ECTOPIC PREGNANCY
DEFINITIONAny pregnancy where the fertilised ovum gets implanted & develops in a site other than normal uterine cavity.
INCIDENCE >1 in 100 pregnancies.
Recent evidence indicates that the incidence of ectopic pregnancy has been rising in many countries.USA-5 fold
UK-2 foldFrance 15/1000 pregnancies
India-1in100 deliveriesRecurrence rate - 15% after 1st, 25% after 2 ectopics
AETIOLOGY
Any factor that causes delayed transport of the fertilised ovum through the fallopian tubes.
Fallopian tube favours implantation in the tubal mucosa itself thus giving rise to a tubal ectopic pregnancy.
These factors may be Congenital or Acquired.
CONGENITAL - Tubal Hypoplasia, Tortuosity, Congenital diverticuli, Accessory ostia, Partial stenosisACQUIRED -
Inflammatory: PID, Septic Abortion, Puerperal Sepsis, MTP (intraluminal adhesion)Surgical: Tubal reconstructive surgery, Recanalisation of tubes
Neoplastic: Broad ligament myoma, Ovarian tumourMiscellaneous Causes: IUCD, Endometriosis, ART (IVF & & GIFT),
Previous ectopic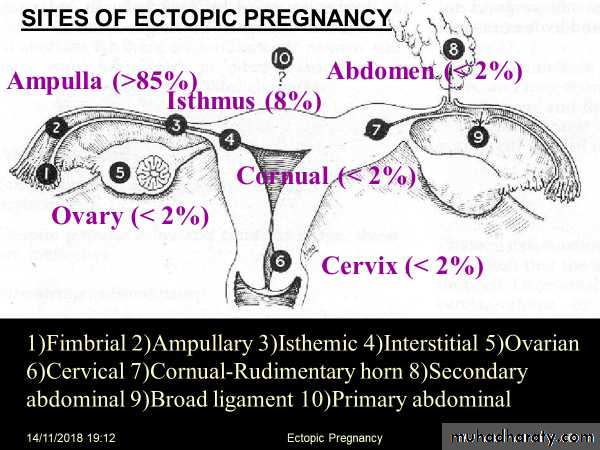
CLINICAL PRESENTATION
Ectopic Pregnancy remains asymptotic until it ruptures when it can present in two variations - Acute &. ChronicSYMPTOMS:
AmenorrheaAbdominal Pain
SyncopeVaginal Bleeding
Pelvic MassTubal Pregnancy
Commonest site of ectopic pregnancy (99%) and The ampulla is the most frequent location of implantation (64%).
Symptoms:
Onset occurs ~7 weeks after LMPAbdominal pain
Vaginal bleedingSigns:
Abdominal tenderness (91%)1st trimester bleeding (79%)
Common associated findings:Adnexal tenderness (54%), Amenorrhea
Early pregnancy symptomsCullen’s sign (Periumbilical bruising)
Nausea, vomiting, diarrhea, dizziness
Other Signs:Tachycardia, Low grade fever
Hypoactive bowel soundsCervical Motion Tenderness
Enlarged uterusTender pelvic or adnexal mass
Cul-de-sac fullnessDecidual cast (Passage of decidua in one piece)
Signs suggestive of ruptured ectopic pregnancy:Usually between 6- and 12-weeks gestation
Severe abdominal tenderness with rebound, guarding
Orthostatic hypotensionDifferential Diagnosis
AppendicitisThreatened Abortion
Ruptured ovarian cystPID
SalpingitisEndometritis
NephrolithiasisOvarian torsion
Intrauterine pregnancy
Alternative diagnoses:Dysmenorrhea
Dysfunctional uterine bleedUTI
Diverticulitis
Mesenteric lymphadenitisMETHODS OF EARLY DIAGNOSIS:
Immunoassay utilising monoclonal antibodies to beta HCGUltrasound scanning – Abdominal & Vaginal including Colour Doppler
Laparoscopy
Serum progesterone estimation not helpfulA combination of these methods may have to be employed.
At 4-5 weeks-TVS can visualise a gestational sac as early as 4-5 weeks from LMP.
During this time the lowest serum beta HCG is 2000 IU/Lt.When beta HCG level is greater than this and there is an empty uterine cavity on TVS, ectopic pregnancy can be suspected.
In such a situation, when the value of beta HCG does not double in 48 hours ectopic pregnancy will be confirmed.
The USG features of ectopic pregnancy after 5 weeks can be any of the following-
Demonstration of the gestational sac with or without a live embryo (Begel’s sign) - The GS appears as an intact well-defined tubal ring by 6 weeks when it measures 5 mm in diameter. Afterwards it can be seen as a complete sonolucent sac with the yolk sac and the embryonic pole with or without heart activity inside.Poorly defined tubal ring possibly containing echogenic structure and POD typically containing fluid or blood.
Ruptured ectopic with fluid in the POD and an empty uterus.
(here methods of early diagnosis end)INVESTIGATIONS-
Laboratory/Chemical test –Serial quantitative beta HCG level by RIA
Serum progesterone level (<5 mg/ml in ectopic pregnancy)Low levels of Trophoblastic proteins such as SPI and PAPP-, Placental protein 14 & 12
USG- usually haematocele is foundLaparoscopy
Initial InvestigationsMonitor βhCG levels
βhCG- hormone produced by the placenta (and fetal kidney)
Detectable in plasma and urine following blastocyst implantationBlood levels rise rapidly, doubling every 2d and plateaus at 8-10 weeks gestation
Serum βHCG levels correlate with the size and gestational age in normal embryonic growthβHCG with inadequate increase may suggest ectopic pregnancy
** β-hCG level does not predict ruptured ectopic, ruptured ectopic may occur at anyβ-HCG level
MANAGEMENTDepends on the stage of the disease and the condition of the patient at diagnosis.
Options: -Surgery – Laparoscopy / Laparotomy
Medical – Administration of drugs at the site / systemically
Expectant – ObservationMANAGEMENT OF ACUTE ECTOPIC PREGNANCY
HospitalisationResuscitation -
Treatment of shockLie flat with the leg end raised
AnalgesicsBlood transfusion
Laparotomy should be done at the earliest.Salpingectomy is the definitive treatment.
(No benefit from removing Ovary along with the tube)
OptionsSURGICAL-
SURGICALLY ADMINISTERED MEDICAL (SAM) TREATMENTMEDICAL TREATMENT
EXPECTANT MANAGEMENTMEDICAL TREATMENT WITH METHOTREXATE
Ectopic pregnancy size should be < 3.5 cm.Can be given IV/IM/Oral, usually along with Folinic acid
Recent concept is to give Methtrexate IM in a single dose of 50 mg/m2 without Folinic acid. If serum HCG does not fall to 15% within 4-7 days, then a second dose of Methtrexate is given and resolution confirmed by HCG estimationAdvantages
Minimal Hospitalisation. Usually outdoor treatment
Quick recovery90% success if cases are properly selected
DisadvantagesSide effects like GI & Skin
Monitoring is essential- Total blood count, LFT & serum HCG once weekly till it becomes negativeEXPECTANT TREATMENT
Today only selected cases are managed expectantly, screened and identified by high resolution ultrasound scanner and monitored by serial serum HCG assayCriteria for this management:
initial HCG less than 250 I.U plus other criteria for medical treatmentIt has high success rate reaching 70-80%.