1
Anaemia of Chronic Disease (ACD)
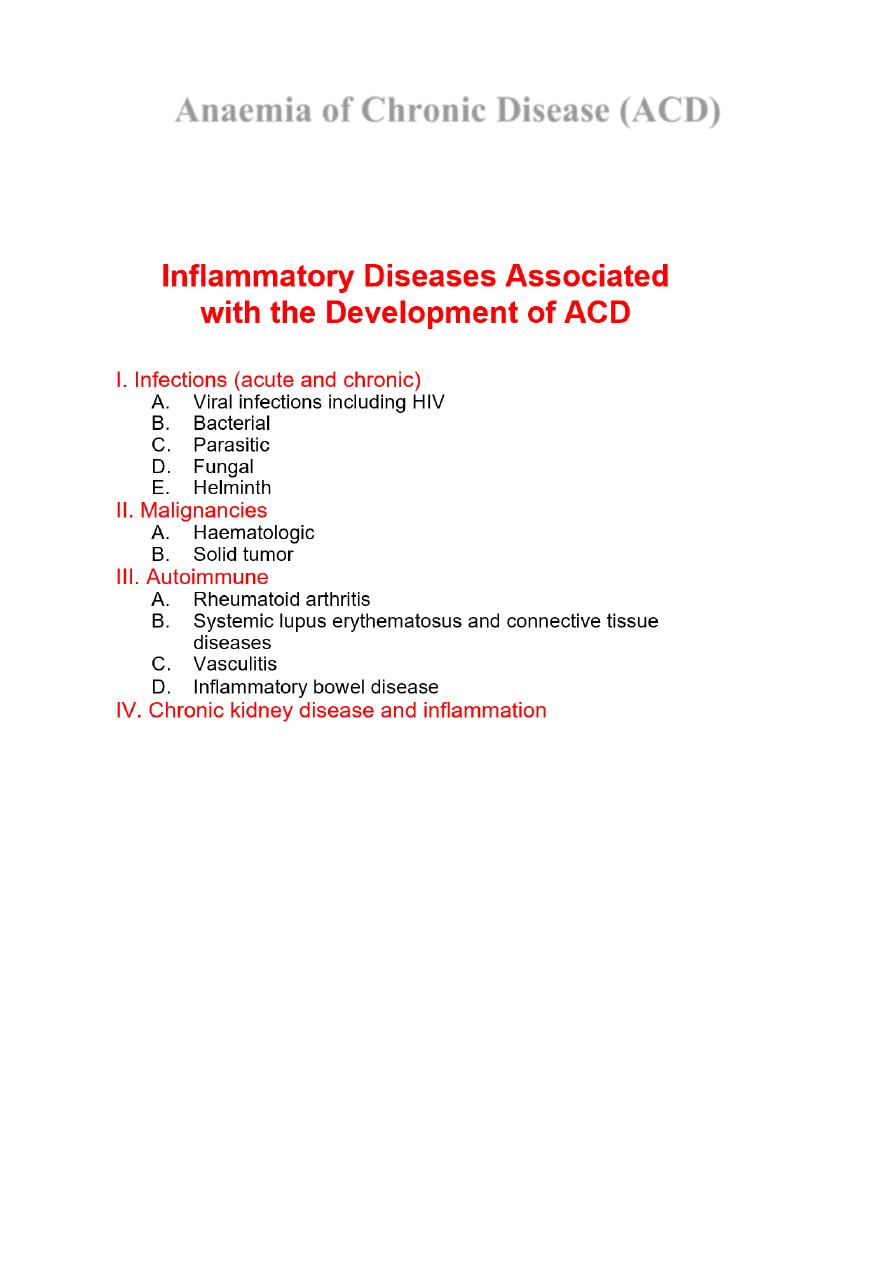
Anaemia of chronic disease (ACD), also known as anaemia of inflammation (AI), is a
common type of anaemia, particularly in hospital populations. It occurs in the setting of
chronic infection, chronic inflammation or neoplasia.
Pathophysiology—Cornerstones
The anaemia is not related to bleeding, haemolysis or marrow infiltration, is mild, with
haemoglobin in the range of 85–115 g/L, and is usually associated with a normal MCV
(normocytic, normochromic),
Hepcidin
Master Regulator of Iron Homeostasis
Pathogenesis It has recently become clear that the key regulatory protein that accounts for the
findings characteristic of ACD is hepcidin, which is produced by the liver.
Hepcidin production is induced by pro-inflammatory cytokines, especially IL-6. Hepcidin
binds to ferroportin on the membrane of iron-exporting cells, such as small intestinal
enterocytes and macrophages, internalising the ferroportin and thereby inhibiting the export
of iron from these cells into the blood.
2
The iron remains trapped inside the cells in the form of ferritin, levels of which are therefore
normal or high in the face of significant anaemia.
Iron retention within the reticulo-endothelial system
Inadequate formation and function of erythropoietin
Impairment of erythrocyte progenitor formation
ACD Diagnosis
ACD Best Therapy
Treatment or Cure of the Underlying Disease!
Current Therapeutic Options in ACD
• Blood transfusions
• Recombinant human erythropoietin
• Iron
Therapeutic measures are aimed to increase haemoglobin levels in ACD patients
ACD Therapy
Blood Transfusions
• Can be readily used for rapid correction of severe anaemia
• Immediate increase of haemoglobin
• 1 unit contains ~200 mg of iron
Iron
• NO,
if
infections
or
cancer
underlie
ACD;
ferritin >100 ng/mL
• May favor proliferation of pathogens
• By countering iron-withholding strategy
• By impairing immune function
• May not reach erythroid cells due to diversion into reticulo-endothelial system

3
• May cause tissue damage via formation of toxic radicals by the Fenton reaction (triggered
by TNF-a)
• However, in autoimmune diseases, iron may inhibit pro-inflammatory immune effector
pathways, thus reducing disease activity
• What to do in ACD with true iron deficiency (ACD and bleeding)?
• Iron is needed for basic metabolic functions
• How to substitute iron?
• Iron is very poorly absorbed in ACD (down-regulation of ferroportin in the duodenum by
hepcidin)
• IV iron administration is very effective in inflammatory bowel disease and ACD
Iron Therapy in Dialysis Patients
Prospective study investigating the incidence of infectious complications in ESRD patients
receiving IV iron therapy
Group 1: ferritin <100 ng/mL and TfS <20%
Group 2: ferritin >100 ng/mL and TfS >20%
Observation period: 1 year
Frequency of septicaemia in Group 2 was 2.5-fold higher than in Group 1
Too much iron may be harmful in ACD!
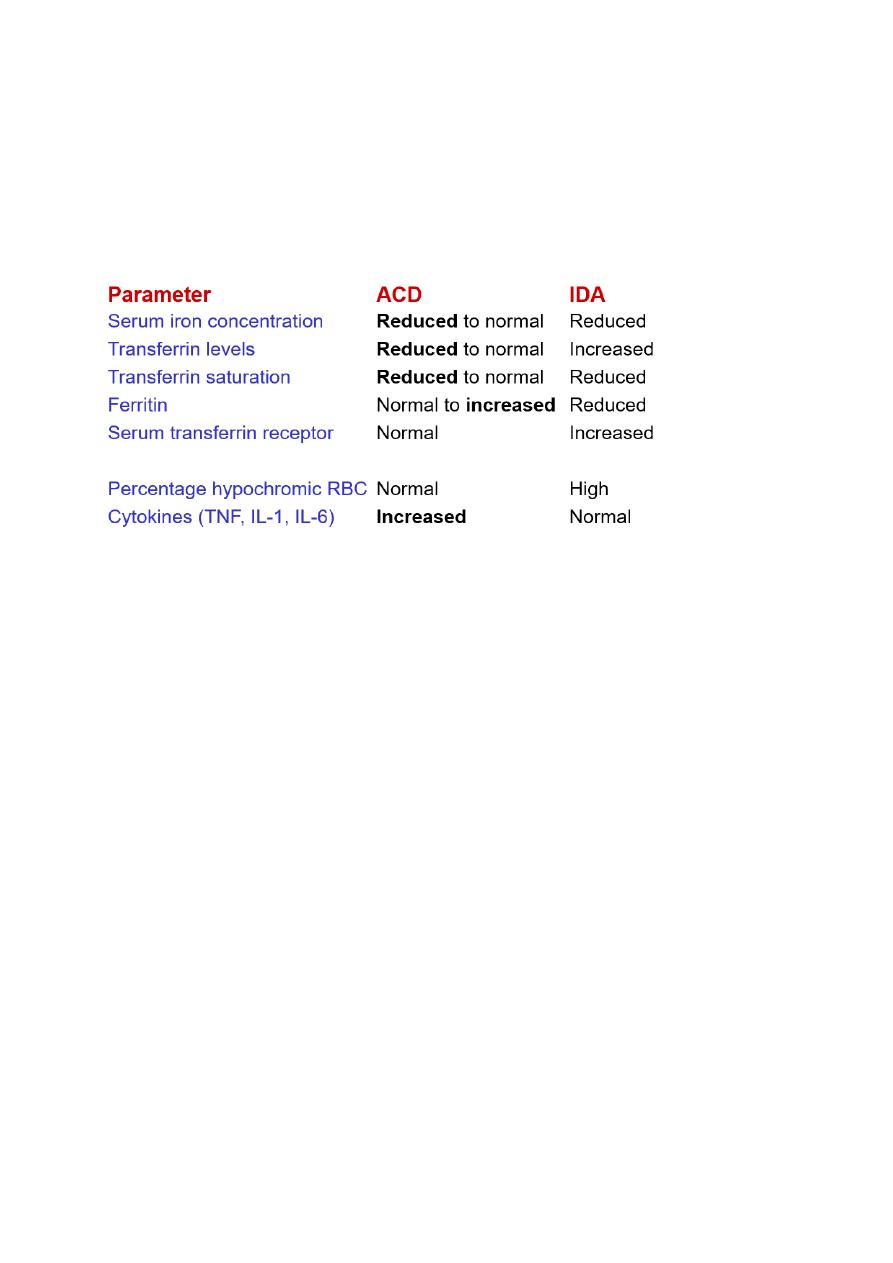
Why Is the Differential Diagnosis Between ACD and ACD + IDA Important?
Because these patients need contrasting therapies!!!
No iron in ACD
Iron needed in ACD/IDA
Therapy—Erythropoietin-Stimulating Agents (ESA)
Effective in increasing haemoglobin levels in ACD: patients with cancer, infections, and
autoimmune disorders
Response rate to treatment depends on underlying disease, stage, immune activation, and
iron availability
Increase of haemoglobin with ESA treatment is associated with a decreased need for blood
transfusions
Therapeutic End Points
Normalization of haemoglobin levels in end stage renal disease patients was associated
with a significant increase of cardiovascular mortality as compared with patients with
haemoglobin levels below the normal range
Dialysis patients: risk of death was highest with haematocrit levels between 33% and 36%
Avoid over-correction of anaemia (Hgb >12 g/dL)
Currently recommended therapeutic end point: Hgb 11–12 g/dL
Mubark A. Wilkins