Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
1
Interpretation of abnormal Chest radiograph
Let us review what we learned:
1- Film labeling
2-Technical aspect of the film.
3-The diaphragm :
* Should be clearly visible, except where the heart and mediastinum are in
contact .
* Good inspiration ---level regarding the ribs.
* The Rt hemidiaphragm usually being up to 2.5 cm higher than the Lt
4- check the size and shape of the heart –later
5- check the position of the heart and mediastinum .
* trachea: midway or slightly to Rt of mid point between the medial end of
clavicles- be aware of rotation.
* Heart : very variable ,usually one-third lies to Rt of the midline.
6-look at the mediastinum :
* Outline should clear except in contact with diaphragm
* In young children – normal thymus should not be mistaken for disease
7- examine the hilar shadow :
* The hilar shadows represent the pulmonary arteries and veins
* The Lt hilum is usually higher in position than Rt
8- examine the lungs
* The only structures that can be identified within normal lungs are blood vessels,
the interlobar fissures, and the walls of certain larger bronchi seen end-on .
Positions of fissures ?
* Looks for abnormal pulmonary opacities (white) or translucency (black)
* Do not mistake : pectoralis muscles, breasts, nipples ,plaits of hair , skin lumps
* A good way of finding a subtle shadow is to compare one lung with other zone
by zone.
* Lateral film ?
9- Check the integrity of the ribs, clavicles, scapula, and spine and examine the soft
tissues
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
2
* In female check the presence of breast (mastectomy)
* Reduction in the soft tissue bulk leads to increase transradiancy (blackness) of that
side of the chest.
10- check the costophrenic angles and under the diaphragm
Interpretation of abnormal Chest radiograph
Where is the abnormality ? –Location ---- Define
How extensive is it ?-------------- ----------- Description
What is it ?------------------------------------- Diagnosis (ddx)
-----------
3 Ds
1. Define (Location )!!!
e.g.
If the shadow is surrounded on all sides ( PA & lateral
films ) by aerated lung it must arise within the lung .
If the shadow has a broad base with smooth convex
borders projecting into the lung and a well defined
outlines its likely to be pleural, extrapleural or
mediastinal in origin.
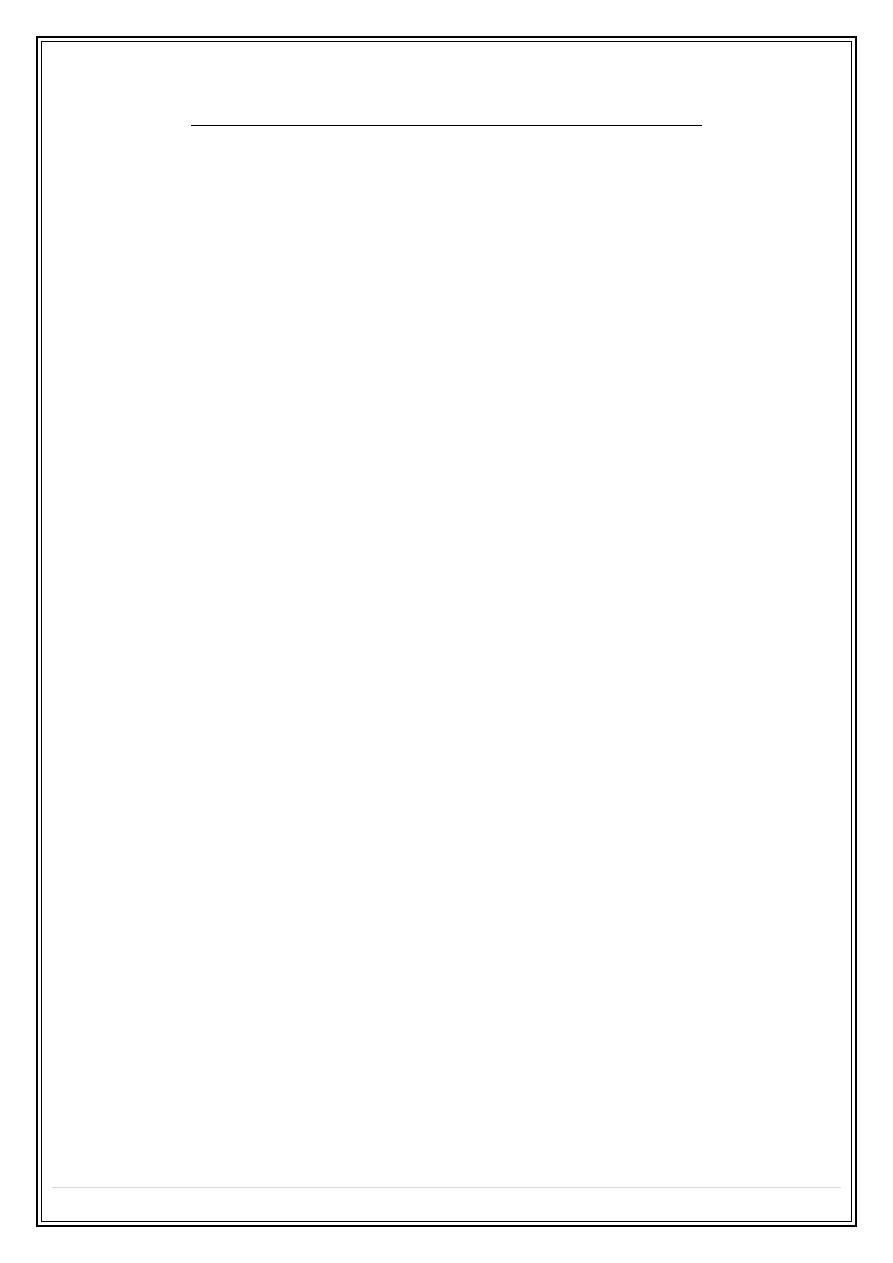
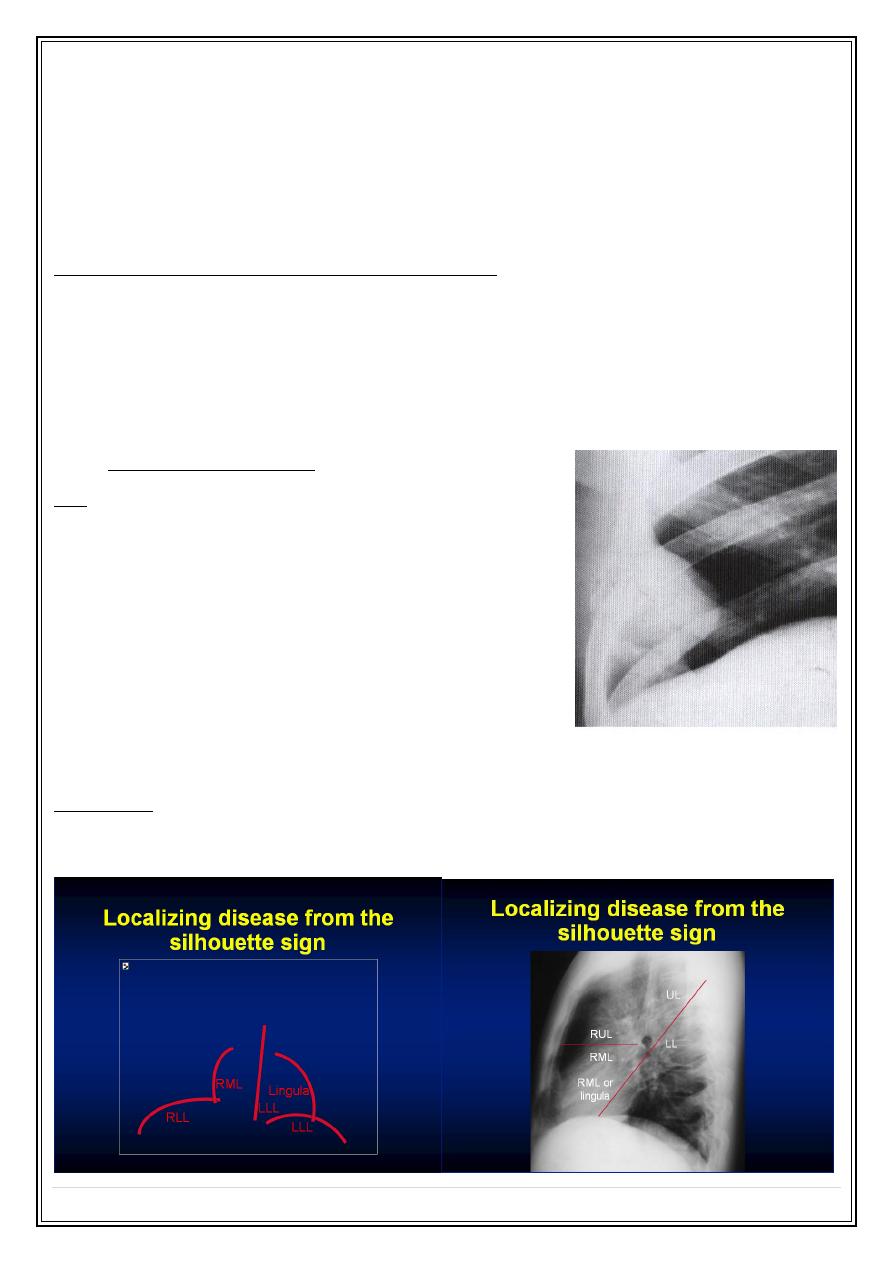
The silhouette sign ?
An intrathoracic lesion touching a border of the heart,
aorta or diaphragm obliterates that border on the chest radiograph.
Benefit !! :
Localization e.g. loss of heart border means the that the shadow lies in the
anterior half of the chest.
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
3
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
4
2.Description!!! + 3.Differntial diagnosis for each Abnormal Lung patterns :
1. Alveolar/ acinar shadow .
2. Spherical shadows ( lung masses, lung nodules).
3. Interstitial shadow.
4. Changing transradiancy pattern.
5. Vascular pattern.
6. Bronchial pattern .
1. Alveolar/ acinar pattern :
A- Air – space filling (infiltrate).
Replacement of the air in the alveoli by:
1. Fluid :
❖
Transudate------ (pulmonary edema)
❖
Exudates (consolidation )
infection (pneumonia)
infarction.
contusion.
hemorrhage
Immunological disorders e.g. collagen vascular disease
and extrensic allergic alveolitis
Note : there is no way of telling from the chest radiograph which of these
possibilities is the cause.
2. Other materials e.g. tumour cells
B- Collapse (atelectasis)
Signs of air - space filling ?
1. A shadow with ill-defined borders except where the opacity is in contact with a
fissure.
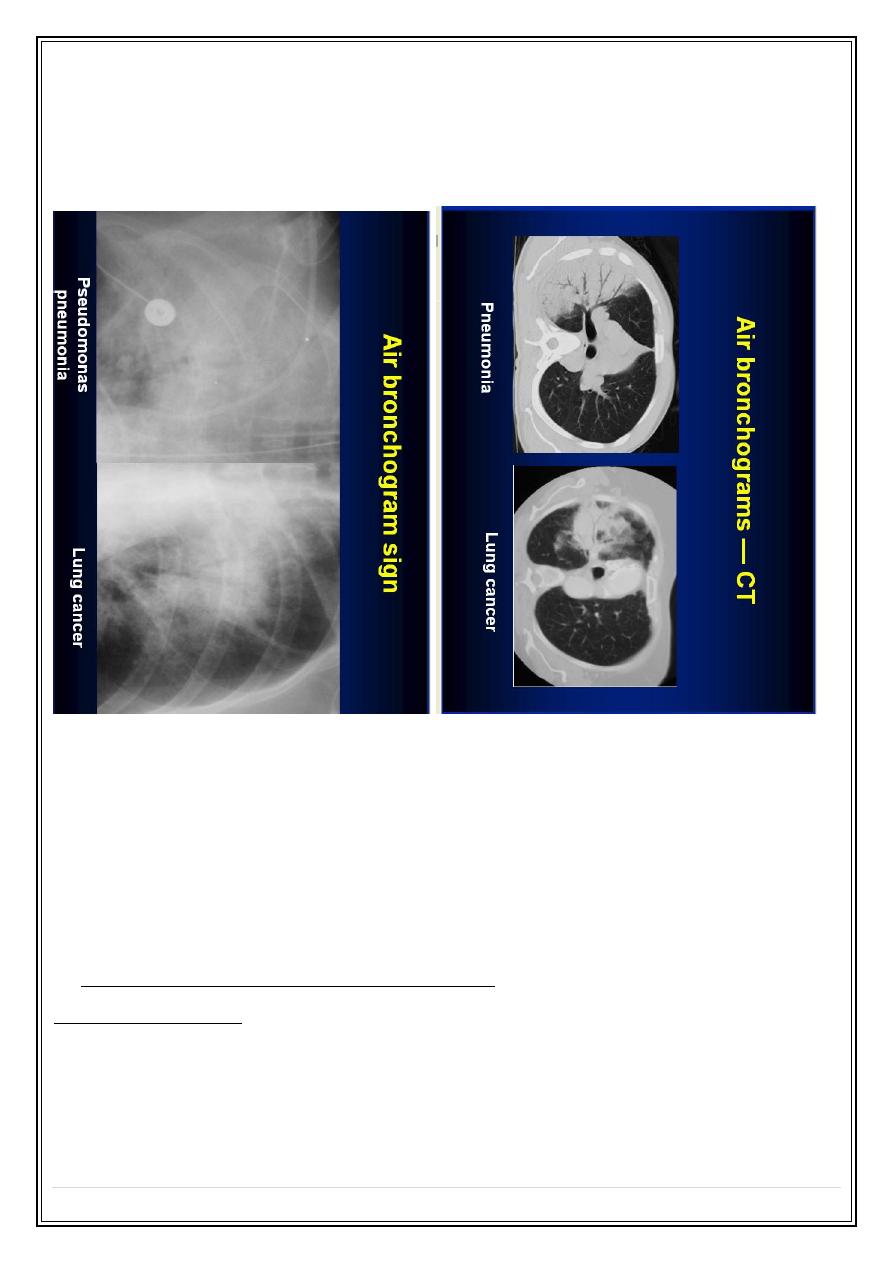
2. An air-bronchogram ?
What is this ???
Normally its not possible to identify air in the bronchi within normally aerated
lung( because the walls of the bronchi are too thin and air filled bronchi are
surrounded by air in the alveoli.
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
5
But if the alveoli are filled with fluid, air in the bronchi contrasts with fluid in the
alveoli producing radiolucent streaks. Called air bronchogram . this sign is seen to
great advantages on CT (CT air bronchogram ).
3. The Silhouette sign
Consolidation :
•
Ground glass ----- hazy area of increased attenuation not obscuring
bronchovascular markings ( ddx interstitial lung disease ).
•
Patchy ------ area of marked increase in attenuation with obliteration of underlying
anatomical features, not restricted to a lobe.
•
Lobar ----- same as patchy consolidation, but restrict to a lobe.
2.Spherical shadow ( nodule, mass )
Solitary lung nodule :
The common causes of a solitary pulmonary nodule:
➢
malignant tumour ( 40 % of solitary pulmonary nodule are malignant)
---- primary (lung ca)
---- secondary metastasis
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
6
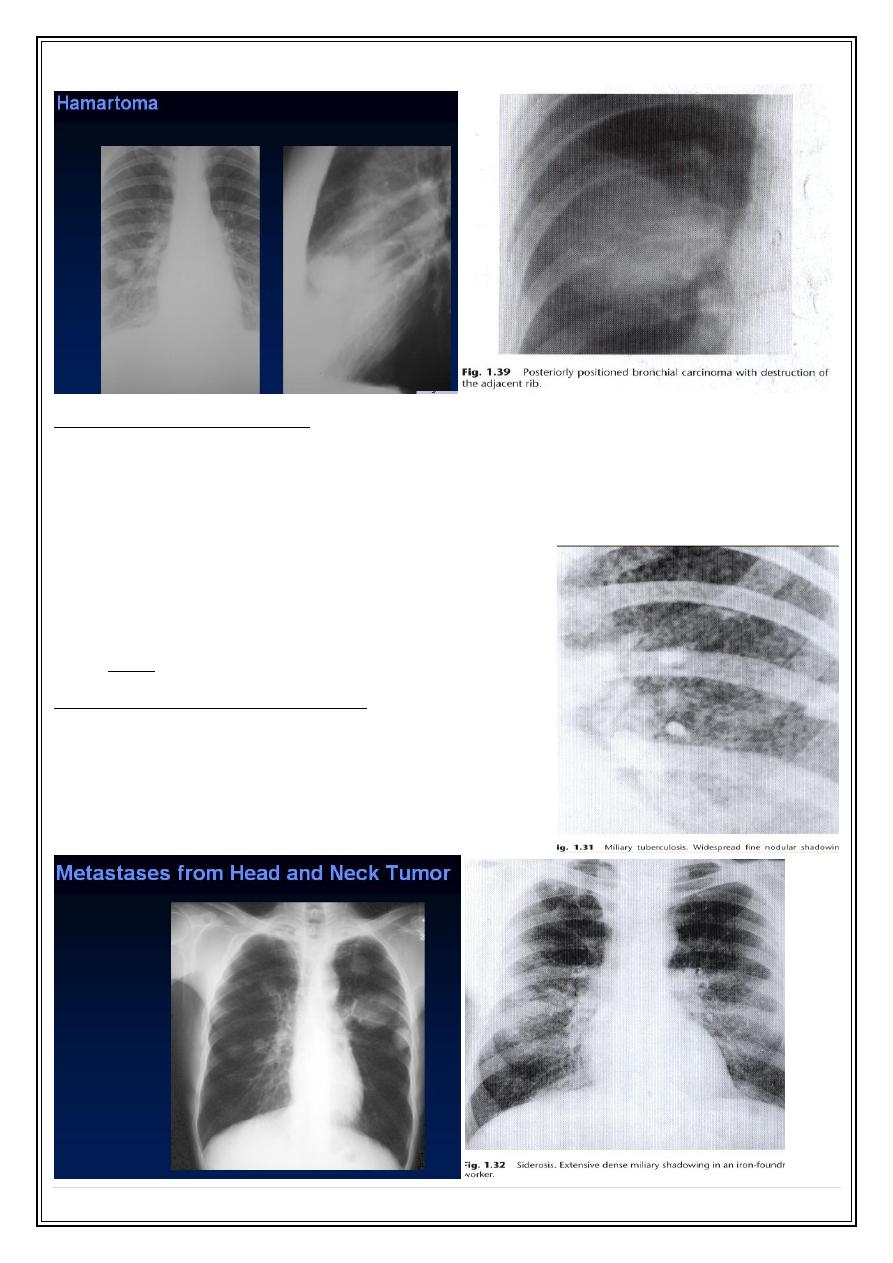
➢
Benign tumor ---- hamartoma
➢
Infection ---- round pneumonia.
---- abscess
---- Hydatid
➢
granuloma ----.e.g. TB
➢
Pleural --- loculated effusion
--- pleural tumor
What is to look within a mass ?
1. Location.
2. Size. (masses larger than 4 cm are predominantly primary malignancy, metastasis
,lung abscess or pleural fibroma)or rarely spherical pneumonia
3. Shape & outline.( carcinomas are often irregular, speculated “infiltrating" or
notched margins)
4. Presence of calcification.( calcification favoring benign lesion such as hamartoma
or TB granuloma, although others rarely do)
5. Presence of cavitation.
6. Associated abnormalities such as ( bone destruction, effusion, collapse,
lymphadenopathy ).
7. Other lesions.
Adjuvant signs ?
1. Comparison with previous films—doubling time !!(usually malignant lesion have a
doubling time of1-6 months) while failure to grow over a period of 18 months or
more is a strong pointer to either benign tumor or an inactive granuloma
2. Age of the patient.
3. Symptoms.
The role of CT in patient with solitary pulmonary nodule :
1. Demonstrate calcification not clearly seen on plain radiograph
2. Estimate the rate of growth of a very small asymptomatic nodule
3- stage the extent of disease in those cases where the nodule is likely to be a primary
carcinoma
4- establish whether or not the nodule is solitary or multiple
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
7
Multiple pulmonary nodules :
The common causes of multiple pulmonary nodules:
❖
Tumor --Benign – hamartoma
--Malignant - metastases (most), lymphoma
❖
Infection ---- granuloma e.g. TB (most )
---- round pneumonia
---- abscess
---- hydatid
Note metastases are frequently of variable sizes
Miliary nodules : ( miliary shadow )
Multiple small micro nodules ( 2-4 mm )
The usual causes include:
1.miliary TB
2.miliary metastases
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
8
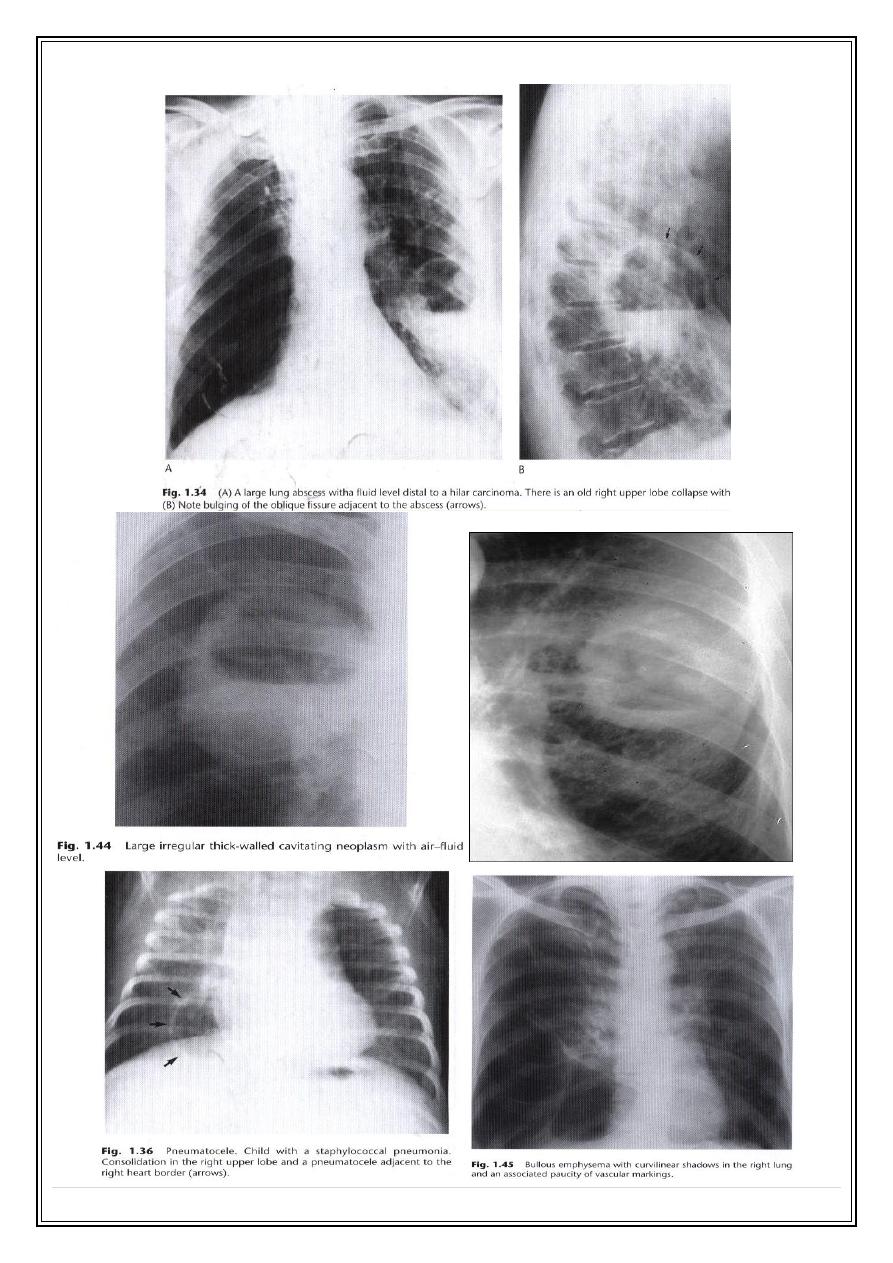
Cavitating lesions & cysts :
A cavity is a gas-filled space surrounded by a complete wall which is 3 mm or greater in
thickness.
Thinner walls cavities are called cysts or ring shadows.
Common Cavitating process :
1. Lung abscess.
2. TB.
3. staphylococcal infections.
4. Primary carcinoma ( in the tumour mass it self or the distal lung ).
Particular features of importance ?
1. the site. (TB cavities are usually upper zone, in the posterior segments of the
upper lobes or apical segments of the lower lobe )
2. the wall of the cavity. (thick & thin )
3. the presence of fluid level.( common in primary tumor ,uncommon in Cavitating
metastases &TB)
4. Contents.( e.g fungal ball, blood clot)
5. the state of surrounding lung.
Thick wall cavity ?
acute abscess
most neoplasm
most metastases
Thin wall lesion or ring shadow?
bullas
Pneumatoceles ( staphylococcal infection in children )
Hydatid cyst
Chronic inactive TB
traumatic lung cyst
tumour
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
9
Large irregular thick wall Cavitating neoplasm:
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
10
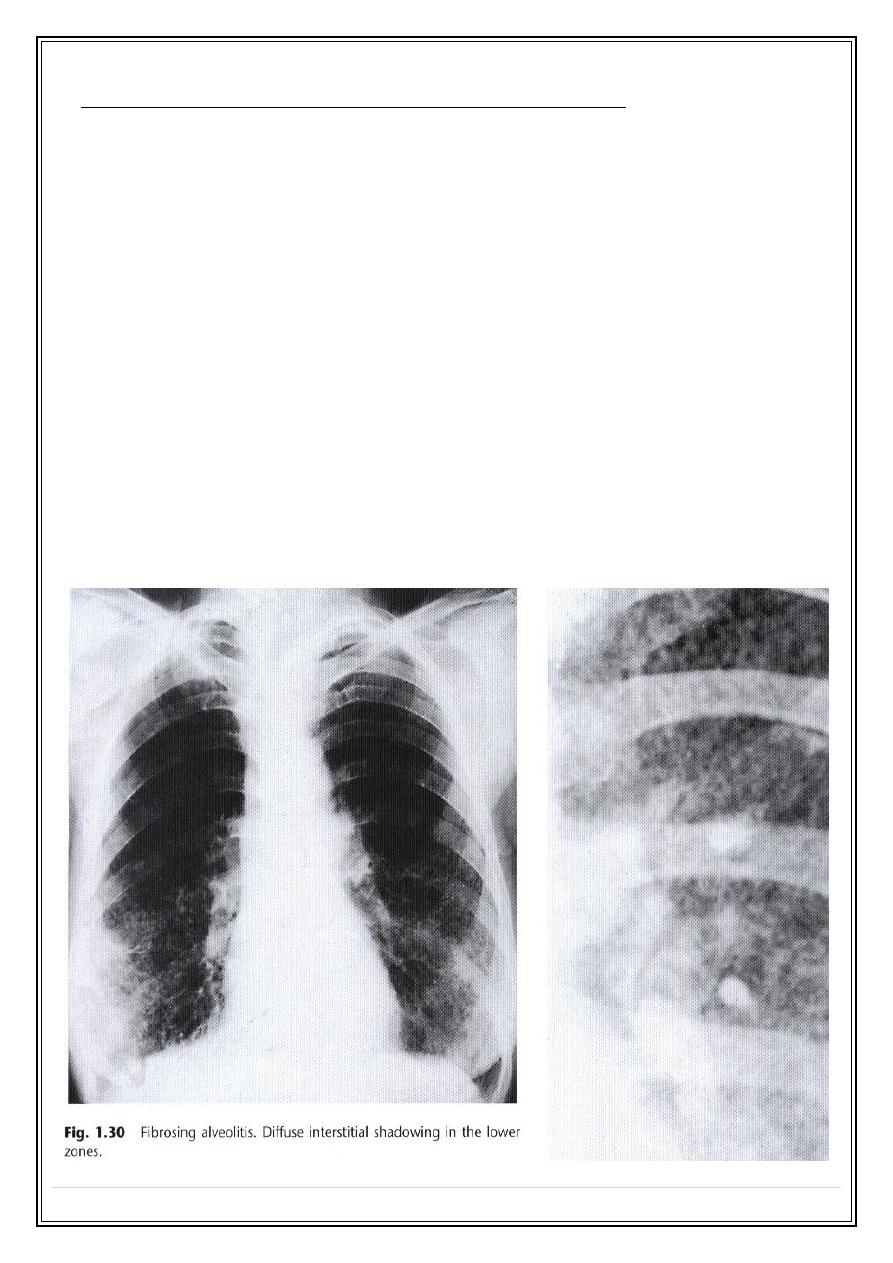
3.Interstitiasl pattern : ( diffuse lung diseases )
o
miliary shadowing
o
ground glass appearance.
o
nodular ( less than 1 cm )
o
reticular.
o
reticulondular .
o
honeycomb shadowing – 5-10 mm sizes thin wall cysts--- end stage of pulmonary
fibrosis.
Causes of diffuse bilateral reticulondular shadowing ?
1.infection ( interstitial pneumonitis ) ( virus , mycoplasma, fungi ).
2. pneumoconiosis ( silicosis , asbestosis ).
3. collagen disease.
4. cardiac ( pulmonary edema -- could be acinar or reticolonodular )
5. miscellaneous (fibrosing alveolitis,lymphangitis carcinomatosis).
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
11
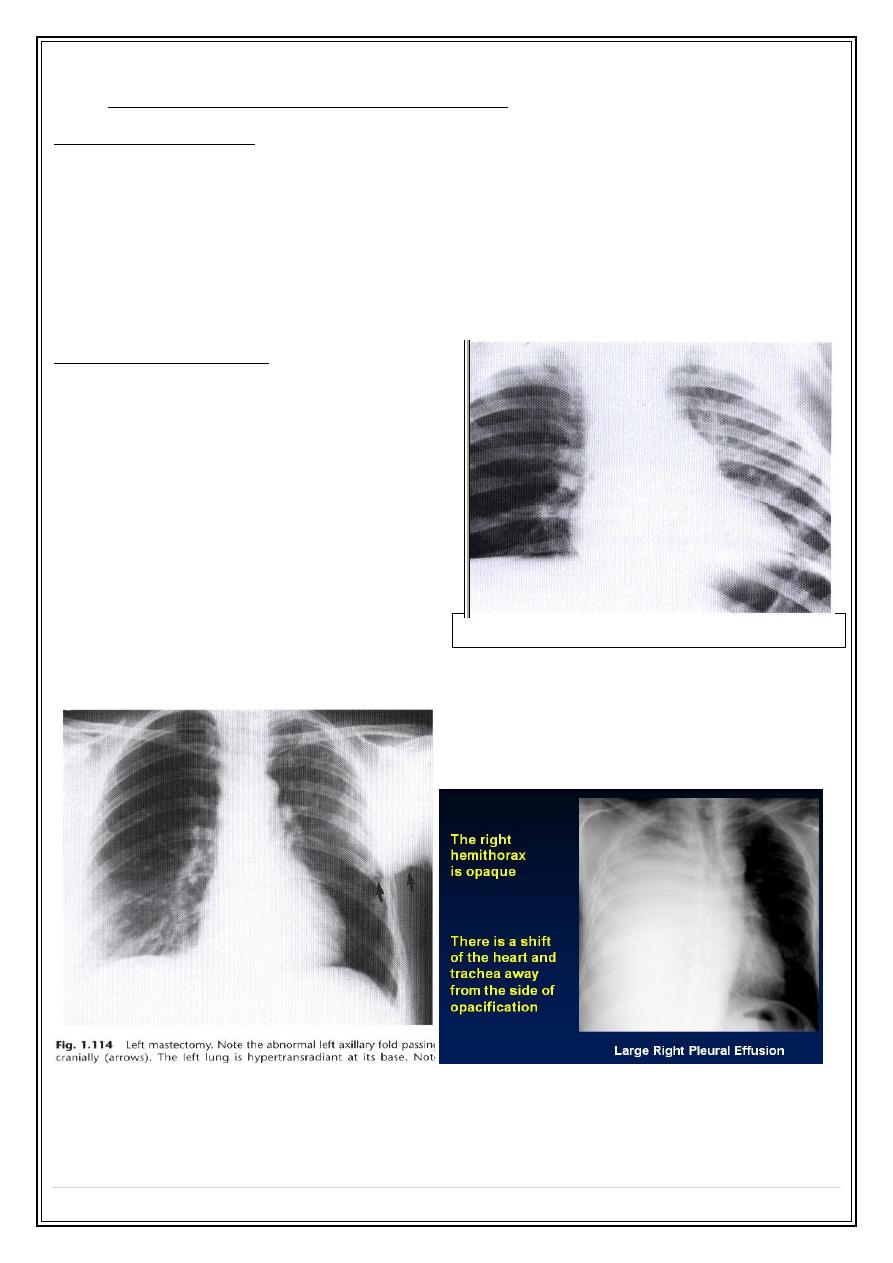
4.changing transradiancy pattern :
Increase transradiancy
a- both lungs - asthma
- emphysema
b. unilateral - soft tissue ( mastectomy )
- emphysema * compensatory ( lobar collapse, lobectomy.)
* obstructive ( FB, tumour)
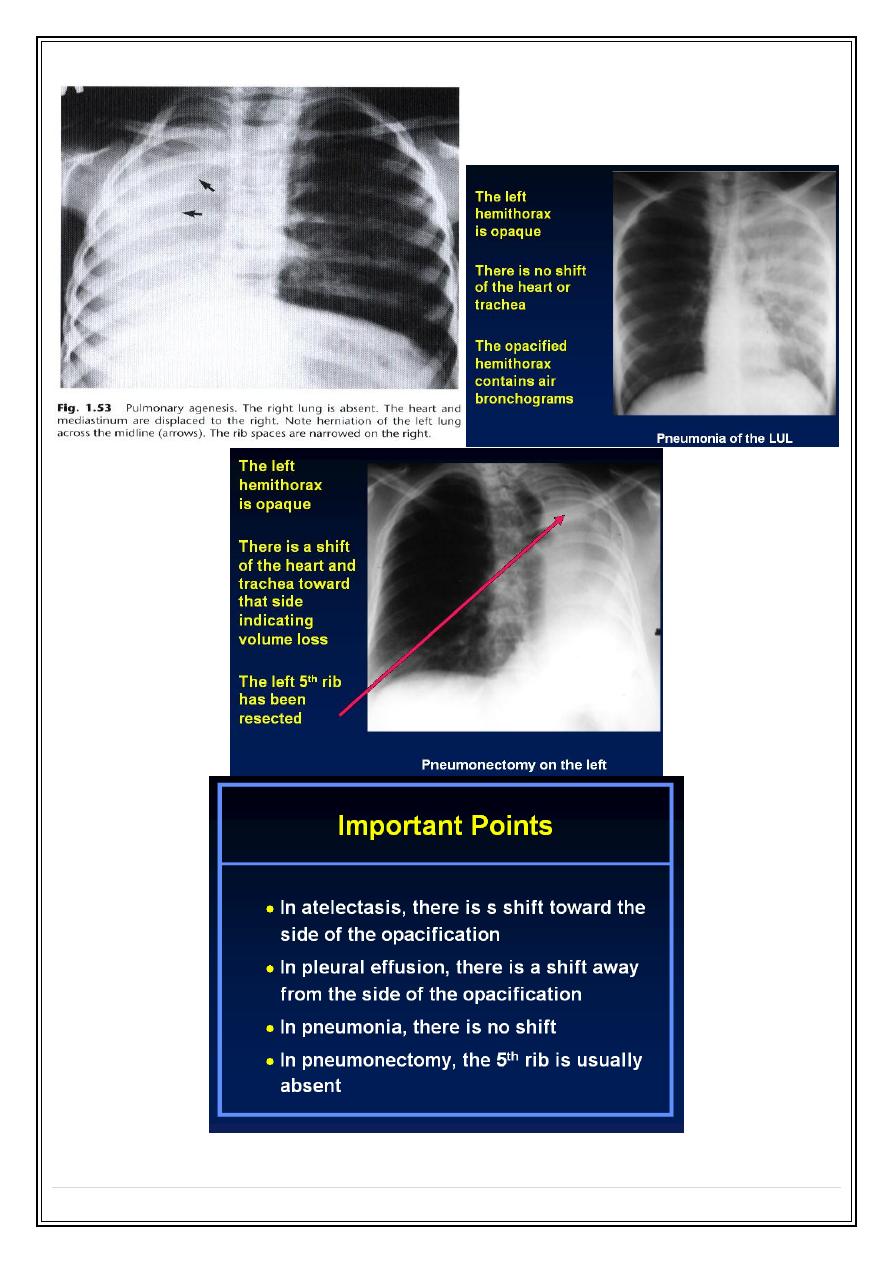
Decrease transradiancy:
causes of opaque hemithorax
1. pleural ( large effusion ).
2. congenital ( pulmonary agenesis )
3. pulmonary ( collapse/consolidation ).
4. surgical ( pneumonectomy )
Obstructive emphysema—Rt lung —inhaled FB
Secret Lectures
(4)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
12
Thank You,,,