Lectures in Community Medicine
family planning
Motto of family planning
•Having children by
choice not by chance
Facts
-The perfect method does not exist
-Contraceptives methods change based on the
clients circumstances
-30% of married and 61 % of unmarried females(in
the west) change methods within 2years
-Careful consideration of all factors can help a
woman choose the best method
Waiting
until the mother is at least
18
years old before
trying to have children improves maternal and child health.
If additional children are desired after a child is born, it is
healthier for the mother to
wait at least 2 years
after
the previous birth before attempting to conceive (but not
more than
5
years).
After a miscarriage or abortion, it is healthier to
wait at
least 6 months.
When planning a family
women who are over the age
of
35
should be aware of
the risks of having a child at
that age.
Older women are at a higher risk of having a child with
autism and Down syndrome
, the chances of
having
multiple births
increases, which cause further
late-pregnancy risks, they have an increased chance of
developing
gestational diabetes
, the need for a
Caesarian-section
is greater, older women's bodies
are not as well-suited for delivering a baby. The risk of
prolonged labor
is higher. Older mothers have a
higher risk of a long labor, putting the baby in distress.

Family
Planning
W H O
A way of thinking and living
that is adopted voluntarily,
upon the basis of knowledge
,attitudes and responsible
decisions by individuals and
couples…..
in order to…
Promote the health and
welfare of the family group
and thus contribute
effectively to the social
development of a country
(WHO 1971)

Globally….
Family planning is among the most cost-
effective of all health interventions

OBJECTIVES
To avoid
unwanted births
and to bring
about wanted
births (for the
sub fertile)
OBJECTIVES
To regulate the
intervals
between
pregnancies
(spacing)
OBJECTIVES
To control the
time at which
births occurs in
relation to the
ages of the
parents (timing)

OBJECTIVES
To determine
the number of
children in the
family (family
size)
SCOPE OF FAMILY PLANNING
SERVICES
1-
The proper
spacing and
limitation of
births
SCOPE OF FAMILY PLANNING
SERVICES
2-
Advice on
sterility
SCOPE OF FAMILY PLANNING
SERVICES
3-
Education for
parenthood
SCOPE OF FAMILY PLANNING
SERVICES
4-
Sex
education
SCOPE OF FAMILY PLANNING
SERVICES
5-
Screening for
pathological
conditions related to
the reproductive
system (e.g. cervical
cancer)
SCOPE OF FAMILY PLANNING
SERVICES
6-
Genetic
counselling
SCOPE OF FAMILY PLANNING
SERVICES
7-
Premarital
consultation and
examination

SCOPE OF FAMILY PLANNING
SERVICES
8-
Carrying out
pregnancy tests

SCOPE OF FAMILY PLANNING
SERVICES
9-
Marriage
counselling

SCOPE OF FAMILY PLANNING
SERVICES
10-
The preparation of
couples for the
arrival of their first
child

SCOPE OF FAMILY PLANNING
SERVICES
11-
Providing services
for unmarried
mothers

SCOPE OF FAMILY PLANNING
SERVICES
12-
Teaching home
economics and
nutrition

SCOPE OF FAMILY PLANNING
SERVICES
13-
Providing
adoption
services
F
Family Planning
Services..
Definition

• Family planning services are
defined as "educational,
comprehensive medical or social
activities which enable
individuals, including minors, to
determine freely the number
and spacing of their children and
to select the means by which
this may be achieved."
IMPACT OF
FAMILY
PLANNING
WOMEN’S
HEALTH
i-Avoidance of
Unwanted
Pregnancies
An unwanted pregnancy
may lead to an induced
abortion. Abortion
outside the medical
setting (criminal
abortion) is one of the
most dangerous
consequences. There is
also evidence of higher
incidence of mental
disturbances among
mothers who have had
unwanted pregnancies

WOMEN’S
HEALTH
ii- Limiting the
number of
births and
proper spacing
Repeated
pregnancies
increases the risk of
maternal mortality
and morbidity.
These risks rise with
each pregnancy
beyond the
third
and increase
significantly beyond
the
fifth.
With increased parity
the following increase:
1- Rupture of the uterus
2- Uterine atony
3- Toxaemia
4- Eclampsia
5- Placenta previa
6- Nutritional anaemia
7- Stillbirths
8- Cancer of the cervix..
family planning is the
only way to limit the
size and control the
interval between births
WOMEN’S
HEALTH
iii-Timing
of births
Generally
mothers face
greater risk of
death below
20 and above
30-35.
IMPACT
OF
FAMILY
PLANNING
ON…….
FOETAL HEALTH
A number of
congenital
anamolies are
associated with
advanced
maternal age
which can be
avoided by timing
pregnancy in
relation to
maternal age.
CHILD HEALTH
A- Child mortality: It is
well known that this
increases if pregnancies
occur in rapid
succession. A birth
interval of 2-3 years is
considered desirable to
reduce child mortality.
• B- Child growth,
development and
nutrition: The child is
not likely to receive his
full share of love and
care, including
nutrtional needs
CHILD HEALTH
C- Infectious diseases:
Children living in large
sized families have an
increased risk of
infection especially
gastroenteritis
respiratory and skin
infections.
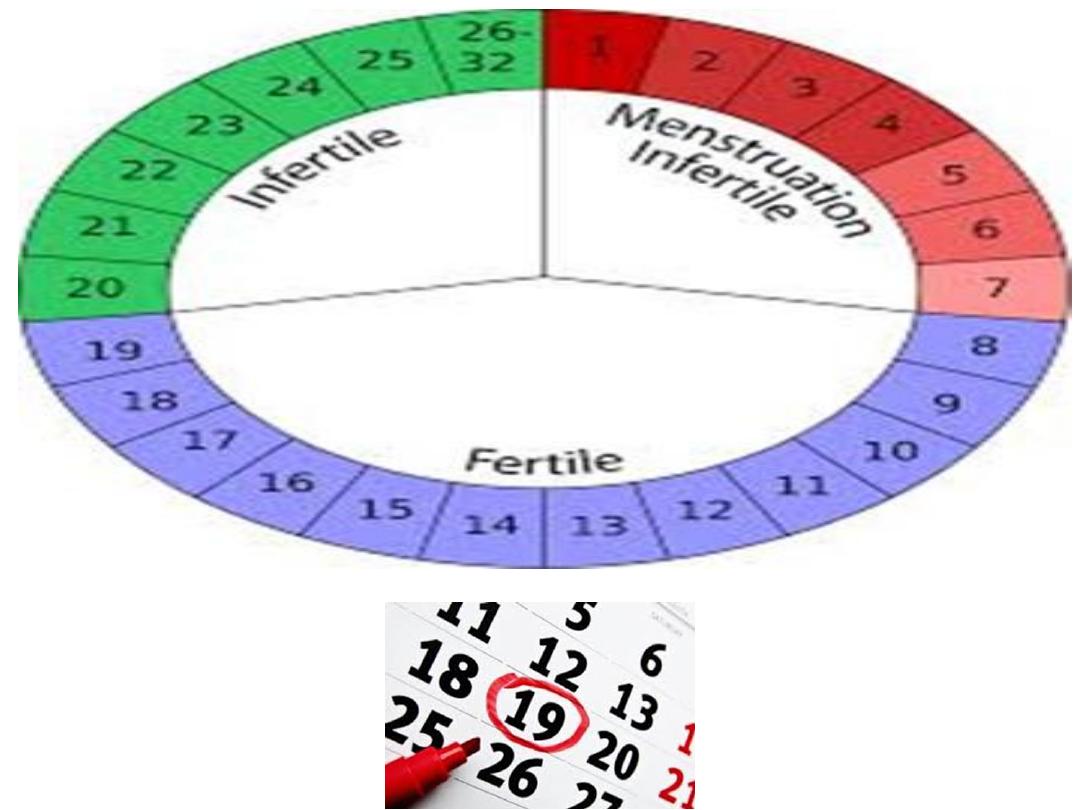
2-3
percent of the world’s
reproductive age population
depends on NFP which limits
sexual intercourse to naturally
infertile periods
.
BIRTH CONTROL -
CONTRACEPTION
Refers to methods or devices
used to prevent pregnancy.
Planning and provision of birth
control is the
essence
of family
planning.
BENEFITS OF CONTRACEPTION
Contraception in developing countries has cut
maternal deaths by 44% (270,000 deaths averted in
2008). Teenage pregnancies are at greatest risk of
adverse outcomes e.g. preterm birth, LBW & infant
mortality, thus adolescents need comprehensive sex
education and access to reproductive health
services, including contraception.
Birth control increases economic growth because of
fewer dependent children, more women
participating in the workforce, and less consumption
of scare resources. their children's schooling and
body mass index all substantially improve with
greater access to contraception.
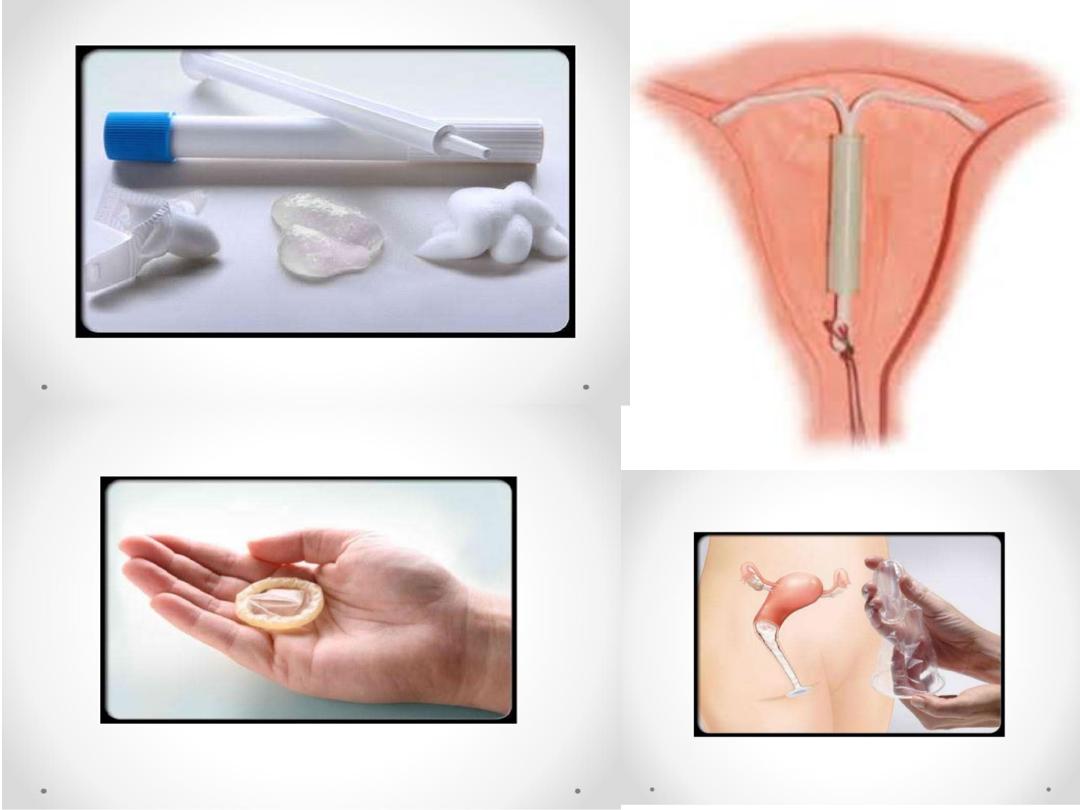
Birth Control Methods:
A- Barriers: such as condoms, diaphragms, and the
contraceptive sponge;
B- Hormonal contraception :includes oral pills,
patches, vaginal rings, and injectable contraceptives;
C- Intrauterine devices (IUDs).

e.g. transdermal patch


•Emergency contraception can
prevent pregnancy after
unprotected sex.
• Long-acting reversible
contraception such as implants,
IUDs, or vaginal rings are
recommended to reduce teenage
pregnancy.

eg. Split dose emergency
contrceptive pills
Chance of pregnancy during first year of use:
Method
Typical use
Perfect use
No birth control
85%
85%
Combination pill
8%
0.3%
Progestin-only pill
13%
1.1%
Sterilization (female)
0.5%
0.5%
Sterilization (male)
0.15%
0.10%
Condom (female)
21%
5%
Condom (male)
15%
2%
Copper IUD
0.8%
0.6%
Hormone IUD
0.2%
0.2%
Patch
8%
0.3%
Vaginal ring
8%
0.3%
Depo Provera
3%
0.3%
Implant
0.05%
0.05%
Diaphragm and spermicide
16%
6%
Withdrawal
27%
4%
Standard Days Method
~12-25%
~1-9%
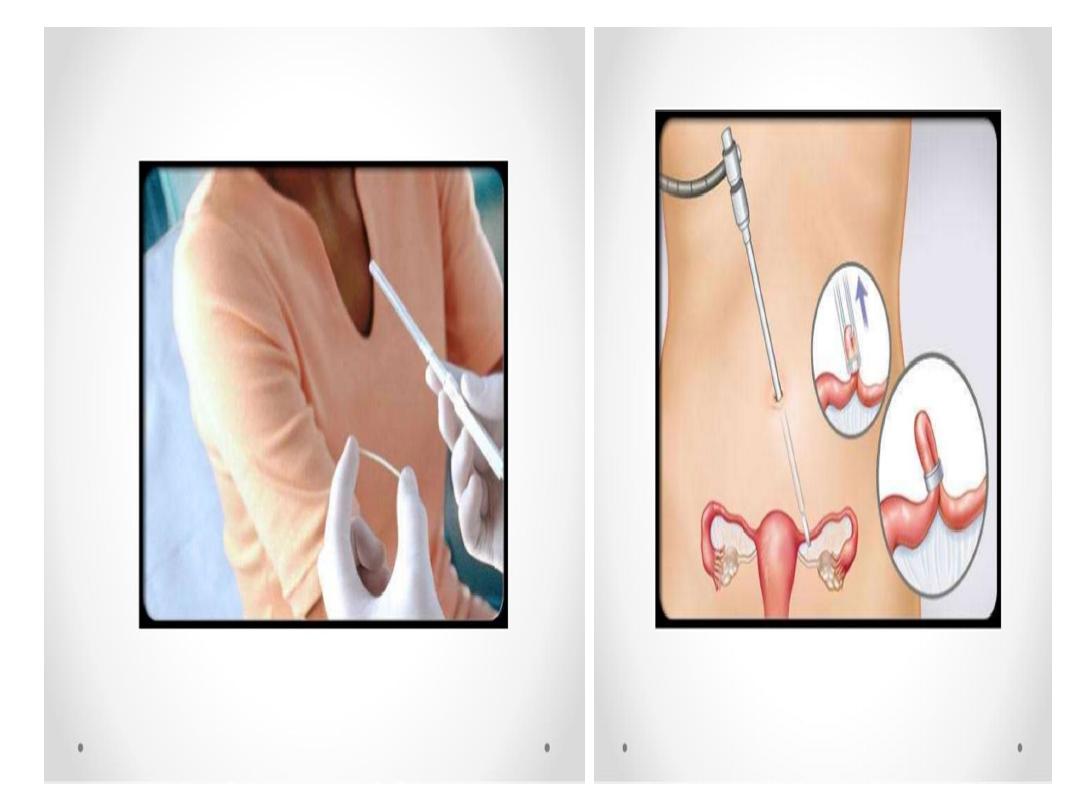
STERILIZATION
Sterilization by means such
as vasectomy and tubal
ligation is permanent
contraception
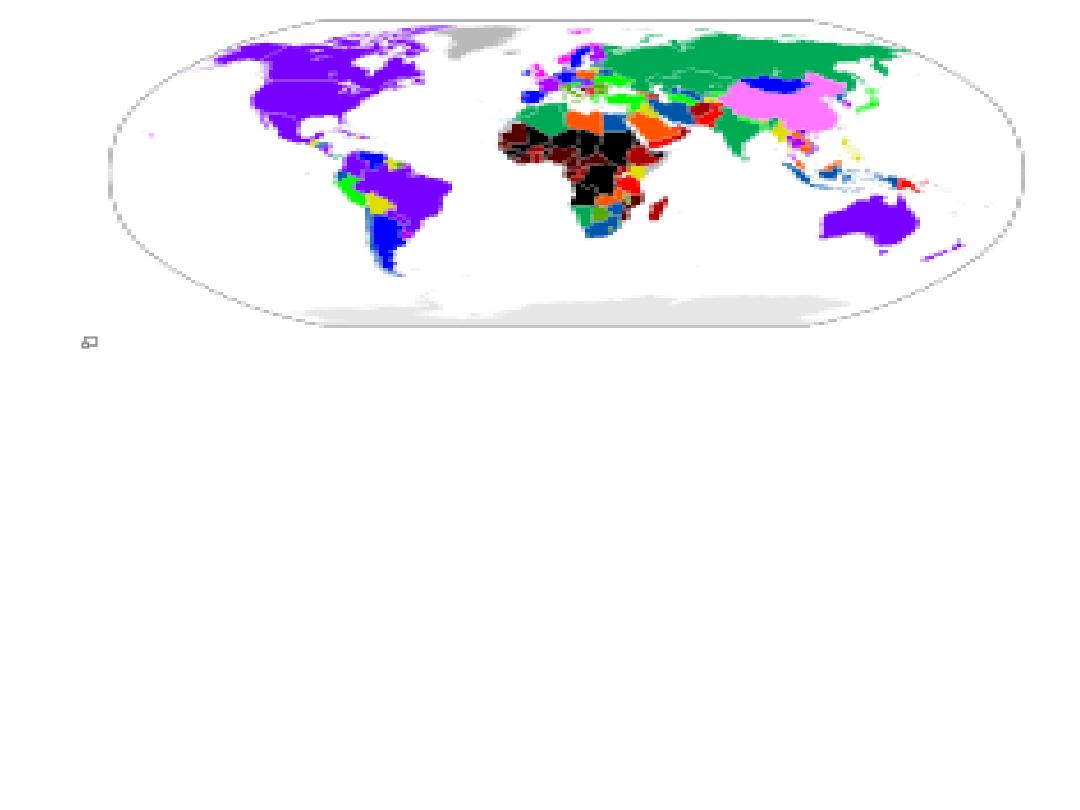
Percentage of
women using
modern
contraception:
Blue to pink :60-90%
Dark brown to
black:6-18%
FAMILY PLANNING IN IRAQ
• Barriers to birth spacing:
• 1-The influence of persons in the.
community(traditional ,religious).
• 2-Availability of variety of methods.
• 3-Accessibility of FP services.
• Cost.
Grounds on which abortion is permitted:
To save the life of the woman
Yes
To preserve physical health No
To preserve mental health No
Rape or incest
No
Foetal impairment Yes
Economic or social reasons No
Available on request
No
Additional requirements:
Approval from
THREE
physicians is needed in order to obtain a legal abortion
AND THIS SHOULD BE DONE IN A
STATE HOSPITAL
.
The
written consent
of the pregnant woman’s husband is also necessary.
The United Nations’ Children Fund (2010) states that
through 2005 and 2009, contraceptive use in Iraq was
at
50%
. This is because a majority of Iraqi women
are unaware of Iraq’s national policy and how to
access health facilities and obtain contraceptives.