
Dermatology
Dr. Ahmed Abdulhussein Alhuchami
2018
Genital Ulcer
Causes:
ST causes: herpes genitalis, chancre (primary syphilis), chancroid, lymphogranuloma
venereum (LGV), and granuloma inguinale (Donovanosis).
Non ST causes: Behcet disease, fixed drug eruption, trauma, malignancy as SCC, and
chronic infections as TB.
Syphilis
Definition:
Syphilis is a STI caused by a spirochetal bacterium, Treponema pallidum, also called
"Lues" or "Cupid's disease
(Roman mythology god of love
)".
Mode of Transmission:
The infection is usually acquired through sexual contact with infected lesions or body
fluids; less commonly, transplacentally; and rarely through blood transfusion, or
inoculation with contaminated instruments (as tattooing or IV drug users).
Microbiology:
Treponema pallidum is a Gram negative, fragile, spiral bacterium (spirochete) with
corkscrew rotation motility. It can be observed only by dark-field microscope, and
unable to be cultured in vitro.
T. pallidum can cause the following diseases:
1. Syphilis: caused by T. pallidum pallidum.
2. Bejel (endemic syphilis): caused by T. pallidum endemicum. Transmitted non
sexually, and has features of secondary syphilis without presence of the primary stage.
Bejel is endemic in some areas in Saudi Arabia, Iraq, and Syria.
3. Yaws: caused by T. pallidum pertenue. It is a tropical disease characterized by an
infection of the skin, bones, and joints.
4. Pinta: caused by T. pallidum carateum (vitiligo-like presentation).
Classification and Stages:
There are two types of syphilis congenital and acquired.
The Acquired Syphilis passes through four distinct clinical stages:
1. Primary stage (chancre).
2. Secondary stage (skin, mucous membrane, and systemic eruption).
3. Latent stage (history of syphilis + absence of signs and symptoms + positive
serology).
It is divided into early latent (less than one year) and late latent (1 year or longer).
4. Tertiary stage (skin, mucous membrane, and visceral).
Early syphilis (within the first 2 years of infection, more infectious) including the
primary, secondary, and early latent stages.
Late syphilis (after 2 years of infection, less infectious) including late latent and tertiary
syphilis.
1
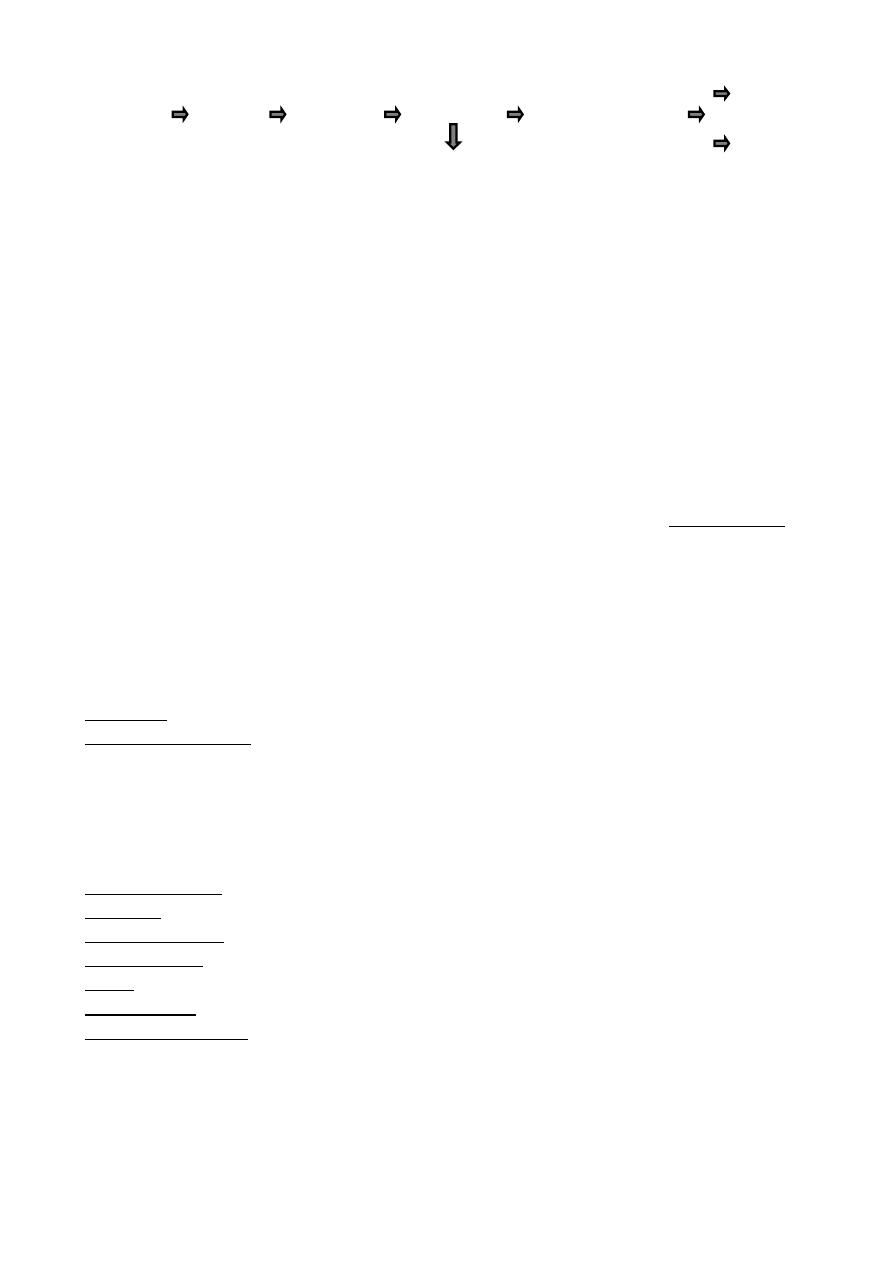
Natural Course of Untreated Syphilis:
50% 50% 75% (1/3) Remission
Exposure Primary Secondary Early latent Late latent (1/3) Remain latent
(1/3) Tertiary
Relapse to Secondary
25%
A- Acquired Syphilis:
Primary Syphilis
(Chancre)
:
The syphilitic ulcer (chancre) appear in the genital area after 9-90 days (3 weeks in
50%) after exposure to infected partner at the site of initial contact. Chancre is usually
solitary, painless, hard, and indurated; the base is clean with a scant yellow serous
discharge (typical chancre occur in 50% of patients). Extragenital chancres accrue in 5%
of cases. The chancre usually heals with scarring after 3-6 weeks.
Painless, hard, discrete regional lymphadenopathy occurs in 1-2 weeks; which never
coalesce or suppurate unless there is mixed infection.
Secondary Syphilis:
I- Cutaneous findings: most eruptions are macular and/or papular; nodular, follicular,
and pustular eruptions occur infrequently.
The skin changes of syphilis can mimic many other skin diseases "great imitator", but
the lesions of secondary syphilis have certain characteristics that differentiate them:
1. There is little or no fever at onset.
2. Pain or itching is minimum or absent.
3. Lesions are non inflammatory, develop slowly.
4. There is a marked tendency to polymorphism.
5. Usually bilateral symmetrical, with characteristic palms and soles involvement.
6. The color is characteristic, resembling a "clean-cut ham" (coppery tint).
Hair loss: small irregular patches of hair loss ("moth eaten" alopecia).
Malignant syphilis: wide spread lesions that become necrotic and ulcerated, associated
with toxicity, fever, arthralgia. Most patients are immunocompromised.
II- Mucous membrane findings: are extremely infectious, including: codylomata lata
(smooth, papillated, or covered with cauliflower-like vegetations), oral mucous patches,
pharyngitis and laryngeal involvement which may produce hoarseness.
III- Systemic findings:
Ophthalmologic: iritis, is the most common eye complication.
Auditory: sensorineural hearing loss.
Musculoskeletal: back pain, arthralgias, arthritis, tenosynovitis, and bursitis.
Haematologic: anaemia, leukocytosis, relative lymphopenia, and elevated ESR.
Renal: acute membranous glomerulonephritis.
Neurological: asymptomatic or symptomatic (headache and meningeal irritation).
Hepatic and gastric.
Differential Diagnosis of Secondary Syphilis:
Skin eruption: pityriasis rosea, guttate psoriasis, lichen planus, pityriasis versicolor,
drug eruptions, and viral eruptions.
Condylomata lata: genital warts, and haemorrhoids.
Oral lesions: aphthous ulcers, and candidiasis.
Alopecia "Moth eaten": alopecia areata, and tinea capitis.
2
Tertiary Syphilis:
I- Cutaneous lesions: in opposite to the secondary syphilis; the lesions are few,
asymmetrical, slowly growing, destructive and heals with scar, and this stage is less
infectious and the microorganisms are few within these lesions.
They can be divided into 2 types:
1. Nodular and noduloulcerative lesions: may be psoriasiform.
2. Gummas (a form of granuloma): are non-tender pink to dusky-red nodules or plaques.
They favor sites of previous trauma, scalp, and forehead, but may arise anywhere in the
body.
II- Mucous membranes lesions: Discrete gummas or diffuse gummatous infiltration
may involve mucous membranes, especially the palate, nasal mucosa, tongue, tonsils,
and pharynx. The lesions ulcerate and are disfiguring. Destruction of the nasal cartilage
and bone (saddle nose) are the disease hallmark. Oral leukoplakia may occur, and may
progress to SCC in 50% of cases.
III- Visceral (systemic findings): cardiovascular syphilis and neurosyphilis
{asymptomatic or symptomatic (headache, fever, stiff neck, confusion, and seizures)}.
B- Congenital Syphilis:
T.pallidum can be transmitted to the fetus in utero from an infected mother (usually
with early syphilis), this transmission usually occurs after the forth month of gestation.
The ability of the mother to infect the fetus diminishes with further pregnancies.
Approximately 25% of infants from mothers with untreated primary or secondary
syphilis die in utero. Of those infants born (75%), one-half develop the disease,
one-forth are seropositive without clinical manifestations, and one-forth are not
infected.
Congenital syphilis divided into:
Early: presenting within the first 2 years of life (usually after the third week).
Late: presented after the age of 2 years.
Stigmata of Congenital Syphilis:
1. Ophthalmic: corneal clouding.
2. Oral: Hutchinson teeth (notched, peg-shaped upper incisors) and high-arched palate.
3. Nose: saddle nose.
4. Orthopedic: frontal bossing, saber shin, and thickened medial clavicle.
5. Neurologic: 8
th
cranial nerve palsy.
6. Positive serology for syphilis.
3
Diagnosis of Syphilis:
1. History and examination.
2. Dark-field microscopy: in which the specimen (usually taken from the base of a
chancre) appears bright against a dark background. Mostly useful in early disease
when the serological tests still negative.
3. Serological tests.
4. PCR.
5. Biopsy: rarely needed.
Serological Tests of Syphilis
: classified into two main groups:
A- Non-specific (lipoidal or non treponemal) tests:
These tests are directed against the phospholipids in the cell wall of the microorganisms,
including two important tests:
1. Venereal disease research laboratory (VDRL).
2. Rapid plasma regain (RPR) tests.
These tests become positive 3-6 weeks after infection (after 3 weeks in 50%).
Remain strongly positive throughout the secondary phase, and usually become
negative after treatment, so can be used to monitor response to therapy
and follow up.
They are used for screening purposes and have a high degree of sensitivity but
relatively low specificity.
These tests give quantitative as well as qualitative results, so all reactive samples are
titrated to determine the highest reactive dilution. A fourfold change in titer is
considered significant clinically.
When these tests are positive, verification should be done by the specific tests.
B- Specific (treponemal) tests:
These tests are directed against the treponaeml antigens include:
1. T. pallidum haemagglutination test (TPHA): available in Iraq.
2. Reiter protein complement fixation test (RPCF).
3. Fluorescent treponemal antibody absorption test (FTA/ABS).
4. T. pallidum immobilization test (TPI).
These tests become positive earlier than the non specific tests.
A patient who has a reactive treponemal test usually will have a reactive test for a life
time, regardless of treatment or disease activity, so these tests should not be used to
assess response to treatment or follow up.
They are not used for screening purposes.
These tests cannot be titrated.
False reactions:
False-positive reactions: (positive non-specific test with negative specific test), may
occur with collagen vascular disease, advancing age, narcotic drug use, chronic liver
disease, several chronic infections such as TB, and several acute infections such as
herpes.
False-negative reactions: may occur if the patient has been used topical or systemic
antibiotics, or due to Prozone phenomenon (caused by excessive amount of antibody).
4
Treatment of Syphilis:
Penicillin remains the treatment of choice for all stages of syphilis.
Early syphilis:
Single IM injection of 2.4 Million U benzathin penicillin G, if penicillin allergic,
doxycycline 100 mg orally twice daily for 2 weeks.
Late syphilis:
IM injection of 2.4 MU benzathin penicillin G once a week for 3 weeks, if penicillin
allergic, doxycycline 100 mg orally twice daily for one month.
Congenital syphilis:
Crystalline penicillin G 200 000 U/Kg/d IV or 50 000 U/6h IM for 10-14 days.
Sexual partner(s) should be treated.
No proven alternatives to penicillin are available for treating:
1. Neurosyphilis.
2. Congenital syphilis.
3. HIV infected patient.
4. Pregnant patient.
These patients should be skin tested and desensitized if the test is positive.
Jarisch-Herxheimer Reaction: a complex allergic response to antigens released from
dead microorganism can complicate the treatment of syphilis. A transient acute febrile
reaction with head ache and myalgia may develop within 24 hours of therapy. It occurs
in of 50% of patients with early syphilis.
Follow Up:
All patients should be followed after treatment, this done by clinical examination and
by measuring the VDRL titer (a 4 fold decrease in titer suspected after 6 months of
therapy), as follows:
Early syphilis:
1. Every 3 months in the 1
st
year.
2. Every 6 months in the 2
nd
year.
3. Yearly thereafter.
Late syphilis: yearly.
Neurosyphilis: every 6 months by measuring the blood and CSF level.
Signs of Relapse:
1. Clinical.
2. Serological (4 fold increase).
3. Transplacental infection.
4. Infection of the partner.
5
Chancroid
It is a common and endemic in many of the world's poorest regions such as areas of
Africa, and Asia, but it is rare in Iraq. It is caused by haemophilus ducreyi which is short
gram negative bacillus.
Clinical Features:
In reverse to chancre, the ulcer of chancroid is painful, tender, deep, soft, bleed easily
with purulent base, with short IP (3-5 days). Multiple ulcers appear on the genitalia from
autoinoculation (highly infectious ulcer).
Usually heal with scarring after months.
Unilateral or bilateral painful inguinal lymphadenopathy (which may matted together)
develops in about 50% of patients.
Investigation:
Smear: the gram negative bacilli are usually found in small clusters or parallel chains of
two or three organisms (the "school-of-fish" pattern).
Culture: using modified Muller-Hinton agar.
Treatment:
Single dose of azithromycin 1 gm orally, or cefriaxone 250 mg IM; or erythromycin 500
mg orally four times daily for 7 days.
"Best Regards"
6