Thoracic outlet syndrome
ا.د اسامه عبيد الخفاجيMBChB
FIBM Cardiothoracic & vascular surgey
MRCS Edn.
Thoracic outlet syndrome
syndromes that result from compression of the neurovascular structures passing from the chest and neck to the upper extremities.The syndrome is caused by compression of the brachial plexus or subclavian-axillary artery and/or vein in the region between the thoracic outlet and the insertion of the pectoralis minor.These syndromes include:
the cervical rib syndrome,
scalenus anticus syndrome,
hyperabduction syndrome,
pectoralis minor syndrome,
the first thoracic rib syndrome
At the superior aperture of the thorax, the subclavian vessels and the brachial plexus traverse the cervicoaxillary canal to reach the upper extremity
Narrowing of this space occurs during functional maneuvers.
during hyperabduction of the arm
in drooping of the shoulders as in poor posture &
during deep inspiration
Compression factors
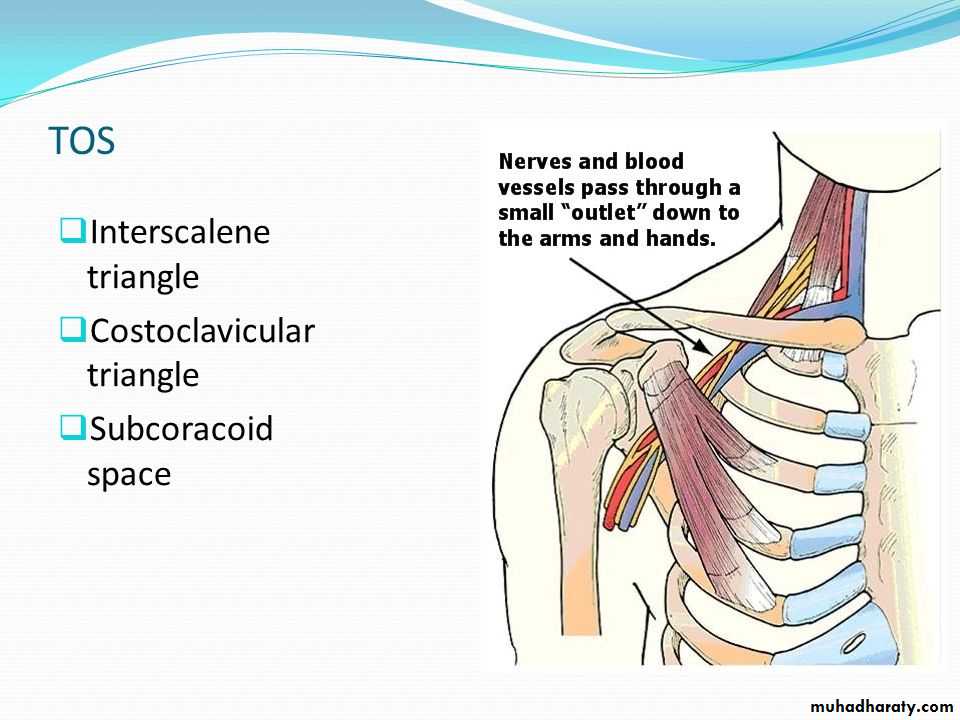
I-Anatomical variation: Potential sites of neurovascular compression
Interscalene triangle
Costoclavicular space
Subcoracoid area
II-Congenital:
Cervical rib and its fascial remnants
Rudimentary first thoracic rib
Exostosis of first thoracic rib
Bifid clavicle
Flat clavicle
Enlarged transverse process of C7
III-Traumatic:
Fracture of clavicleDislocation of head of humerus
Crushing injury to upper thorax
IV-Compression by tumor in the outlet space
V-Atherosclerosis
Clinical presentation
A-Neurological manifestations:
pain,
motor weakness,
paresthesias, and numbness,
Pain is usually of insidious onset in the fingers and hands in an ulnar distribution, but they may occur anywhere in the upper extremity, neck, or shoulder girdle
. The upper cord compression syndrome results from compression or irritation of the upper roots of the brachial plexus (C5, C6, and C7). The pain usually occurs in the upper chest (pseudoangina)
The lower cord compression syndrome is the more common pattern of neurologic symptoms in patients with thoracic outlet syndrome. The lower nerves of the brachial plexus that form the ulnar nerve (C8 and T1) are affected. Pain typically occurs in the posterior neck, medial scapula area, medial aspect of the arm, ulnar aspect of the forearm and hand, and fourth and fifth digits
B-Arterial manifestations:
ischemic pain, numbness and paresthesias,coldnessweakness and easy fatigability in the arm or hand.
These symptoms are accentuated by exercise and exposure to cold.
occasionally aneurysmal dilatation
C-Venous manifestations: Less frequently
pain ,edema of the arm, cyanosis,distention of the superficial veins of the limb and shoulder,
Diagnosis
Clinical maneuversAdson or scalene maneuver: While the physician monitors the radial pulse, the patient takes a deep breath, extends the neck, and turns the chin toward the side being examined. Disappearance or reduction of the radial pulse constitutes a positive finding. During a positive test, a bruit frequently becomes audible in the supraclavicular fossa and the hand may become cool and pale. The deep breath causes elevation of the first rib and extending and turning the neck causes narrowing of the interscalene triangle. If the pulse is altered before the head is turned, one should suspect the presence of a cervical rib.
Costoclavicular compressive maneuver: While the radial pulse is monitored, the patient places his or her shoulders back and downward into an exaggerated military position. Disappearance or reduction of the radial pulse or appearance of a subclavian bruit constitutes a positive finding.
Hyperabduction maneuver: The radial pulse is monitored while the arm is passively moved into a hyperabducted position. Reduction or cessation of the radial pulse and the appearance of an axillary bruit indicate arterial compression.
Three-minute elevated arm stress test: The patient is asked to slowly open and close the hands while keeping both arms abducted, externally rotated, and flexed to 90 degrees at the elbow. Normal patients may experience fatigue but rarely have pain or paresthesias. In patients with a thoracic outlet syndrome, this test may reproduce their symptoms.
Investigations :
Chest and neck X-ray: may demonstrate
cervical ribs,
anomalous first ribs,
prominent transverse processes,
bony exostoses
CT scan
EMG
Angiography
Color duplex
MRI & MRA


Management:
Conservative (physiotherapy):For all patients, except those with
symptomatic arterial occlusion & distal embolization,
a poststenotic aneurysm,
symptomatic venous occlusion,
conservative management include:
weight reduction
exercise program directed toward
improving posture,
strengthening the elevators of the shoulder girdle,
active neck exercise (strengthening scalenus muscles)
avoiding hyperabduction
Surgical therapy:
Indicated in
Patients with major neurologic or vascular complications
those who do not respond to a 4-month (or longer) trial of nonoperative management.
Operative management include:
excision of the cervical rib
division of the scalene muscles
removal of a major portion of the 1st rib