د.اشرف مزاحم الشاكر
lec. : 2
1
Tumours of the submandibular gland
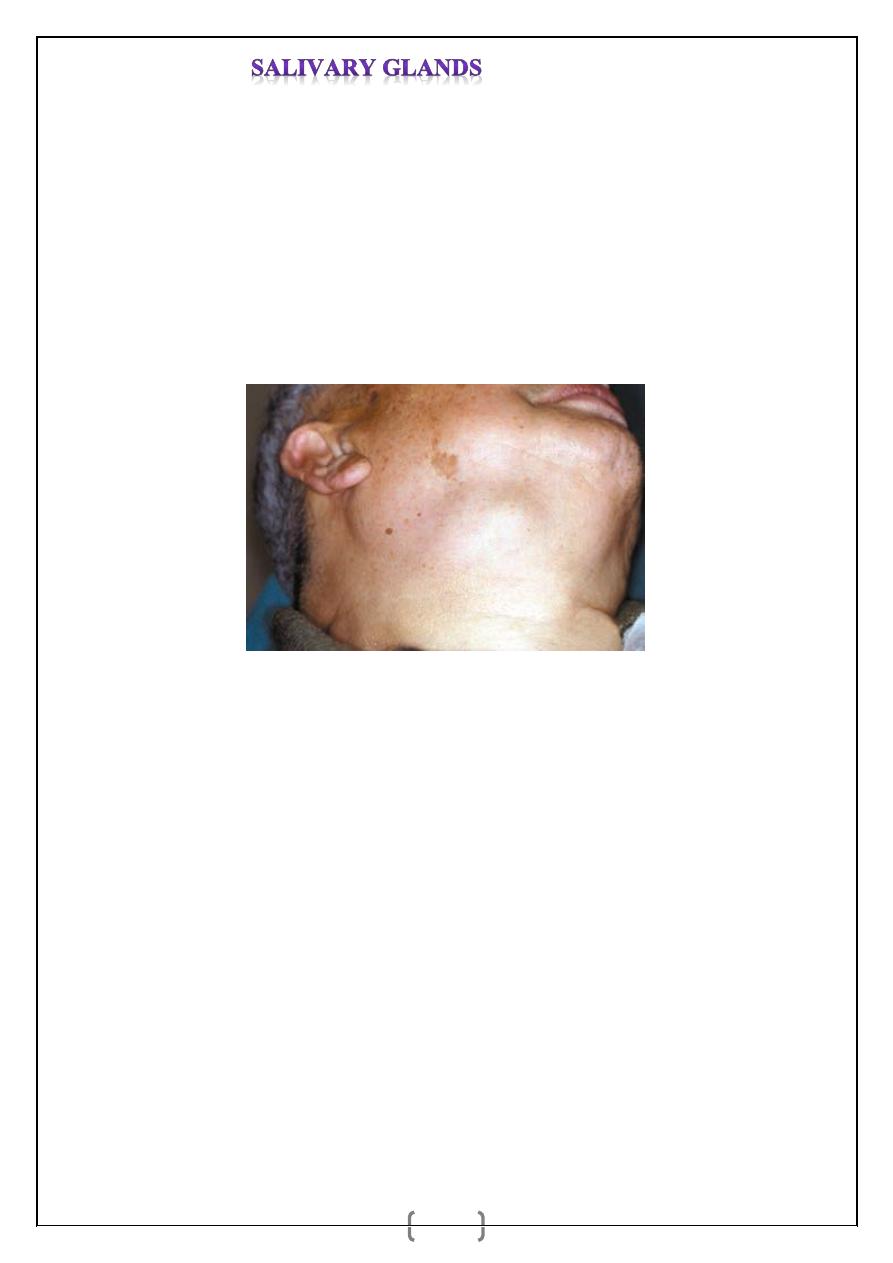
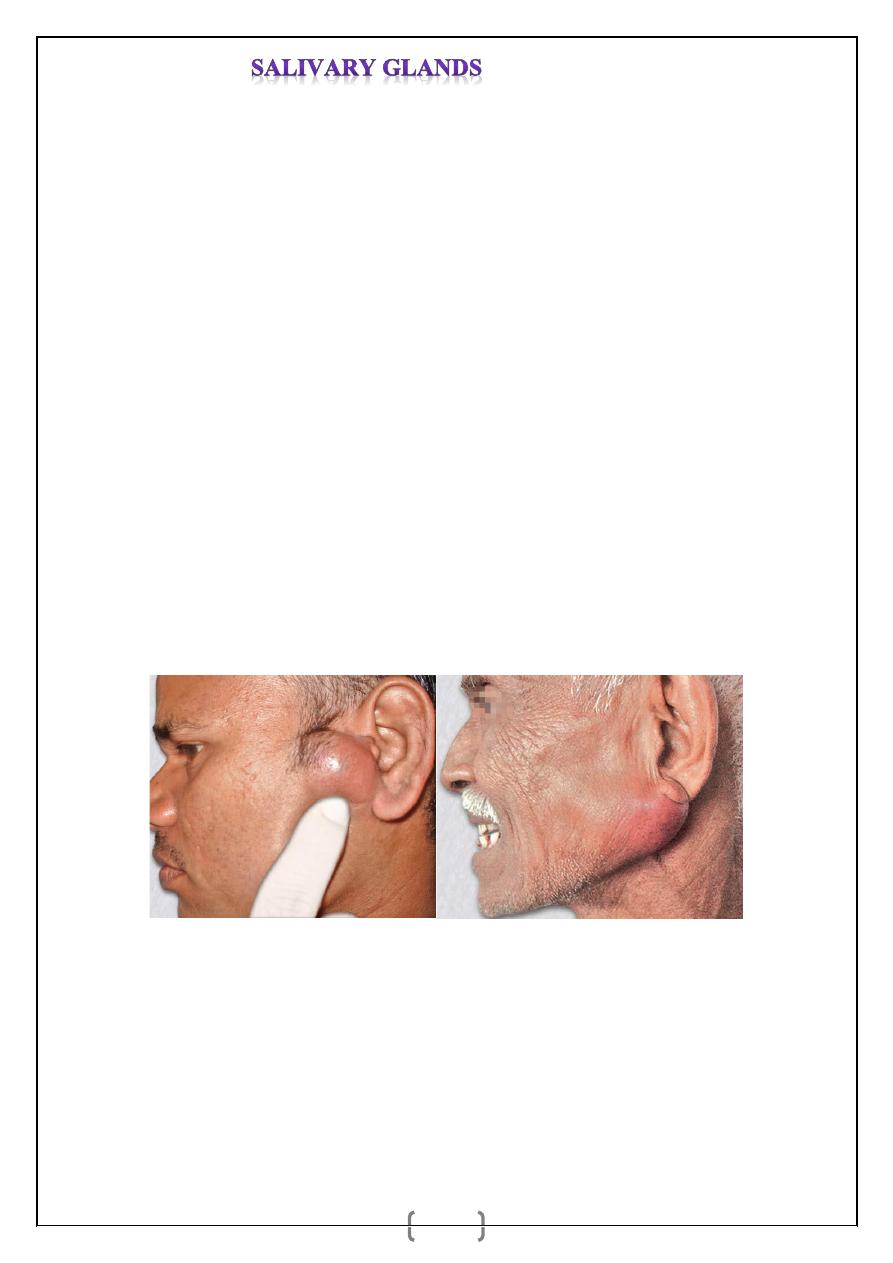
Tumours of the submandibular gland are uncommon and usually present as a slow-growing,
painless swelling within the submandibular triangle (Figure1). Only 50 per cent of
submandibular gland tumours are benign, in contrast to 80–90 per cent of parotid gland
tumours. In many circumstances, the swelling cannot, on clinical examination, be
differentiated from submandibular lymphadenopathy. Most salivary neoplasms, even
malignant tumours, are often slow growing, painless swellings. Unfortunately, pain is not a
reliable indication of malignancy as benign tumours often present with pain in the affected
gland, presumably due to capsular distension or outflow obstruction.
Figure1 Benign tumour of the right submandibular gland.
Clinical features of malignant salivary tumours
These include:
• facial nerve weakness
• rapid enlargement of the swelling
• induration and/or ulceration of the overlying skin
• cervical node enlargement.
Investigation
Computed tomography (CT) and MRI scanning are the most helpful techniques for imaging
tumours arising in the major salivary glands. The tumour is intrinsic to the gland, and its
border can be imaged to highlight whether it is circumscribed and probably benign, or
diffuse, invasive and probably malignant. The scan will highlight the relationship of the
tumour to other anatomical structures, which is helpful in planning surgery. Open surgical
biopsy is contraindicated as this may seed the tumour into surrounding tissues, making it
د.اشرف مزاحم الشاكر
lec. : 2
2
impossible to eradicate microscopic deposits of tumour cells. Fine-needle aspiration biopsy
is a safe alternative to open biopsy. There is evidence to suggest that, provided the needle
gauge does not exceed 18G, there is no risk of seeding viable tumour cells. The role of fine-
needle aspiration biopsy is, however, controversial as it rarely alters surgical management.
Management of submandibular gland tumours
As with all salivary gland tumours, surgical excision with a cuff of normal tissue is the goal.
When the tumour is small and entirely encased within the submandibular gland parenchyma,
straightforward intracapsular submandibular gland excision is appropriate. However, benign
tumours that are large and project beyond the submandibular gland are best served by
suprahyoid neck dissection, preserving the marginal mandibular branch of the facial nerve,
lingual nerve and hypoglossal nerves. This
entails a full clearance of the submandibular
triangle, involving the development of a subplatysmal skin flap, dissection of periosteum
along the lower border and inner aspect of the mandible, and delivery of the gland and
tumour with a cuff of normal tissue. In cases of overt malignancy, modified neck dissection
or radical neck dissection is appropriate. This may necessitate sacrifice of the lingual and
hypoglossal nerves if the tumour is adherent to the deep bed of the gland.
THE PAROTID GLAND
Anatomy
The parotid gland lies in a recess bounded by the ramus of the mandible, the base of the skull
and the mastoid process. It lies on the carotid sheath and the XIth and XIIth cranial nerves
and extends forward over the masseter muscle. The gland is enclosed in a sheath of dense
deep cervical fascia. Its upper pole extends just below the zygoma and its lower pole into the
neck. Several important structures run through the parotid gland.
These include:
• branches of the facial nerve;
• the terminal branch of the external carotid artery that divides into the maxillary artery and
the superficial temporal artery;
• the retromandibular vein;
• intraparotid lymph nodes.
The gland is arbitrarily divided into deep and superficial lobes, separated by the facial nerve.
Eighty per cent of the parotid gland lies superficial and 20 per cent deep to the nerve. An
accessory lobe is occasionally present lying anterior to the superficial lobe on the masseter
muscle.
د.اشرف مزاحم الشاكر
lec. : 2
3
Developmental disorders
Developmental disorders such as agenesis, duct atresia and congenital fistula are extremely
rare.
Inflammatory disorders
Viral infections
Mumps is the most common cause of acute painful parotid swelling and predominantly
affects children. It is spread via airborne droplets of infected saliva. The disease starts with a
prodromal period of 1–2 days, during which the patient experiences fever, nausea and
headache. This is followed by pain and swelling in one or both parotid glands. Parotid pain
can be very severe and exacerbated by eating and drinking. Symptoms resolve within 5–10
days. The diagnosis is based on history and clinical examination; a recent contact with an
infected patient with a painful parotid swelling is often sufficient to lead to a diagnosis.
Atypical viral parotitis does occur and may present with predominantly unilateral swelling or
even submandibular involvement. A single episode of infection confers lifelong
immunity.
Treatment
Symptomatic with regular paracetamol and adequate oral fluid intake.
Complications
Orchitis, oophoritis, pancreatitis, sensorineural deafness and meningoencephalitis are rare,
but are more likely to occur in adults. Other viral agents that produce parotitis include
Coxsackie A and B, parainfluenza 1 and 3, Echo and lymphocytic choriomeningitis.
Bacterial infections
Acute ascending bacterial sialadenitis is historically described in dehydrated elderly patients
following major surgery. Reduced salivary flow secondary to dehydration results in
ascending infection via the parotid duct into the parotid parenchyma. The infecting organism
is usually Staphylococcus aureus or Streptococcus viridans.
Clinical Features
_ Pyrexia, malaise, pain and trismus.
_Red, tender, warm, well-localised, firm swelling is seen in the parotid region (brawny
induration).
_ Tender lymph nodes are palpable in the neck.
_ Features of bacteraemia are present in severe cases.

د.اشرف مزاحم الشاكر
lec. : 2
4
_ Pus or cloudy turbid saliva may be expressed from the parotid duct opening.
Treatment is with appropriate intravenous antibiotics. If the gland becomes fluctuant,
ultrasound may identify abscess formation within the gland that may require aspiration with
a large bore needle or formal drainage under general anaesthesia. In the latter procedure, the
skin incision should be made low to avoid
damage to the lower branch of the facial nerve.
Blunt dissection using sinus forceps is preferred, and the cavity is opened to facilitate
drainage. A drain is inserted and left in situ for 24–72 hours. Sialography is contraindicated
during acute infection. Chronic bacterial sialadenitis is rare in the parotid gland.
RECURRENT CHILDHOOD PAROTITIS
It is a recurrent, rapid enlargement of one or both parotids with fever and malaise in children
of age group between 3-6 years without any known aetiology. Recurrent episodes with a
quiescent period in between are typical. Sialogram shows snowstorm punctate sialectasis.
Low dose antibiotics for long period may be required. Occasionally patient may need total
conservative parotidectomy especially if it occurs late in adolescent period.
Characteristic ‘snowstorm’ appearance of recurrent parotitis of childhood (circled)
Stone formation
Sialolithiasis is less common in the parotid gland (20 per cent) than in the submandibular
gland (80 per cent). Parotid duct stones are usually radiolucent and rarely visible on plain
radiography. They are frequently located at the confluence of the collecting ducts or located
in the distal aspect of the parotid duct adjacent to the parotid papilla. Parotid gland
Sialography is usually required to identify the stone. A stone located in the collecting duct or
within the gland may be managed by either endoscopic retrieval, lithotripsy or, least likely,
surgical removal via a parotidectomy approach.
د.اشرف مزاحم الشاكر
lec. : 2
5
Tumours of the parotid gland
The parotid gland is the most common site for salivary tumours. Most tumours arise in the
superficial lobe and present as slow growing, painless swellings below the ear, in front of the
ear or in the upper aspect of the neck. Less commonly, tumours may arise from the accessory
lobe and present as persistent swellings within the cheek. Rarely, tumours may arise from the
deep lobe of the gland and present
as parapharyngeal masses.
Aetiology
Genetic—loss of alleles of chromosomes in 12q, 8q, 17q. Eskimos are more prone for
salivary neoplasm.
Infective—mumps, Epstein-Barr virus, chronic sialadenitis may be the cause; but not
proved emphatically. Recurrent inflammation can cause duct dysplasia and carcinoma.
Radiation—it is more common in survivors of atomic bomb explosion;
mucoepidermoid carcinoma is more in these patients.
Smoking—adenolymphoma of Warthin’s shows 40% risk in smokers.
Sex—benign tumours and many malignancies are common in females; Warthin’s and
some malignancies are common in males.
Environment and diet—Arctic-Eskimos show dietary deficiency of vitamin A and
develop salivary tumour. Industrial agents like nickel, cadmium, hair dyes, silica,
preservatives may increase the risk of salivary tumours.
80–90 per cent of tumours of the parotid gland are benign, the most common being
pleomorphic adenoma. Malignant salivary gland tumours are divided into two distinct
subgroups:
1 Low-grade malignant tumours, e.g. acinic cell carcinoma, are indistinguishable on
clinical examination from benign neoplasms.
2 High-grade malignant tumours usually present as rapidly growing, often painless
swellings in and around the parotid gland. The tumour presents as either a discrete mass with
infiltration into the overlying skin or a diffuse but hard swelling of the gland with no discrete
mass. Presentation with advanced disease is common, and cervical lymph node metastases
may be present.
Incidence
_ Eighty per cent salivary neoplasms are in the parotids of which 80% are benign; 80% of
these are pleomorphic adenomas.
_ Fifteen per cent of salivary tumours are in the submandibular salivary gland, of which 50%
are benign. 95% of these are pleomorphic adenomas.
د.اشرف مزاحم الشاكر
lec. : 2
6
_ Ten percent of salivary neoplasms are in the minor salivary glands—palate, lips, cheeks,
and sublingual glands. Of these only 10% are benign.
Note:
• Parotid tumours are common but only 20% are malignant.
• Submandibular tumours are uncommon but 50% of them are malignant.
• Minor salivary gland tumours (other than sublingual glands) are rare and 90% of them are
malignant.
• Sublingual salivary tumours are very rare but almost all sublingual salivary tumours are
malignant.
• Incidence of malignancy in salivary glands is inversely related to size of the gland; in
parotid it is 15%; in submandibular it is 50%; in sublingual it is 85%.
PLEOMORPHIC ADENOMA (Mixed Salivary Tumour)
Commonest of the salivary gland tumour in adult.
It is 80% common.
More common in parotids (80%). 10% in submandibular salivary gland; 0.5% in
sublingual salivary gland.
It is mesenchymal, myoepithelial and duct reserve cell origin.
Grossly it contains cartilages, cystic spaces, and solid tissues.
Microscopically it is biphasic in nature with epithelial and stromal components. Benign
tumours will usually not show necrosis.
Even though it is capsulated, tumour may come out as pseudopods and may extend beyond
the main limit of the tumour tissue.
_ When disease occurs in parotid, commonly it involves superficial lobe or superficial and
deep lobe together.
_ But sometimes only deep lobe is involved and then it presents as swelling in the lateral
wall of the pharynx, soft palate and posterior pillar of the fauces. There may not be any
visible swelling in the preauricular region. It is called as ‘dumbbell tumour’. This tumour is
in relation to styloid process, mandible, stylohyoid, styloglossus, stylopharyngeus muscles.
د.اشرف مزاحم الشاكر
lec. : 2
7
Clinical Features
80% common.
Common in females (3:1).
Occurs in any age group. But common in 4th and 5th decade
Usually unilateral.
Present as a single painless, smooth, firm lobulated, mobile swelling in front of the
parotid with positive curtain sign (As the deep fascia is attached above to the
zygomatic bone, it acts as a curtain, not allowing the parotid swelling to move above
that level. Any swelling superficial to the deep fascia will move above the zygomatic
bone).
Obliteration of retromandibular groove is common.
The ear lobule is lifted.
When deep lobe is involved, swelling is commonly located in the lateral wall of
pharynx, posterior pillar and over the soft palate—10%. Deep lobe tumour passes
through Patey’s stylomandibular tunnel pushing tonsils, pharynx, and soft palate often
without any visible swelling or only small swelling when only deep lobe tumour is
present; it also presents as dysphagia. Bidigital palpation of parotid is significant in
such occasion with one finger inside mouth.
Facial nerve is not involved.
Pleomorphic adenoma showing
curtain sign
Typical parotid swelling with ear lobe raised.
Facial nerve should be tested by clenching the teeth.
Complications
Recurrence—5-50%.
Malignancy: 3-5% in early tumours,10% in long duration (15 or more years) tumours.
د.اشرف مزاحم الشاكر
lec. : 2
8
Investigations
FNAC is very important and diagnostic.
CT scan to know the status of deep lobe, local extension and spread.
MRI is better method.
Note:
Incision biopsy of parotid tumour is contraindicated as chances of seedling and recurrence
are high and also there is a chance of injuring the facial nerve, and chance of developing
parotid fistula while doing the biopsy.
Treatment
Surgery—first line treatment.
If only superficial lobe is involved, then superficial parotidectomy is done wherein
parotid superficial to facial nerve is removed.
If both lobes are involved, then total conservative parotidectomy is done by retaining
facial nerve.
Note:
• Enucleation is avoided as it causes high recurrence due to extension of tumour outside as
pseudopods across the capsule.
• Incomplete excision, 10% of tumours which are highly cellular are other causes for
recurrence.
• RT is given after surgery even though it is benign.
• Inexplicable metastasis can occur even though it is benign.
• Tumour may implant due to spillage while surgical removal into retained residual parotid
(deep lobe in superficial parotidectomy).
Recurrence after parotidectomy in pleomorphic adenoma is 5%. It is due to spillage,
improper technique, inadequate margin, retained pseudopods, multicentricity. Recurrent
tumour is multinodular without any capsule. Expression of MUC1/DF3 in the tumour is
marker to predict recurrence.