Introduction to Respiratory system dr.Faris
The main role of the respiratory system is to extract oxygen from external environment and dispose of waste gases, principally carbon dioxide. This requires the lungs to function as efficient bellows, bringing in fresh air and delivering it to the alveoli, and expelling used air at an appropriate rate. Gas exchange is achieved by exposing thin-walled capillaries to the alveolar gas and matching ventilation to blood flowthrough the pulmonary capillary bed. In doing this, the lungs expose a large area of tissue, which can be damaged by dusts, gases and infective agents.
PRESENTING PROBLEMS IN RESPIRATORY DISEASE
Runny, blocked nose and sneezing
Nasal symptoms are extremely common and both common colds and allergic rhinitis cause ‘runny nose’(rhinorrhoea), nasal blockage and attacks of sneezing.
In allergic rhinitis, symptoms may be intermittent, following contact with pollens or animal danders, or persistent, especially when house-dust mite is the allergen.
Cough
Cough is the most frequent symptom of respiratory disease. It is caused by stimulation of sensory nerves in the mucosa of the pharynx, larynx, trachea and bronchi.
Acute sensitisation of the normal cough reflex occurs in a number of conditions, and it is typically induced by changes in air temperature or exposure to irritants such as cigarette smoke or perfumes. Afferent receptors go to the cough centre in the medulla where efferent signals are generated to the expiratory musculature.
Smokers often have a morning cough with a little sputum. A productive cough is the cardinal feature of chronic bronchitis, while dry coughing, particularly at night, can be a symptom of asthma. Cough also occurs in asthmatics after mild exertion or following forced expiration. Cough can also occur for psychological reasons without any definable pathology.
A worsening cough is the most common presenting symptom of lung cancer. The explosive quality of a normal cough is lost in patients with respiratory muscle paralysis or vocal cord palsy. Paralysis of a single vocal cord gives rise to a prolonged, low-pitched, inefficient ‘bovine’ cough accompanied by hoarseness. Coexistence of an inspiratory noise (stridor) indicates partial obstruction of a major airway (e.g. laryngeal oedema, tracheal tumour, scarring, compression or inhaled foreign body) and requires urgent investigation and treatment.
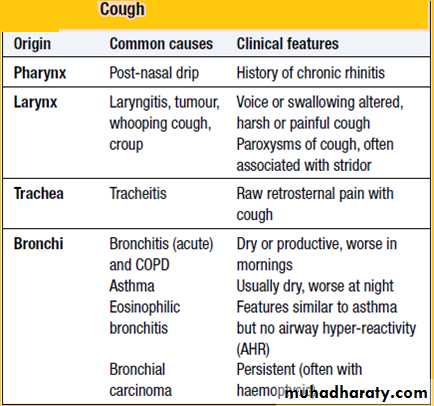
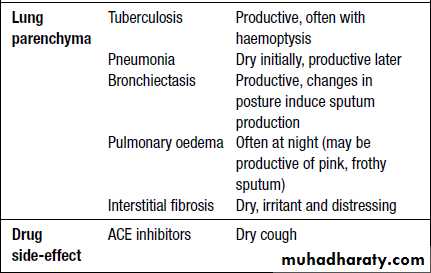
The characteristics of cough originating at various levels of the respiratory tract are detailed in the Box below.
Sputum
Approximately 100 mL of mucus is produced daily in a healthy, non-smoking individual. This flows gradually up the airways, through the larynx, and is then swallowed. Excess mucus is expectorated as sputum. Cigarette smoking is the commonest cause of excess mucus production.Mucoid sputum is clear and white but can contain black specks resulting from the inhalation of carbon. Yellow or green sputum is due to the presence of cellular material, including bronchial epithelial cells, or neutrophil or eosinophil granulocytes.
Yellow sputum is not necessarily due to infection, as eosinophils in the sputum, as seen in asthma, can give the same appearance. The production of large quantities of yellow or green sputum is characteristic of bronchiectasis.
Haemoptysis (blood-stained sputum) varies from small streaks of blood to massive bleeding.
The commonest cause of mild haemoptysis is acute infection, particularly in exacerbations of chronic obstructive pulmonary disease (COPD) but it should not be attributed to this without investigation. Other common causes are pulmonary infarction, bronchial carcinoma and tuberculosis.
In lobar pneumonia, the sputum is usually rusty in appearance rather than frankly blood-stained.
Pink, frothy sputum is seen in pulmonary oedema.
In bronchiectasis, the blood is often mixed with purulent sputum.
Massive haemoptyses (>200 mL of blood in 24 hours) are usually due to bronchiectasis or tuberculosis.
Uncommon causes of haemoptyses are idiopathic pulmonary haemosiderosis, Goodpasture’s syndrome, microscopic polyangiitis, trauma, blood disorders and benign tumours.
Haemoptysis should always be investigated. Although a diagnosis can often be made from a chest X-ray, a normal chest X-ray does not exclude disease. However, if the chest X-ray is normal, CT scanning and bronchoscopy are only diagnostic in about 5% of patients with haemoptysis.
Firm plugs of sputum may be coughed up by patients suffering
from an exacerbation of allergic bronchopulmonary aspergillosis. Sometimes such sputum looks like casts of inflamed bronchi.
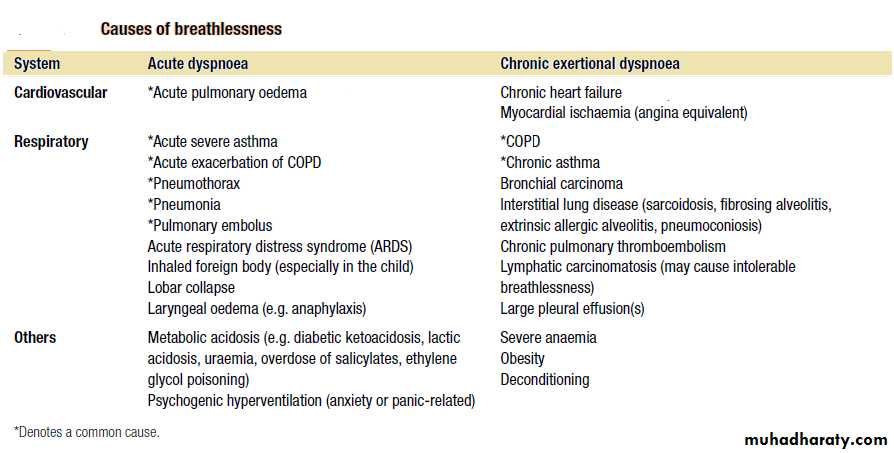
Breathlessness
Dyspnoea is a sense of awareness of increased respiratory effort that is unpleasant and that is recognized by the patient as being inappropriate. Patients often complain of tightness in the chest; this must be differentiated from angina.
Breathlessness should be assessed in relation to the patient’s lifestyle. For example, a moderate degree of breathlessness will be totally disabling if the patient has to climb many flights of stairs to reach home.
Orthopnoea is breathlessness on lying down. While it is classically linked to heart failure, it is partly due to the weight of the abdominal contents pushing the diaphragm up into the thorax. Such patients may also become breathless on bending over.
Tachypnoea and hyperpnoea are, respectively, an increased rate of breathing and an increased level of ventilation. These may be appropriate responses (e.g. during exercise).
Hyperventilation is inappropriate overbreathing. This may occur at rest or on exertion and results in a lowering of the alveolar and arterial PCO2.
Paroxysmal nocturnal dyspnoea is acute episodes of breathlessness at night, typically due to heart failure.
Wheezing
Wheezing is a common complaint and results from airflow limitation due to any cause. The symptom of wheezing is not diagnostic of asthma; other causes include vocal chord dysfunction, bronchiolitis and chronic obstructive pulmonary disease (COPD). Conversely, wheeze may be absent in the early stages of asthma.Chest pain
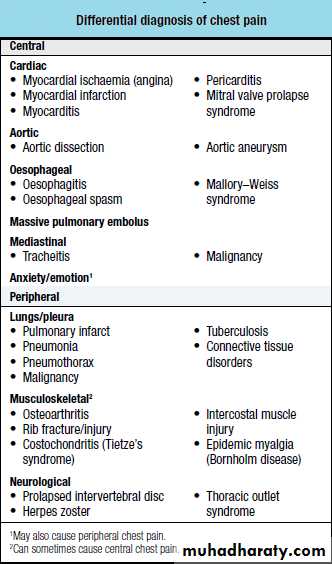
The most common type of chest pain reported in respiratory disease is a localized sharp pain, often termed pleuritic. It is made worse by deep breathing or coughing and the patient can usually localize it. Localized anterior chest pain with tenderness of a costochondral junction is caused by costochondritis.
Shoulder tip pain suggests irritation of the diaphragmatic pleura, while central chest pain radiating to the neck and arms is likely to be cardiac. Retrosternal soreness is associated with tracheitis, while malignant invasion of the chest wall causes a constant, severe, dull pain.