1
ABNORMAL UTERINE BLEEDING
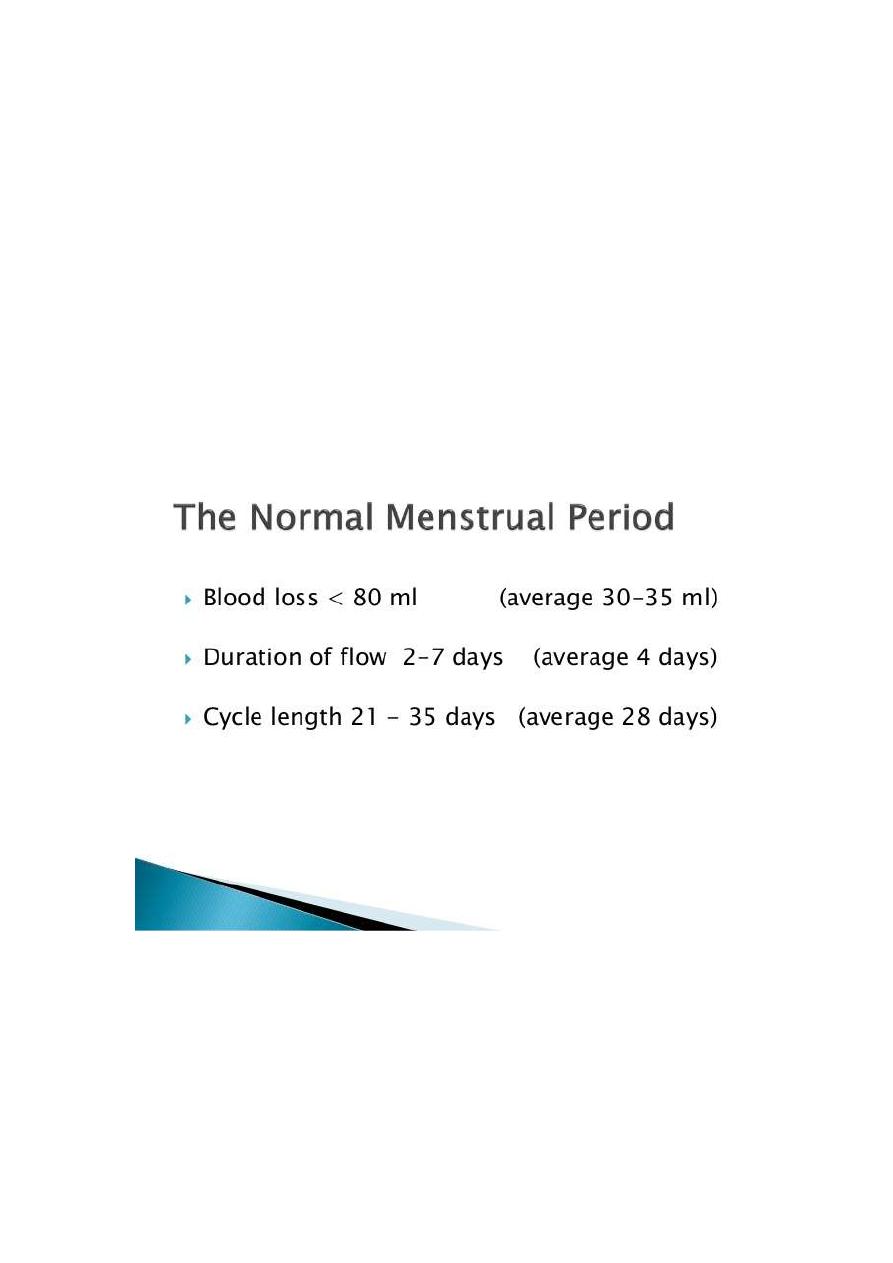
Definition: is a descriptive term applied to any alteration
in normal pattern of menstrual flow
. excessive flow
. prolong flow
. intermenstrual bleeding
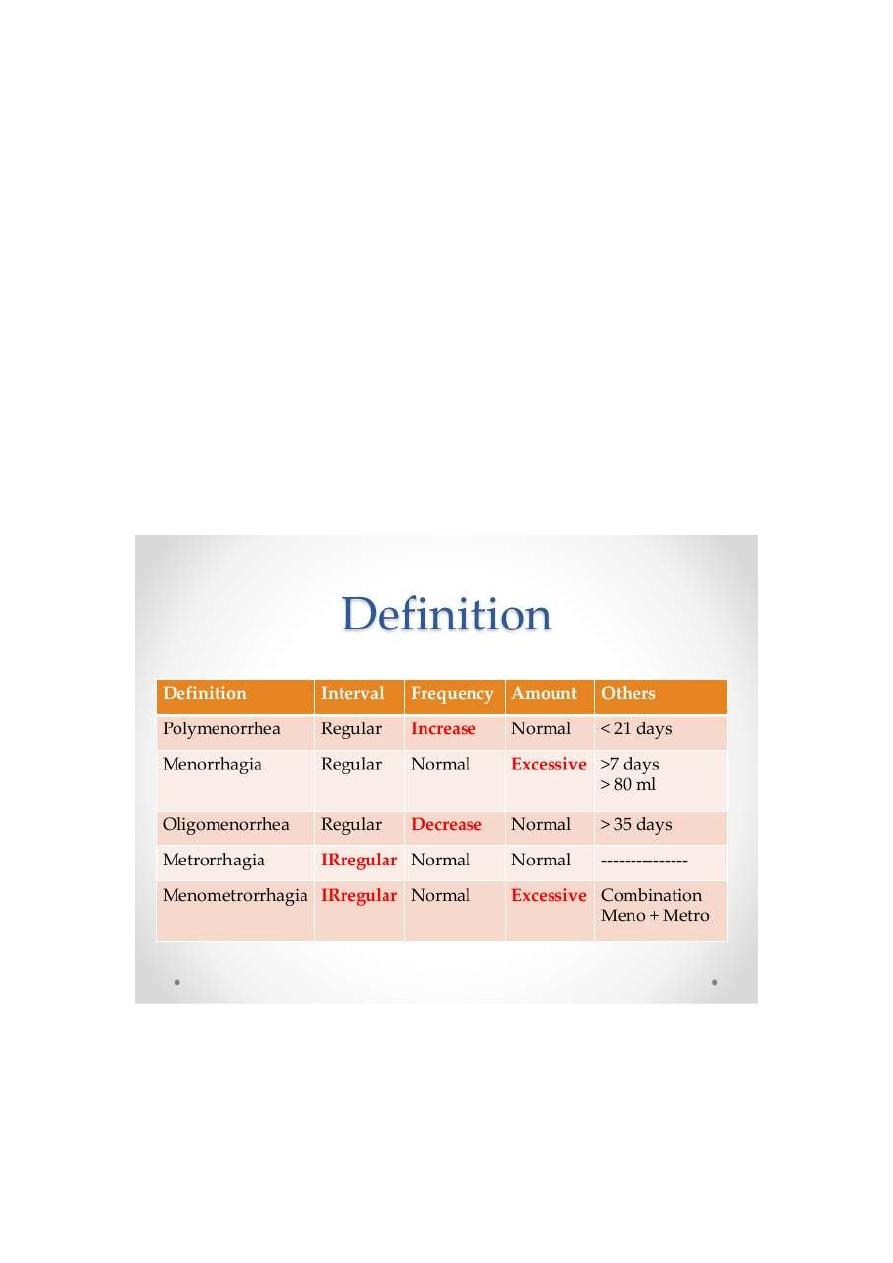
Classical nomenclature of abnormal uterine bleeding
Menorrhagia: prolonged and increased menstrual flow
Metrorrhagia: regular intermenstrual bleeding
2
Polymenorrhea: menses occurring at less than 21 days'
interval
Hypermenorrhea: excessive regular menstrual bleeding
Menometrorrhagia: prolong menses and intermenstrual
bleeding
Amenorrheore a absence of menstruation for more than
6 months
Oligomenorrhoea: menses at intervals of more than 35
days
AETIOLOGY
1.organic causes
3
2. non organic causes this is called dysfunctional uterine
bleeding (DUB)
ORGANIC CAUSES
A General causes
. psychological or emotional can lead to abnormal
bleeding through the effect on hypothalamus effecting
hormonal control of the ovary or it act on autonomic
nerves system supplying genital organ
. medication: exogenous steroid hormones neuroleptic.
anticoagulant and cytotoxic drugs
. endocrine disorder: abnormal thyroid function,
pituitary gland disorder, adrenal disorder, prolactin
disorder, Diabetes mellitus
. Disorder of hemostasis
. liver and renal disease
B local causes
. pregnancy complication: implantation bleeding, all
types of abortion, ectopic, trophoblastic disease
. congenital anomalies: double uterus increase surface
area

4
Traumatic: local internal or external injuries, ring
pessary
. IUCD
PID: either local endometritis or sever pelvic infection
may effect ovarian function and secondarily abnormal
menstruation
. hormonal producing tumor
. tumor of the uterus: benign fibroid common cause or
malignant endometrial carcinoma
.end cervical polyp or hyperplasia
Cervical carcinoma
Rarities such as arteriovenous malformation in the
uterus
NON ORGANIC CAUSES
. Known as dysfunction uterine bleeding
. any abnormal bleeding for which no organic cause can
be detected
. responsible for 50% of abnormal bleeding
. diagnosis by exclusion
. classified to: ovulatory & anovulatary causes

5
Anovulatory cause
. this tend to occur in woman at the extremes of
reproductive age and is typically irregular cycle .it is
more common in obese women
Threshold bleeding: estrogen produce in amount
enough to cause with drawl bleeding but not enough to
produce proper proliferative endometrium (thin hypo
plastic) this usually occur in adolescent and around
menopause
Cystic glandular hyperplasia is the condition in which
excessive and contiuos production of estrogen
producing proliferative endometrium progress to
hyperplasia so columnar epithelium become
hypertrophy and stroma also proliferate with polymorph
small haemorrgic area, necrosis and cystic dilation of the
gland keeping the appearance of Suisse cheese
appearance.
OVULATARY DUB
This pattern is more common in woman aged 35 – 45
and is typically regular heavy and often painful
menstruation
Corpus luteum defect :
.corpus luteum slow to degenerate this cause prolong
menstrual cycle and progesterone changes within the
6
endometrium continue for longer time and there is
premenstrual spoting
.corpus luteum slow to develop (corpus luteum
insufficiency )menstrual loss is prolong may last 15 days
MANGEMENT
History and examination
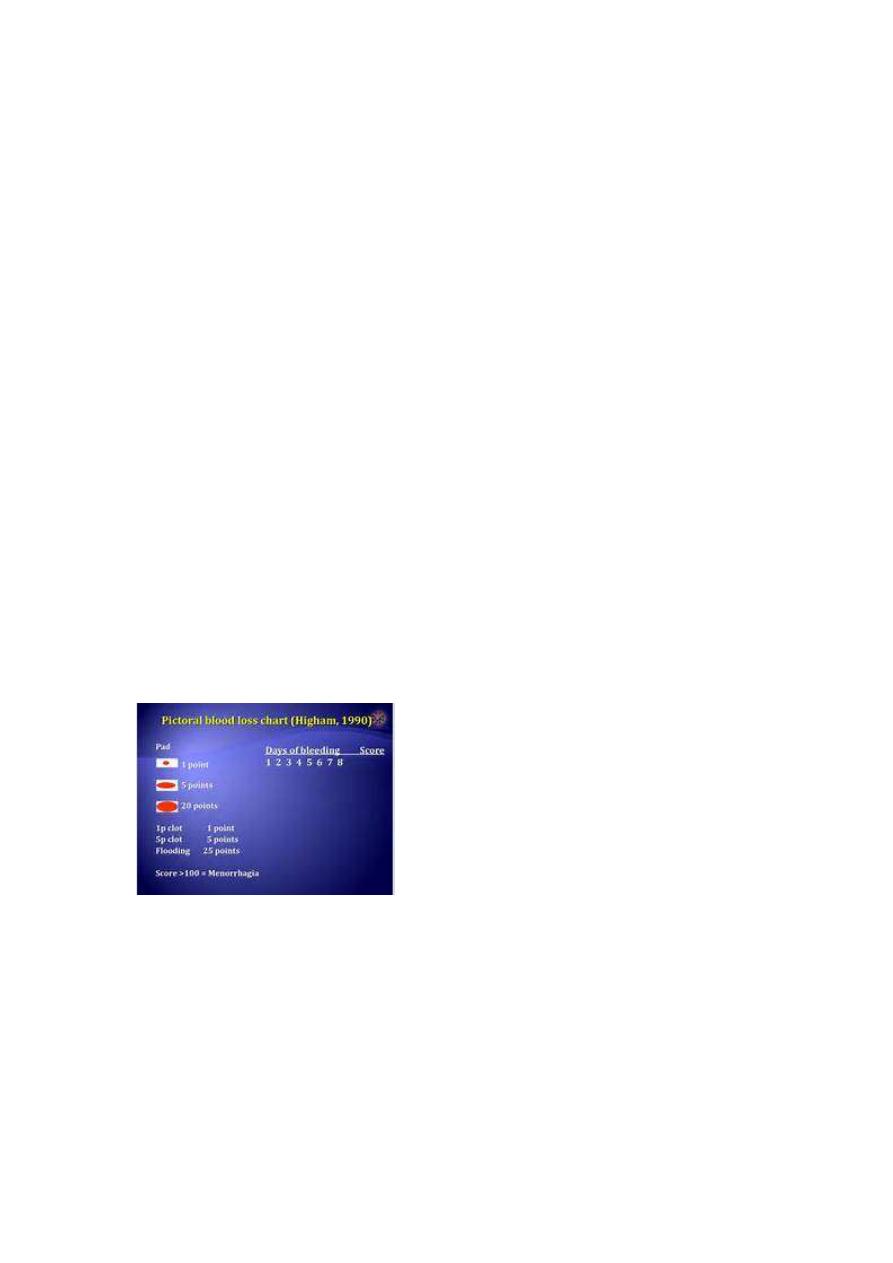
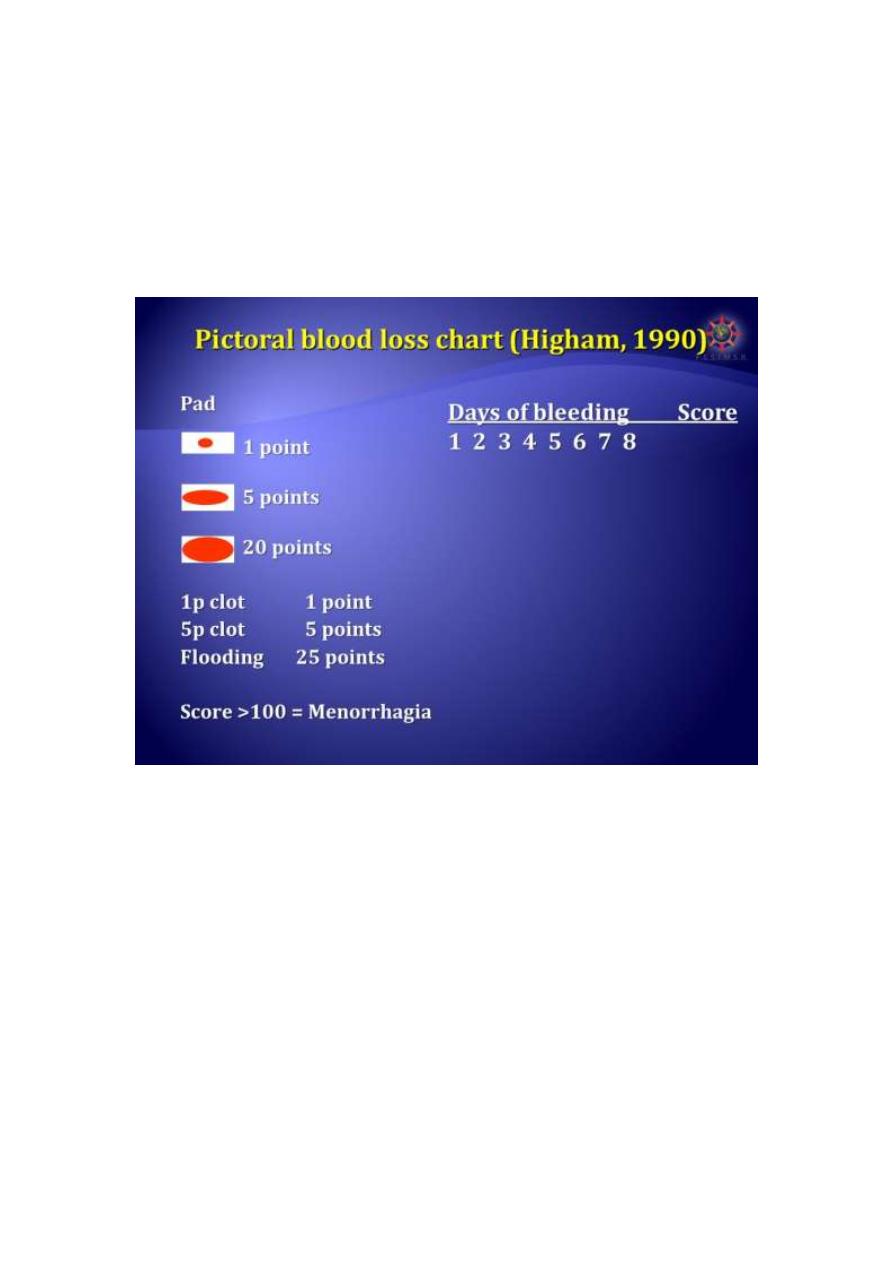
.Patients will have different idea about heavy period so
we have to confirm this is really heavy cycle
Soaked sanitary pad, presence of clots, blood spills over
cloths or bedding, take any time off work due to this
bleeding, treatment for anemia or blood transfusion
Type of abnormal bleeding whether continuous or
regular or intermenstrual bleeding …………………
Examination:
Sign of anemia, sign of endocrine or medical disease
that associated with heavy loss. abdominal and pelvic
examination, cervix is visualized for polyp or carcinoma,
cervical smear and swab

7
INVESTIGATIONS
. full blood count: assess severity and ascertain the need
for treatment iron therapy or even blood transfusion
. coagulation screen: especially if history consistent with
coagulation disorder
. pelvic ultrasound: mass fibroid, polyp, drug failure,
endometrial thickness ,…………
. high vaginal and endocevical swab
. endometrial biopsy: should be performed
If age more than 45, irregular or intermenstrual
bleeding, drug therapy has failed
Biopsy is performed either through outpatient Pipelle
Dilation and curettage
Outpatient hysteroscopy
Thyroid function test
Treatment
.for some woman ,the demonstration that their blood
loss in fact normal may be sufficient to reassure them
and make further treatment unnecessary
.when selecting appropriate management for the
patient ,it is important to consider and discuss :.patients
preference of treatment
.risk \benefit of each treatment
8
.contraceptive requirement complete family or not
.past medical history
.any contra indication to medical therapy
.suitability of anesthetic
MEDICAL TREATMENT:
Mefenamic acid and other NSAIDs
.reduce blood loss of 20 25 percent
.effective analgesia
.a number of contra indication like DU and asthma
Recommended dose 500 mg tds
Tranexamic acid
.reduction blood loss by 50 percent
.recommended dose 1 g qds to be taken when
menstruating heavily
Combined oral contraceptive pills
.benefit double up as very effective contraceptive
.limited by side effect and contra indications ,age
smoking ,obesity and family history
Norethisterone:
9
.cyclical from day 6 to day 26 of menstrual cycle
5 – 10 mg tds
Effective ,oral use but can cause break through bleeding
Levonogestrel intrauterine system (mirena )
.reduce menstrual blood by 95 %
.effective contraceptive
.disadvantages irregular menses and break through
bleeding in the first 3 – 9 month after insertion
GnRH agonists
Act on pituitary to stop the production of estrogen
which result in amenorrhea
.for short term use because its used limited due to hypo
estrogenic state and can cause flushing and sweating
.use for maximum 6 month unless addback HRT
.effective in reducing dysmenorrhea
.can cause irregular bleeding
Dose Zoladex 3.6 mg monthly or Decapeptyl 3 mg
monthly
SURGICAL TREATMENT
.failure of medical treatment
.complete family
10
Endometrial ablation
.destructive procedures employ the principle that
ablation of endometrial lining of the uterus to sufficient
depth prevents regeneration of the endometrium
.reduction blood loss by 95 %
.different method either resection of endometrium
,thermal ablation ,balloon thermal ablation ,microwave
ablation
Hysterectomy
KEY POINT
. PREGNANCY SHOULD ALWAYS BE CONSIDERED AND
EXCLUDED
. CONTRACEPTIVE HISTORY IS VITAL
. REGULAR BLEEDING USUALLY INDICATE HORMONAL
OR SYSTEMIC CAUSE WHILE IIREGULAR BLEEDING
INDICATE LOCAL CAUSE
. PATIENT AGE IMPORTANT AND MAY REFLECT THE
UNDERLYING CAUSE
. EXTREME REPRODUCTIVE AGE USUALLY BENIGN AN
OVULATORY DUB WHILE MIDDLE AGE USUALLY BENIGN
ORGANIC PATHOLOGY AND IF DUB USUALLY
OVULATORY TYPE
11
. COAGULATION DEFECT SHOULD BE EXCLUDED IN ANY
ADOLECENT WITH ABNORMAL BLEEDING CAUSING
SIGNIFICANT ANEMIA OR FAMILY HISTORY OF BLEEDING
TENDANCY
.