Fifth Stage
E.N.T
Dr.Mushtaq – Lecture 17
1
Epistaxis
Greek term “ epistazo” means to bleed from nose
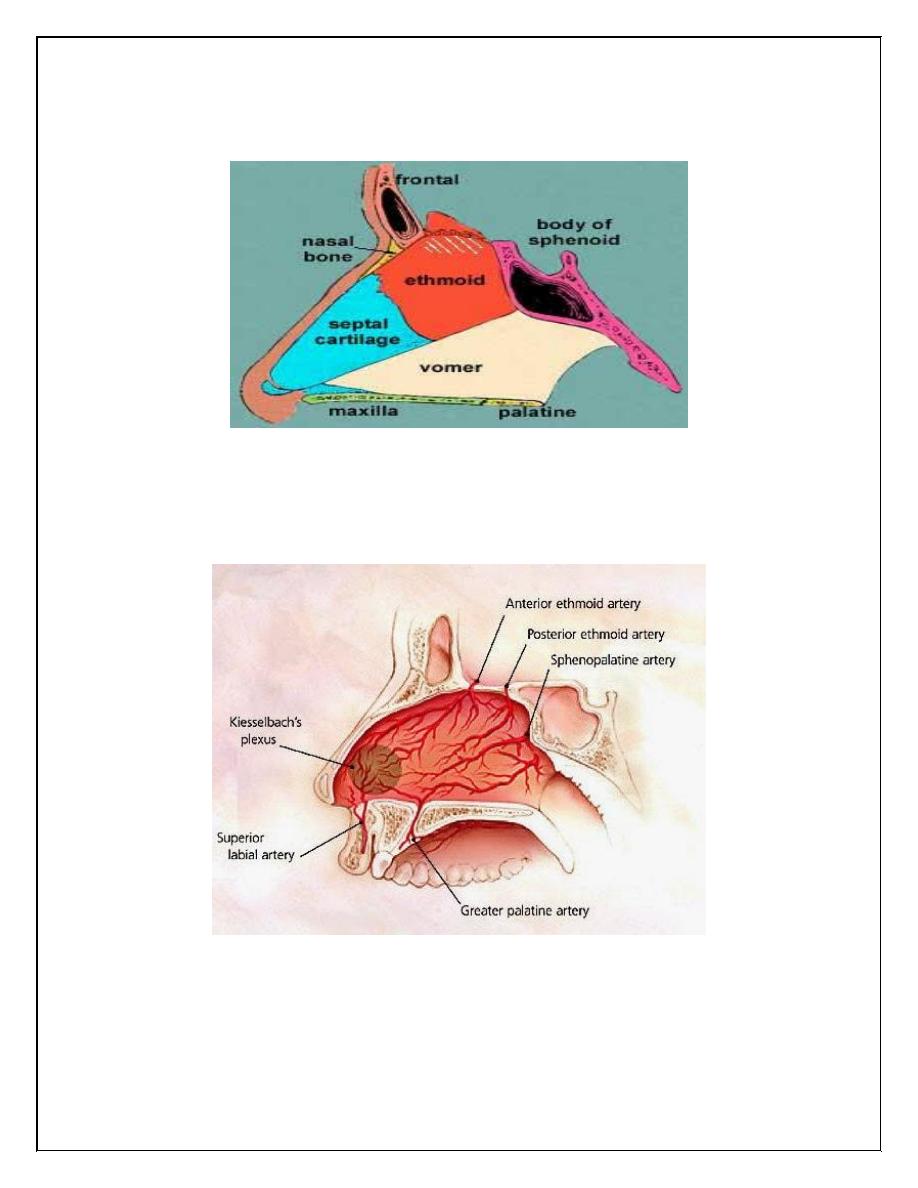
Blood supply of the nasal septum
Woodruff`s plexus // posterior part of inf. Meatus
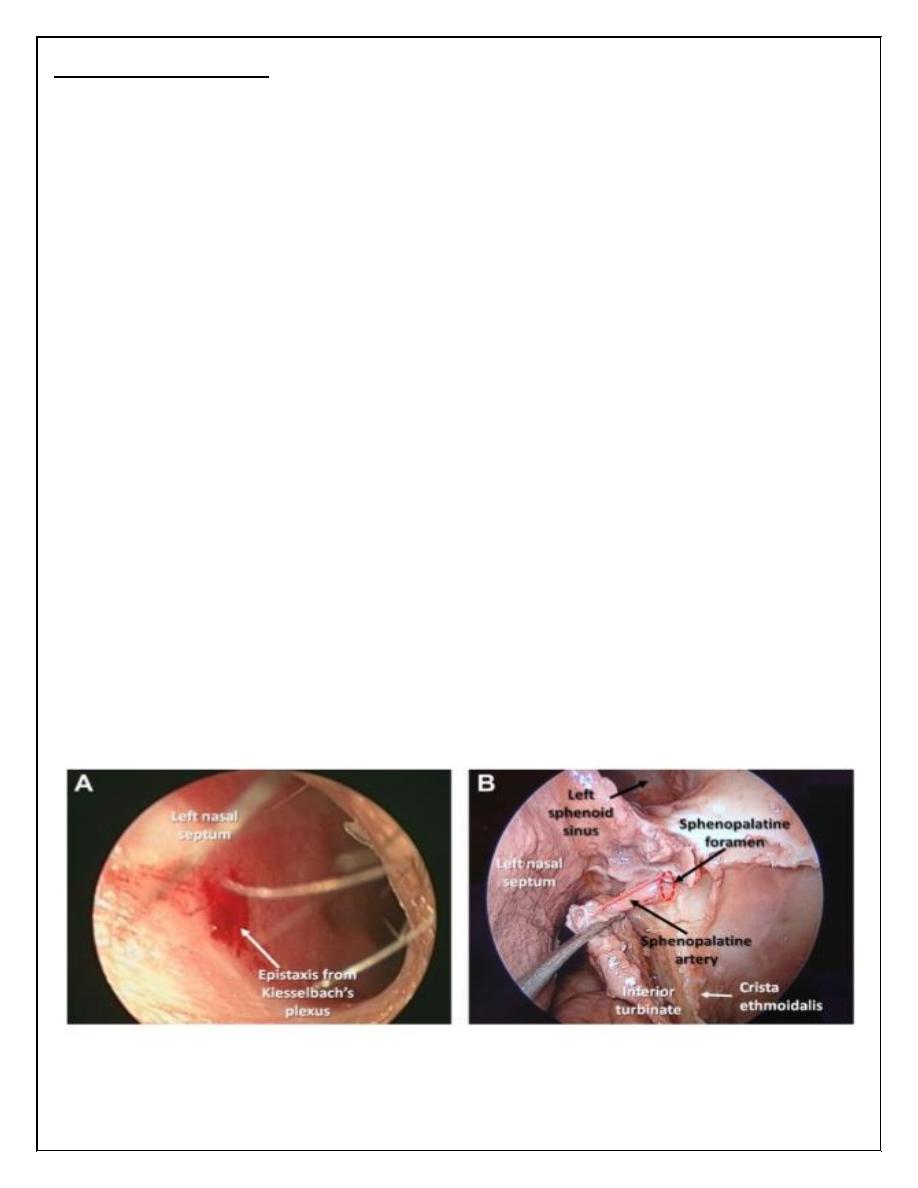
Kiesselbach`s plexus // ant. Part of the septum (Little`s area) 90%
Epidemiology
• Lifelong incidence of epistaxis in general populations is about 60%
• Fewer seek medical attendance
• Peak incidence in children(2-5 yrs) & adult ( 50 -80 yrs).
2
AETIOLOGY
• Aetiological factors:
1.Idiopathic : 80%
2.Trauma : Digital, external nasal trauma or iatrogenic.
3.Coagulopathy : Idiopathic thrombocytopenia (ITP) Disseminated
intravascular coagulopathy (DIC) .
4.Drugs : Warfarin, aspirin, clopidogrel, (NSAIDs)
5.Chronic granulomatous disease : Wegener’s granuloma, sarcoidosis
6.Neoplastic: Angiofibroma, inverted papilloma, squamous cell cancer
7.Hereditary : Hereditary haemorrhagic telangiectasia (HHT), haemophilia,
Von Willebrand’s factor deficiency.
• Aetiological associations:
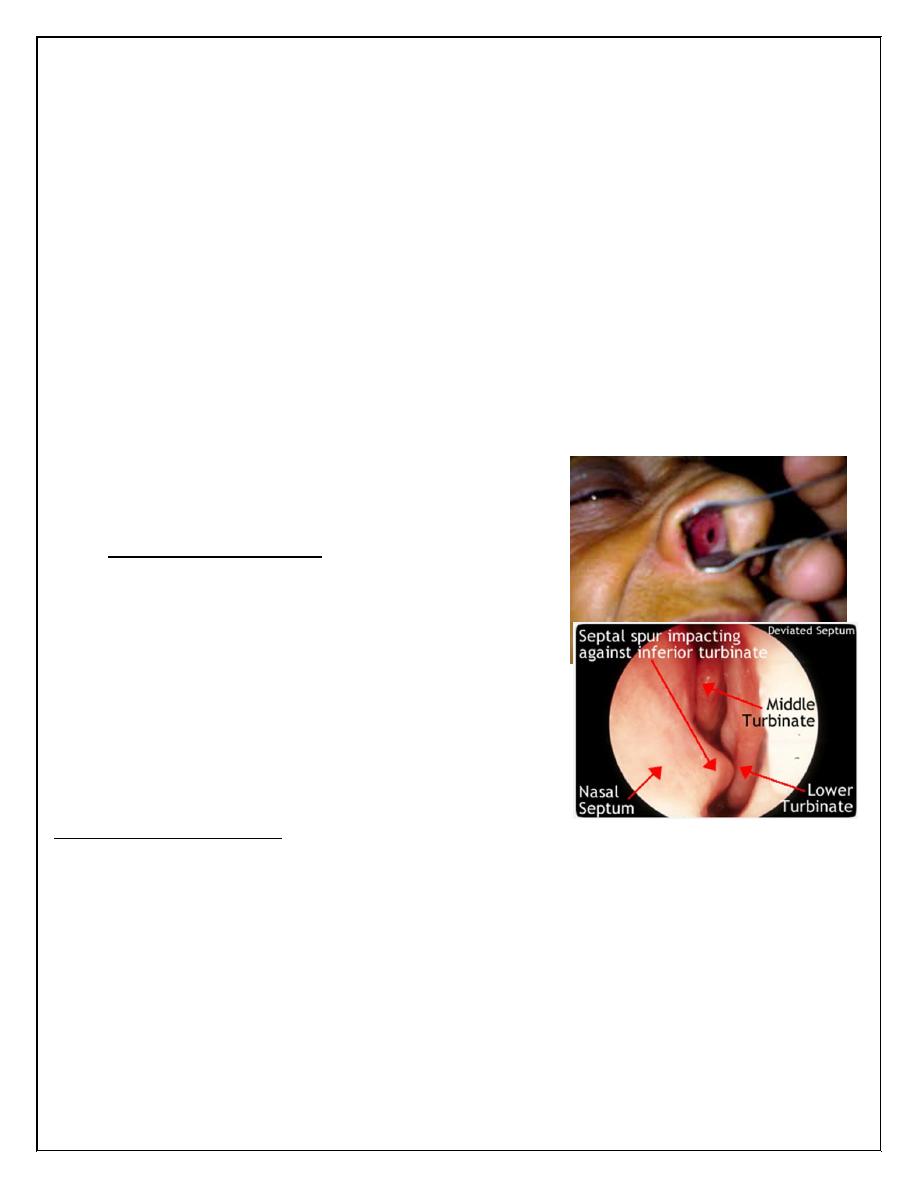
1.Septal abnormalities : Spurs, perforations
2.Alcohol
3.Hypertension
Evaluation and Management
History and Physical Exam
1. Age,
2. Amount of bl. loss ,onset duration, intermittent or continuous , spontaneous or induced,
unilat or bilat. Bleeding from other site, fainting , type of packs was previously used indicate of
severity .
3. Medical History and Blood disease ,blood transfusion
4. Medications: antiplatelet , anticoagulants.
5. Social History: cocaine abuse, alcoholism, smoking
3
6. Family history , pregnancy
7. Toxin Exposure: ammonia, gasoline, phosphorus.
8. Other :trauma ,high altitude living ,allergy, sinusitis rhinitis, URI
Physical Examination
• patient should sit up with body tilted forward
• initial attempt to stop bleeding by applying pressure to nasal alae for several minutes
• decongestant/anesthetic agents .
• adequate lighting, nasal speculum, suctions machine ,attempt to localize active bleeding
(examine for abrasions, foreign bodies, masses, sign of infection …etc.).
• general ex. : vital signs ,pallor ,jaundice, ecchymosis, melena, haematuria, haemoptysis
• for chronic or recurrent epistaxis without an obvious bleeding source
patient should undergo an endoscopic exam
Investigations:
• C.B.F. , E.S.R. , B/ FILM
• Proth. time, partial thromboplastin time ,bleeding time and clotting time.
• Liver enzymes( Liver function tests).
• S. Fibrinogen ,ferritin .
• Blood group
• Clotting factors.
• Renal function tests
Management
• Control significant bleeding before lengthily history
• Steps:
1- first aids and resuscitations
2- localization of bleeding
3- control bleeding
4- assess blood loss.
5- prevention
4
First aids & resuscitation
• ABC
• Neck should not be hyperextend to prevent blood flow into the stomach or possible
aspiration.
• Trotter`s method:
-- blood in mouth should not be swallowed.
-- mouth breathing.
-- direct pressure over the cartilaginous part of the nose for 5minutes is usually
sufficient
-- gauze moisten with epinephrine may be placed to promote vasoconstriction
• applying of pledge socked with anesthetic-vasoconstrictor solution into nasal cavity to
anesthetize and shrink the mucosa.
• Localization the site of bleeding ..
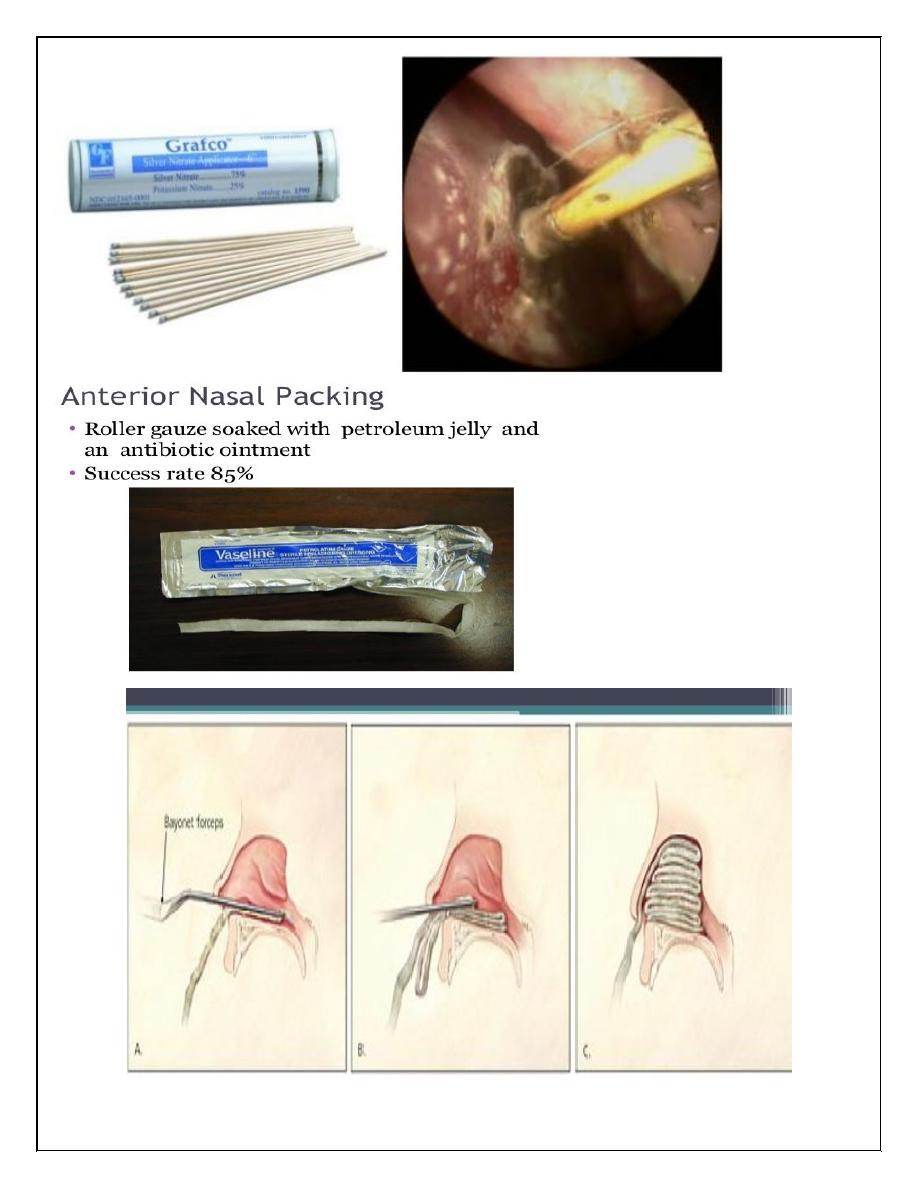
• Cauterize the bleeding point with silver nitrate stick under L/A or electrocautery under
local or general anesthesia.
• If bleeding stops , blood sample should be sent for investigation and cross matching
especially in sever cases.
• Intravenous infusion to replace hypovolaemia
• Antibiotics ,analgesia and sometime sedation may be essential.
5
6
7
8
Thank you,,,