د.اشرف مزاحم الشاكر
lec. : 1
1
There are six main salivary glands,
two sublingual glands, two submandibular glands and
two parotid glands. In addition, there are multiple minor salivary glands.
SALIVA
_ 1500 ml of saliva is secreted per day. pH of resting saliva is less, 7.0; active saliva is 8.0.
_ Saliva contains lingual lipase secreted from tongue glands, α amylase from salivary glands.
_ Saliva contains mucin, glycoproteins, immunoglobulin IgA, lysozyme, lactoferrin which
binds iron; proline rich proteins that protect enamel and bind toxic tannins.
_ Parotid saliva is 20% of total secretion of saliva per day and is serous and watery;
submandibular is 70% and is mucous and moderately viscous; sublingual is 5% and is
mucous and viscous. Minor salivary and other oral glands—5%.
_ Saliva facilitates swallowing, keeps mouth moist, serves as solvent for taste buds,
facilitates speech, keeps oral cavity rinsed and clean, antibacterial, and neutralizes gastric
acid content in regurgitation to relieve heartburn.
Anatomy
The mucosa of the oral cavity contains approximately 450 minor salivary glands. They are
distributed in the mucosa of the lips, cheeks, palate, floor of the mouth and retromolar area.
These minor salivary glands also appear in other areas of the upper aerodigestive tract
including the oropharynx, larynx and trachea as well as the sinuses. They have a histological
structure similar to that of mucous-secreting major salivary glands. Overall, they contribute
to 10 per cent of the total salivary volume (Summary box 50.1).
Common disorders of minor salivary glands
Cysts
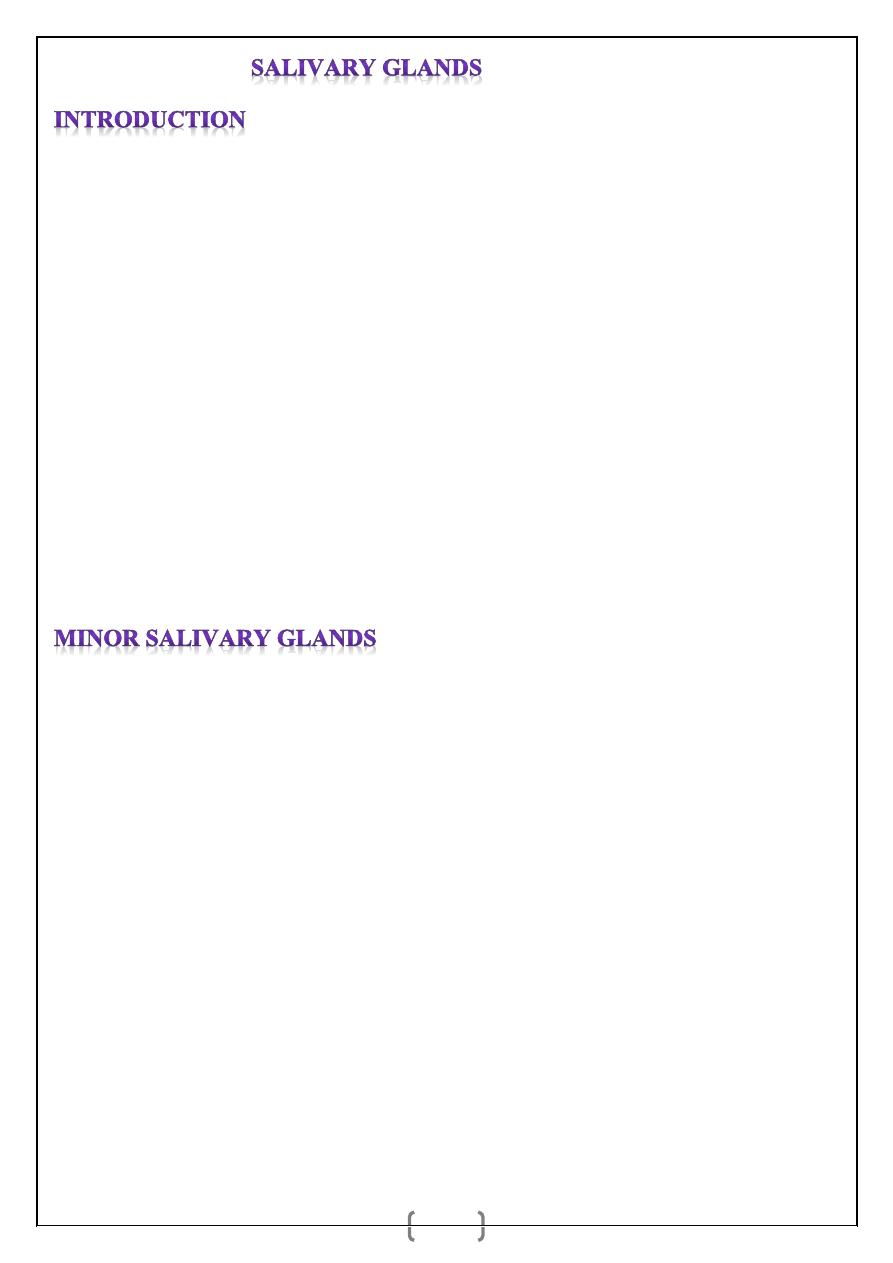
Extravasation cysts are common and result from trauma to the overlying mucosa. They
usually affect minor salivary glands within the lower lip, producing a variable swelling that
is painless and usually, but not always, translucent (Figure 50.1). Some resolve
spontaneously, but most require formal surgical excision that includes the overlying mucosa
and the underlying minor salivary gland. Recurrence is rare.
د.اشرف مزاحم الشاكر
lec. : 1
2
(
Figure 1
)
Mucous retention cyst. A translucent swelling on the lower
Lip is typical
.
Tumours
Tumours of minor salivary glands are histologically similar to those of major glands;
however, up to 90 per cent of minor salivary gland tumours are malignant. Although
tumours of minor salivary gland origin occur anywhere in the upper aerodigestive tract,
common sites for tumour formation include the upper lip, palate and retromolar regions. Less
common sites for minor salivary gland tumours include the nasal and pharyngeal cavities.
Minor salivary gland tumours have also been reported in the paranasal sinuses and
throughout the pharynx. These tumours arise in submucosal seromucous glands that are
found throughout the upper aerodigestive tract. Very rarely, a mucoepidermoid carcinoma
can present as an intraosseous tumour of the mandible.
Clinical feature:
Malignant minor salivary gland tumours are rare. They have a firm consistency, and the
overlying mucosa may have a varied discolouration from pink to blue or black. The tumour
may become necrotic with ulceration as a late presentation.
Treatment:
Malignant minor salivary gland tumours of the palate are managed by wide excision which
may involve partial or total maxillectomy. The subsequent defect can be managed by either
prosthetic obturation or immediate reconstruction. Various microvascular flaps have been
designed to reconstruct maxillectomy defects, including radial forearm flap, fibular flap,
rectus abdominus, latissimus dorsi and the vascularised iliac crest graft.
د.اشرف مزاحم الشاكر
lec. : 1
3
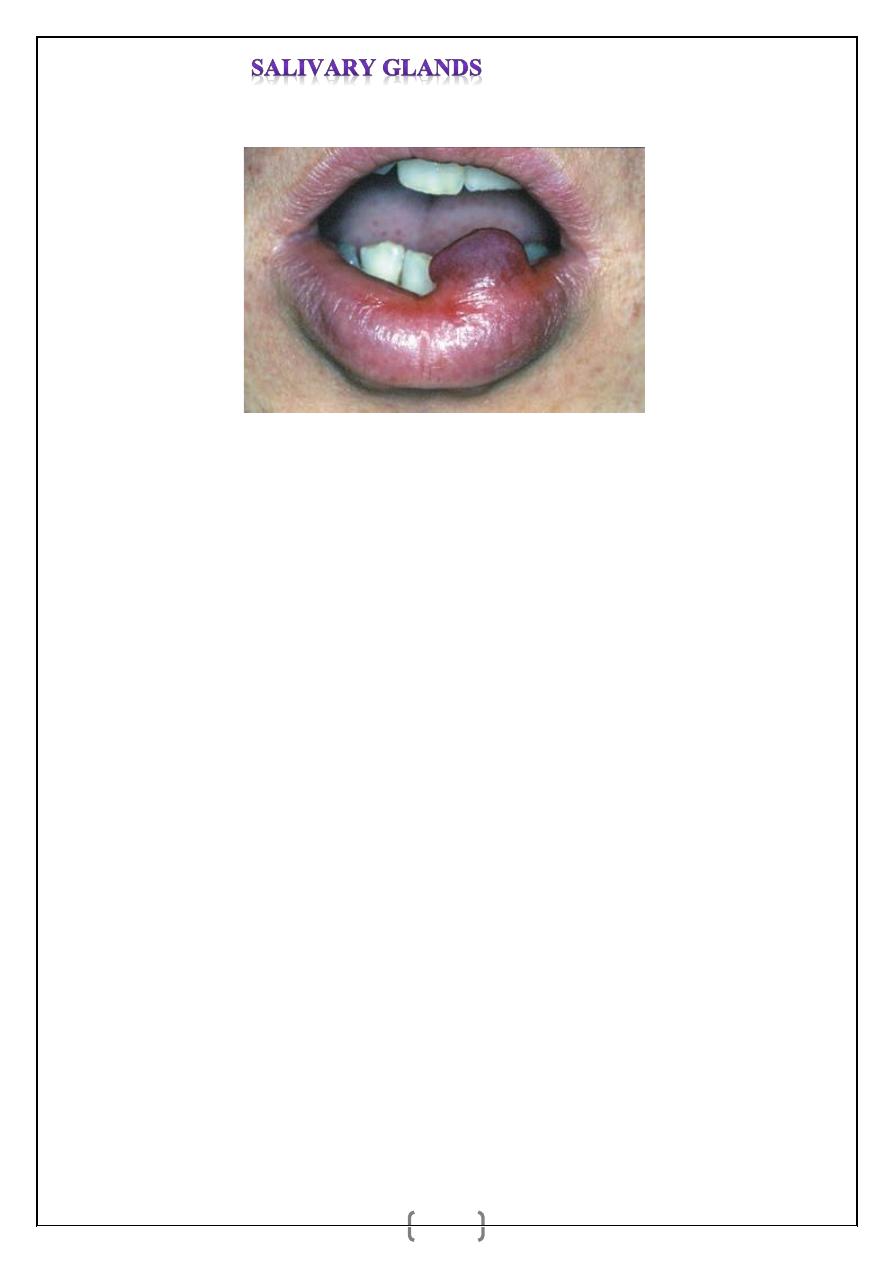
Benign minor salivary gland tumours (10%) present as painless, firm, slow-growing
swellings. Overlying ulceration is extremely rare. Minor salivary gland tumours of the upper
lip are managed by excision to include the overlying mucosa, with primary closure. Benign
tumours of the palate, less than 1 cm in diameter, can be managed by excisional biopsy, and
the defect is allowed to heal by secondary intention. Where tumours of the palate are greater
than 1 cm in diameter, incisional biopsy is recommended to establish a diagnosis prior to
formal excision.
Figure 2
(a) Pleomorphic adenoma of the upper lip. (b) Tumour excised with overlying mucosa. (c) Primary closure of
the defect.
Figure 3
(a) Pleomorphic adenoma in the right palate in a 12-yearold girl. (b) Tumour marked out with adequate
margins including the overlying mucosa. (c) The subsequent defect. (d) Healing by secondary intention three years
after surgery.
Anatomy
The sublingual glands are a paired set of minor salivary glands lying in the anterior part of
the floor of mouth between the mucous membrane, the mylohyoid muscle and the body of
the mandible close to the mental symphysis. Each gland has numerous excretory ducts that
open either directly into the oral cavity
or indirectly via ducts that drain into the
submandibular duct.
a
b
c
a
b
c
د.اشرف مزاحم الشاكر
lec. : 1
4
Common disorders of the sublingual glands:
1. Ranula
: mentioned in the previous lecture
2. SUBLINGUAL DERMOIDS: mentioned in the previous lecture
3. Tumours
:
Tumours involving the sublingual gland are extremely rare and are usually (85 per cent)
malignant. They present as a hard or firm painless swelling in the floor of the mouth.
Treatment requires wide excision involving the overlying mucosa and simultaneous neck
dissection. Immediate reconstruction of the intraoral defect is recommended using, for
example, a radial artery forearm flap.
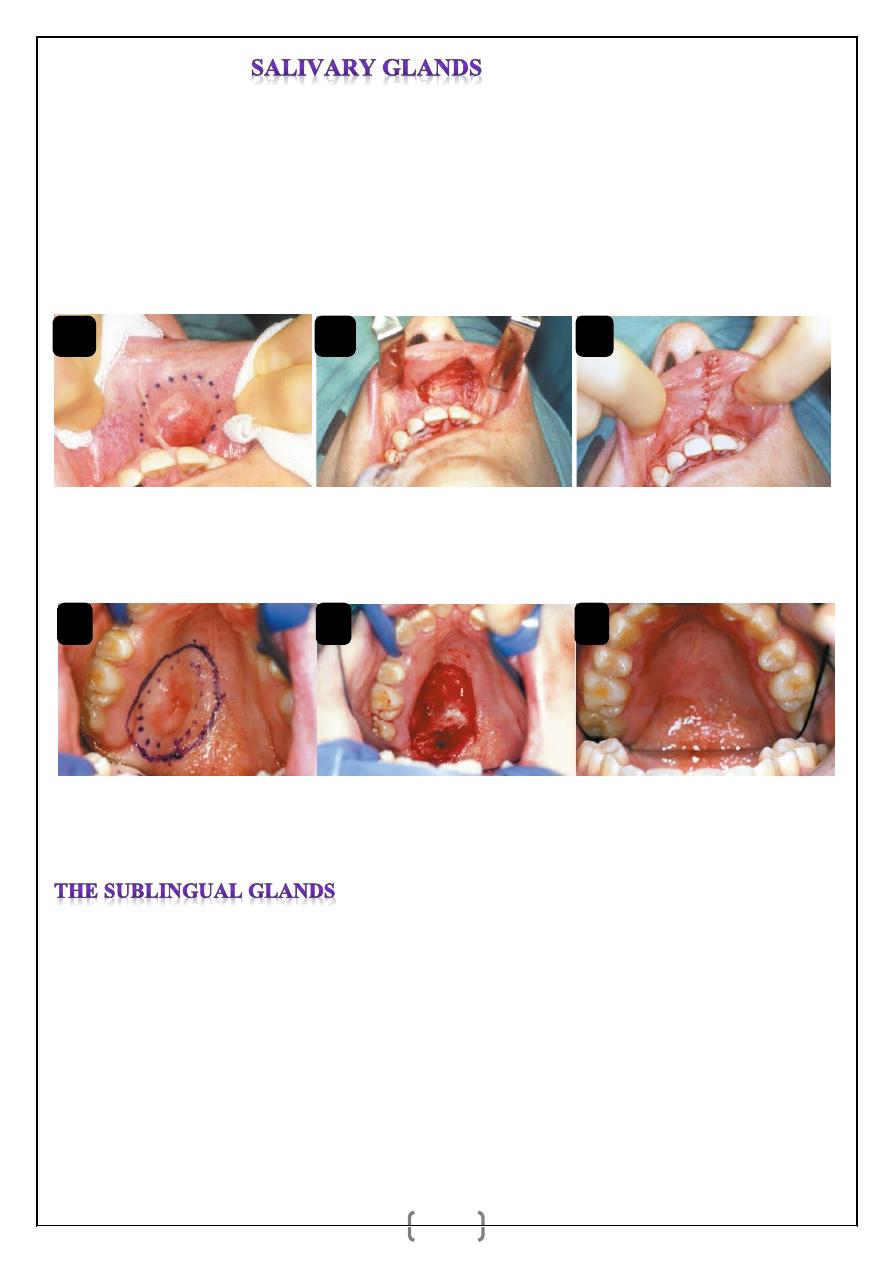
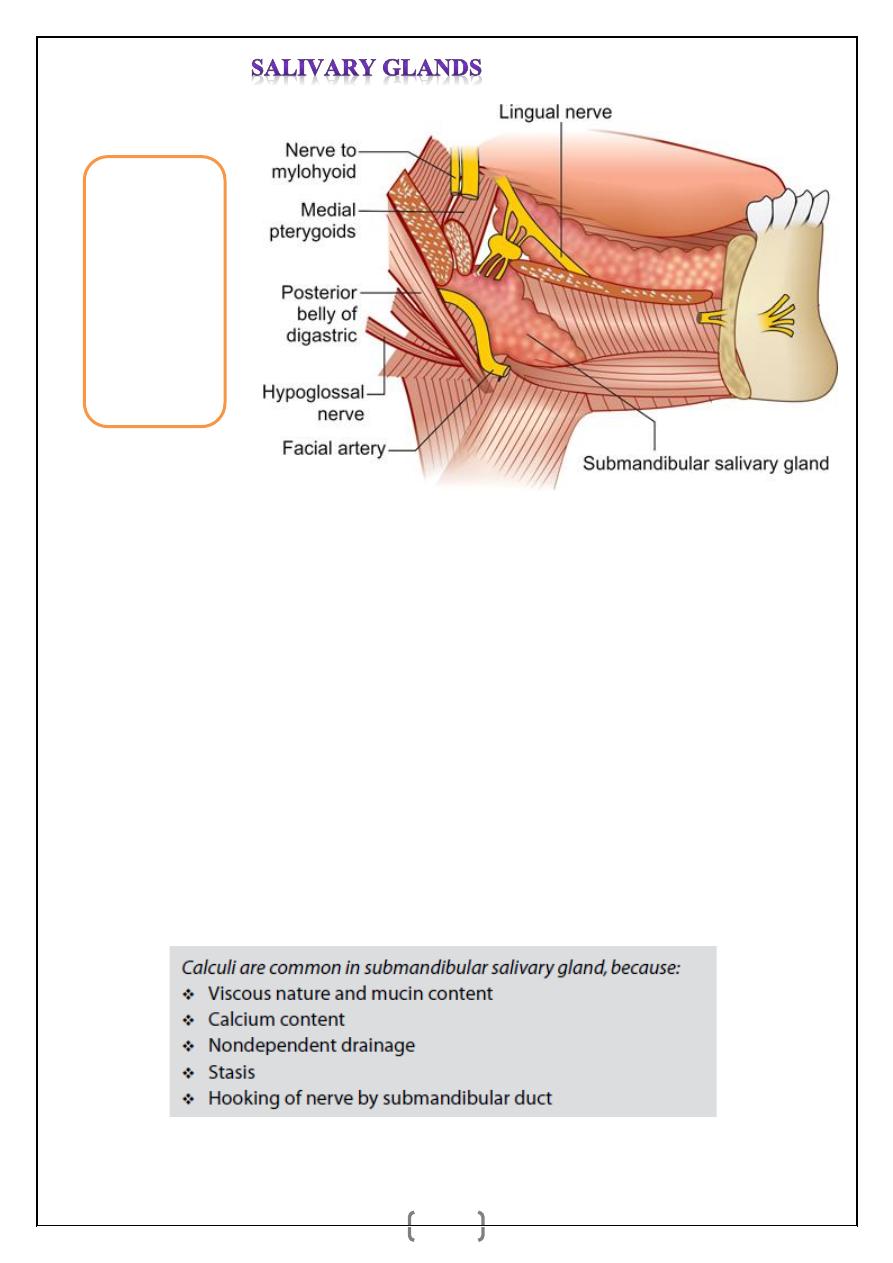
It is a ‘J’ shaped salivary gland situated in the anterior part of the digastric triangle.
Parts
_ Superficial part: Lies in submandibular triangle, superficial to mylohyoid and hyoglossus
muscles, between the two bellies of digastric muscle.
_ Deep part is in the floor of the mouth and deep to the mylohyoid.
Submandibular (Wharton’s) duct (5 cm), emerges from the anterior end of the deep part of
the gland, enters the floor of the mouth, on the summit of papilla beside the frenulum of the
tongue. Lingual nerve and submandibular ganglion are attached to upper pole of the gland.
Hypoglossal nerve is deep to the gland. Facial artery emerges from under surface of the
stylohyoid muscle, enters the gland from posterior and deep surface, reaching its lateral
surface crossing the lower border of mandible to enter the face. Venous drainage is to
anterior facial vein. Nerve supply: Branches from the submandibular ganglion. Resting
salivary flow usually arises from the submandibular salivary gland.
د.اشرف مزاحم الشاكر
lec. : 1
5
Sialorrhoea
: is increased salivary flow often seen due to drugs, in cerebral palsy, physically
handicapped person, children, and psychiatry patients. Intractable sialorrhoea can be
corrected by different surgeries to submandibular salivary gland like duct repositioning to
excision of the gland.
Xerostomia:
is decreased salivary flow. It is seen in postmenopausal women, depression,
dehydration, use of antidepressant drugs; anticholinergic drugs, Sjogren’s syndrome,
radiotherapy to head and neck region.
SALIVARY CALCULUS AND SIALADENITIS
_ 80% Submandibular, 80% Radio-opaque, It is commonly calcium phosphate and calcium
carbonate stones. Calculi are more common in submandibular gland, because the gland
secretion is viscous, contains more calcium and also, its drainage is nondependent, causing
stasis.
_ Secretion from parotid is serous, contains less calcium and so stones are not common.
Fig. 7:
Anatomical
relations of the
submandibular
salivary gland
د.اشرف مزاحم الشاكر
lec. : 1
6
Presentation
Acute Sialadenitis—Features
_ Pain, swelling, tenderness is seen in submandibular region and floor of the mouth,
Dysphagia, trismus, fever. Double chin appearance due to spreading of oedema downwards.
Duct is inflamed and swollen.
Chronic Sialadenitis—Features
_ Pain is more during mastication due to stimulation (Salivary colic which can be induced by
meals, lemon juice, etc.). Salivary colic is pain induced by obstruction to the outflow of
saliva may be ductal stone. During salivation size of the swelling will decrease again 2 hours
after meal/stimulation. Salivary secretion is more during mastication causing increase in
gland size. Firm/rubbery tender swelling is palpable bidigitally.
_ when stone is in the duct, it is palpable in the floor of the mouth as a tender swelling with
features of inflammation in the duct. Pus exudes through the duct orifice. (Irritation of the
lingual nerve, which is in very close proximity to submandibular salivary duct, causes
referred pain to tongue—lingual colic). In submandibular salivary gland, often the stones are
multiple, with chronic inflammation of gland (sialadenitis). Often acute on chronic
sialadenitis can occur. Kuttner tumour is chronic sclerosing sialadenitis of submandibular
salivary gland.
Investigations
_ Intraoral X-ray (dental occlusion films) to see radiopaque stones (80%).
_ FNAC of the gland to rule out other pathology.
_ Total count and ESR in acute phase.
_ USG will demonstrate stone with posterior acoustic shadow.
Note:
Radiological demonstration of stone/stones is called as Sialolithiasis.
Treatment
_ If the stone is in the duct, removal of the stone is done intraorally, by making an incision in
the duct. Incised duct is not sutured as it may result in stricture. Laying open allows free
drainage of saliva. Procedure is usually done under local anaesthesia.
_If stone is in the gland, excision of submandibular gland is done—sialadenectomy. It is
always done under general anaesthesia.
د.اشرف مزاحم الشاكر
lec. : 1
7
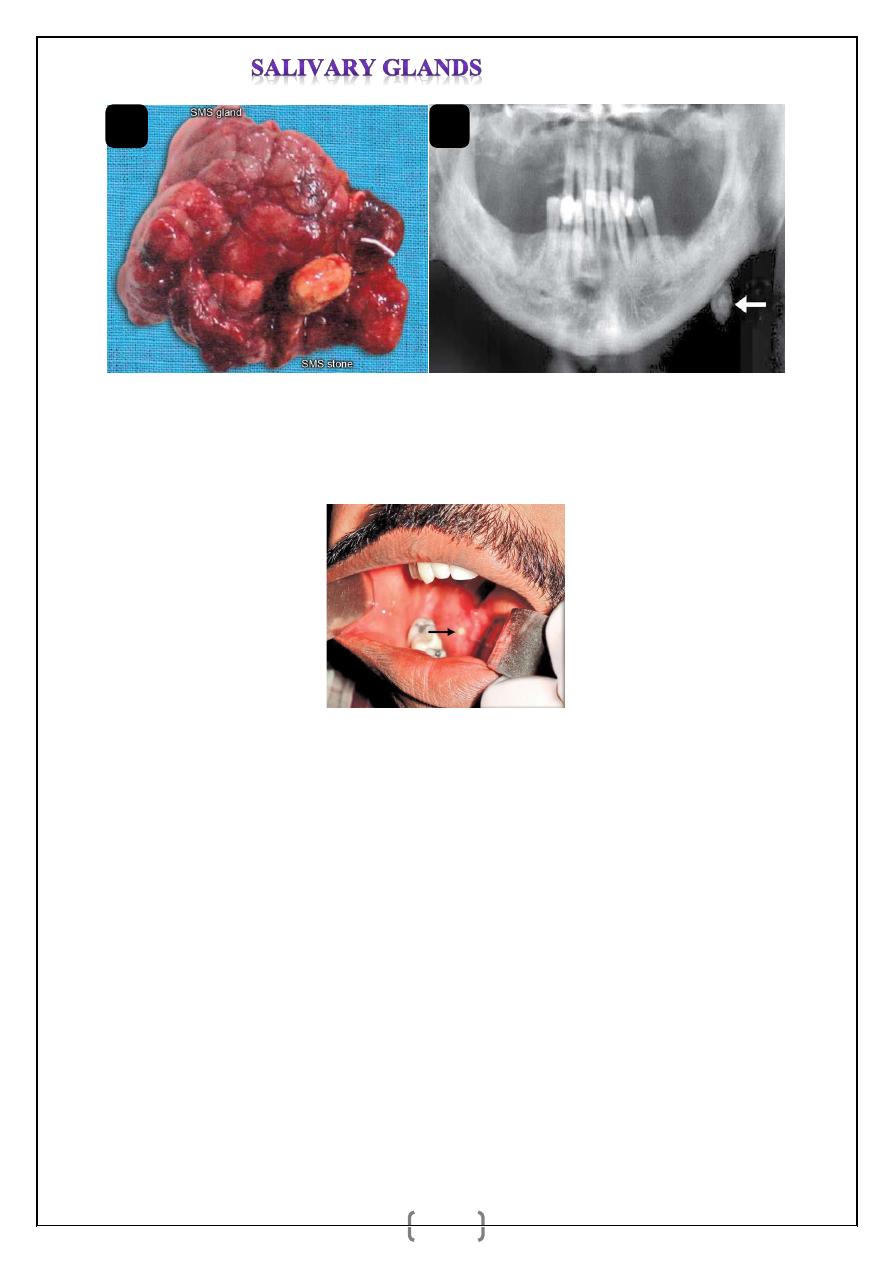
Fig. 8.a and b: a. Excised specimen of submandibular salivary gland with stone in the gland.
b. X-ray (OPG) showing left sided submandibular salivary stone.
Fig. 9: Stone in the duct of submandibular salivary gland (Wharton’s duct).
Complications of Surgery
1. Hemorrhage.
2. Infection.
3. Injury to marginal mandibular nerve, lingual nerve, hypoglossal nerve.
4. Injury to nerve to mylohyoid causing anaesthesia over submental skin.
a
b