muscle is sampled electrically
Thank you,,,