GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
Congenital anomalies of the esophagus:
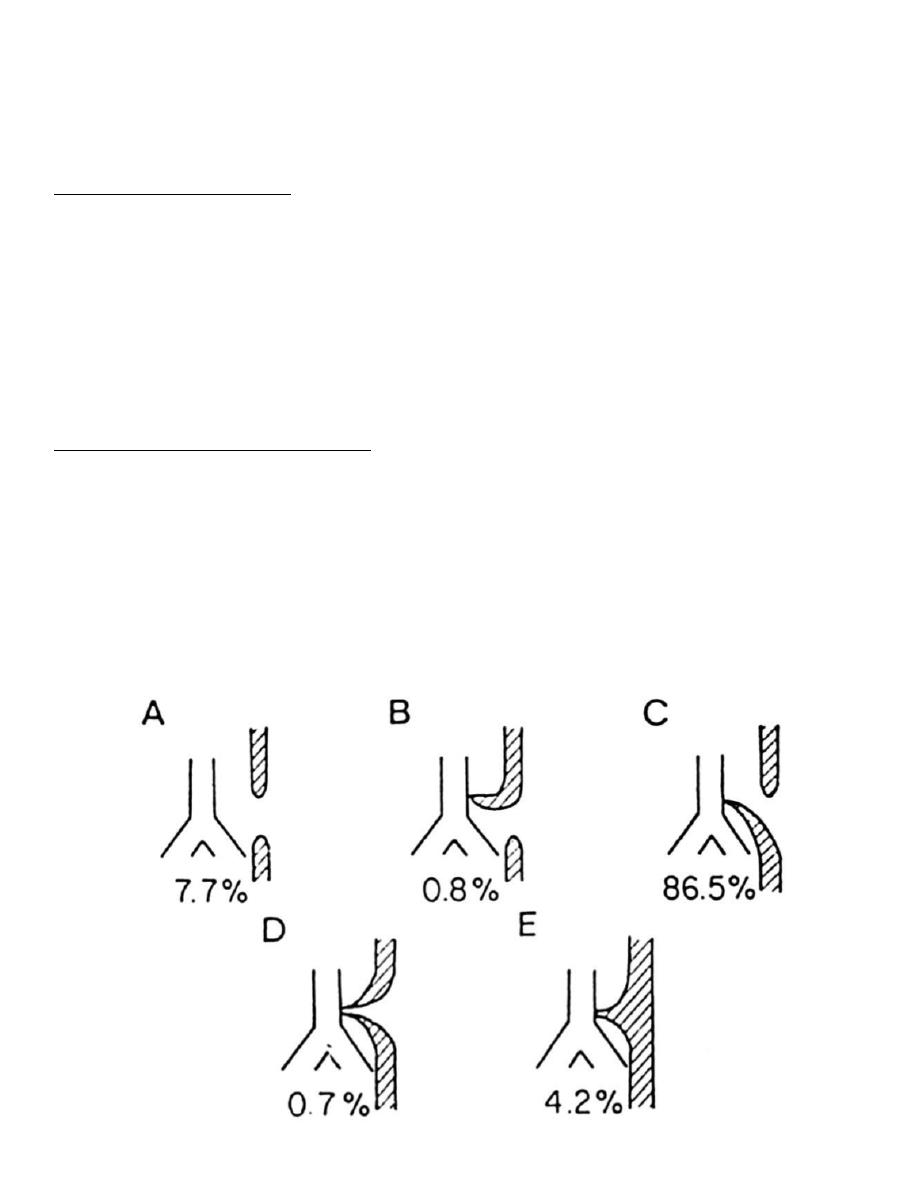
1-Atresia and fistula:
-
Uncommon.
-
may be incompatible with life.
-
segment of esophagus replaced by thin cord
-
may be connected to trachea, A,B,C,D&E.
-
May be associated with heart anomalies.
-
Aspiration and suffocation, pneumonia, and fluid and electrolyte
imbalance.
2-Stenosis, webs and rings:
-
webs in females < 40 years, ID anemia, dysphagia.
-
Plummer Vinson syndrome , SCC.
Types of tracheoesophageal anomalies and their relative
frequencies.
of
1
13

GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
-
Disruption of the normal physiological events of oropharyngeal or
esophageal swallowing results in one of the cardinal symptoms of
disease = DYSPHAGIA .
-
Dysphagia can be categorized as oropharyngeal or esophageal
depending on which phase is involved.
-
Dysphagia can be caused by 2 general types of disease processes:
1.Structural/mechanical abnormalities.
2.Neuromuscular (motor) abnormalities.
Causes of Esophageal Dysphagia:
-
Mechanical disorders.
-
(solid food only).
-
Peptic stricture.
-
Esophageal cancer
-
Schatzki ring.
-
Other.
-
Motor disorders 10-15%
-
(solid and liquid dysphagia).
-
Achalasia (#1).
-
Esophageal spasm (rare).
-
Scleroderma.
-
Other 85-90%
Mechanical Obstruction (solid food only):
Schatzki Ring
Peptic Stricture
Carcinoma
Intermittent progressive Slowly progressive
Rapidly
Chronic heartburn
Age >50 years
of
2
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
Achalasia
-
Formerly known as “cardiospasm”.
-
Characterized by:
-
Absent esophageal body peristalsis.
-
Incomplete LES relaxation.
-
LES hypertension
-
Causes:
1- Idiopathic or primary 95%+.
2- Secondary (acquired) as.
-
Neoplasm < 5%.
-
Other (e.g. amyloidosis) < 1%.
-
Chagas disease (trypansoma cruzii) rare and specific areas as south
America.
Primary Achalasia:
-
Pathology:
-
Loss of ganglion cells in myenteric plexus of esophagus.
-
Degenerative changes of the dorsal motor nucleus in the medulla in
some patients.
-
Etiology:
-
unknown, ? infectious.
-
Clinical features:
-
Gradually progressive dysphagia to solids & liquids.
-
Chest pain in some patients.
-
Nocturnal aspiration & weight loss may occur.
Achalasia:
-
Diagnosis:
-
Barium esophagogram.
-
Esophageal manometry.
-
Endoscopy (to exclude underlying neoplasm).
of
3
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
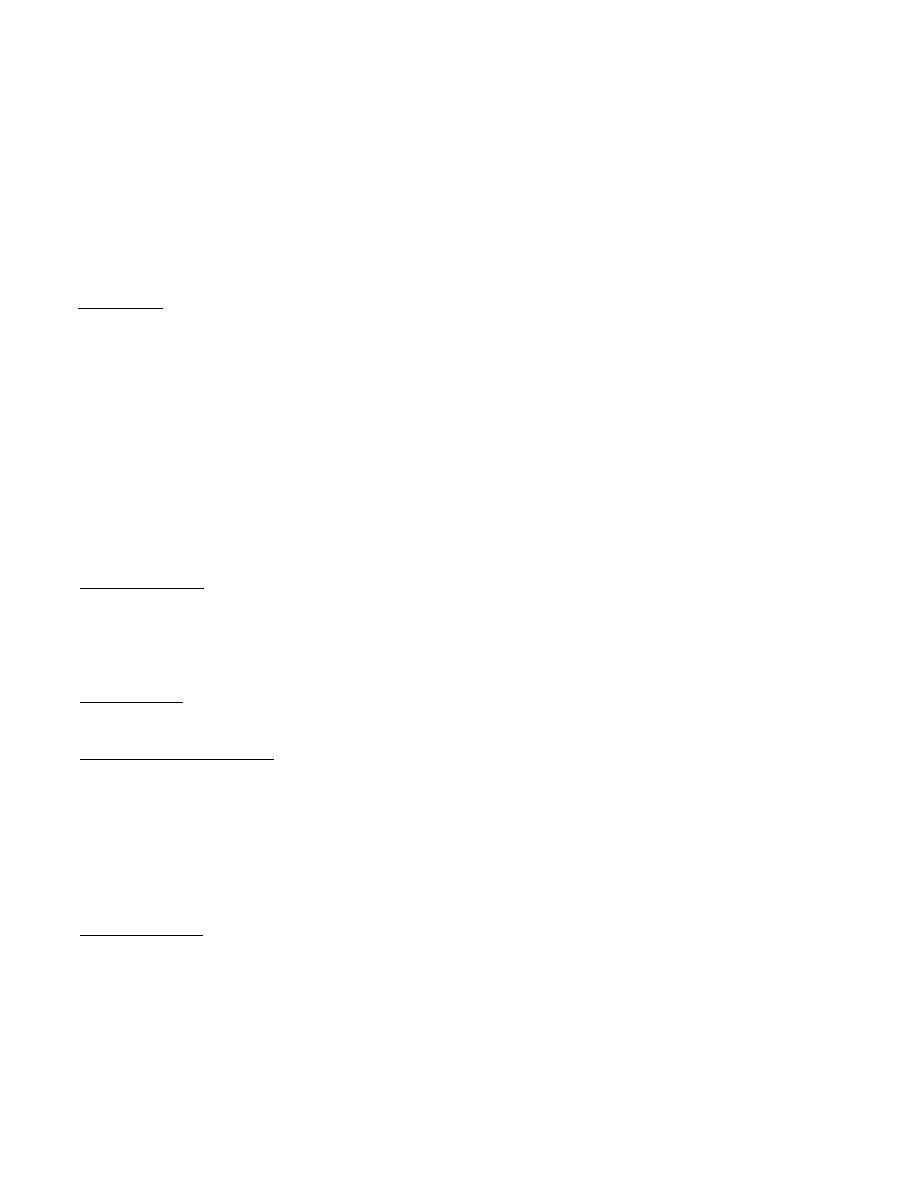
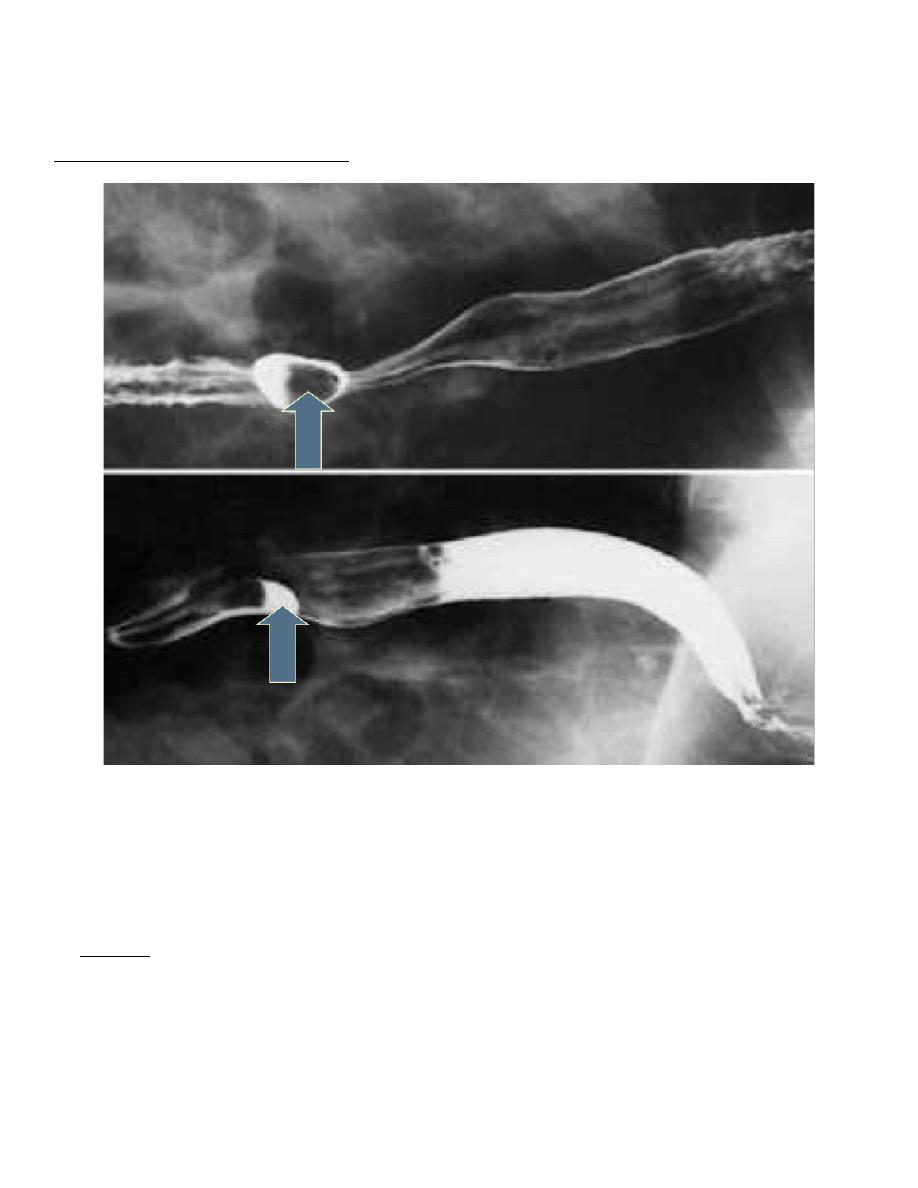
Achalasia:
-
Barium esophagogram.
-
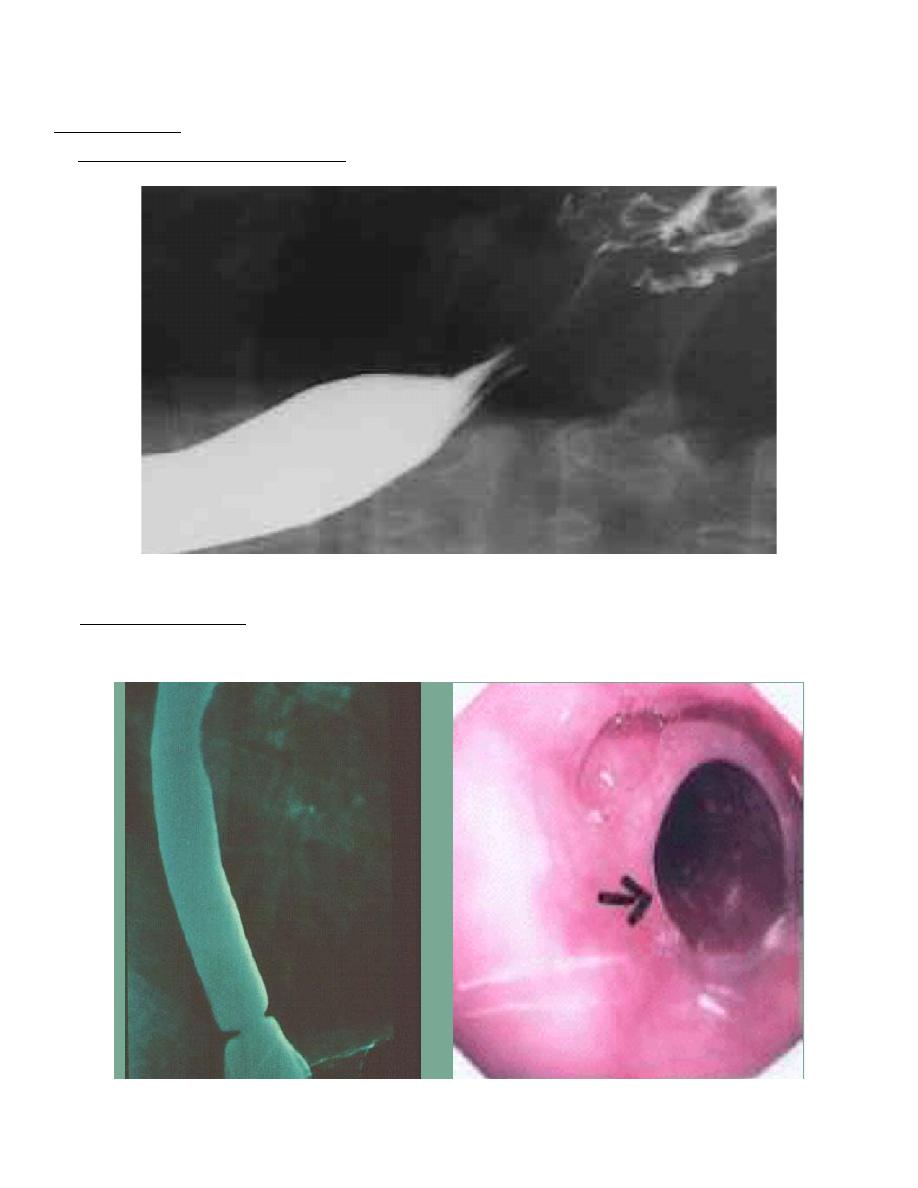
Schatzki Ring:
of
4
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
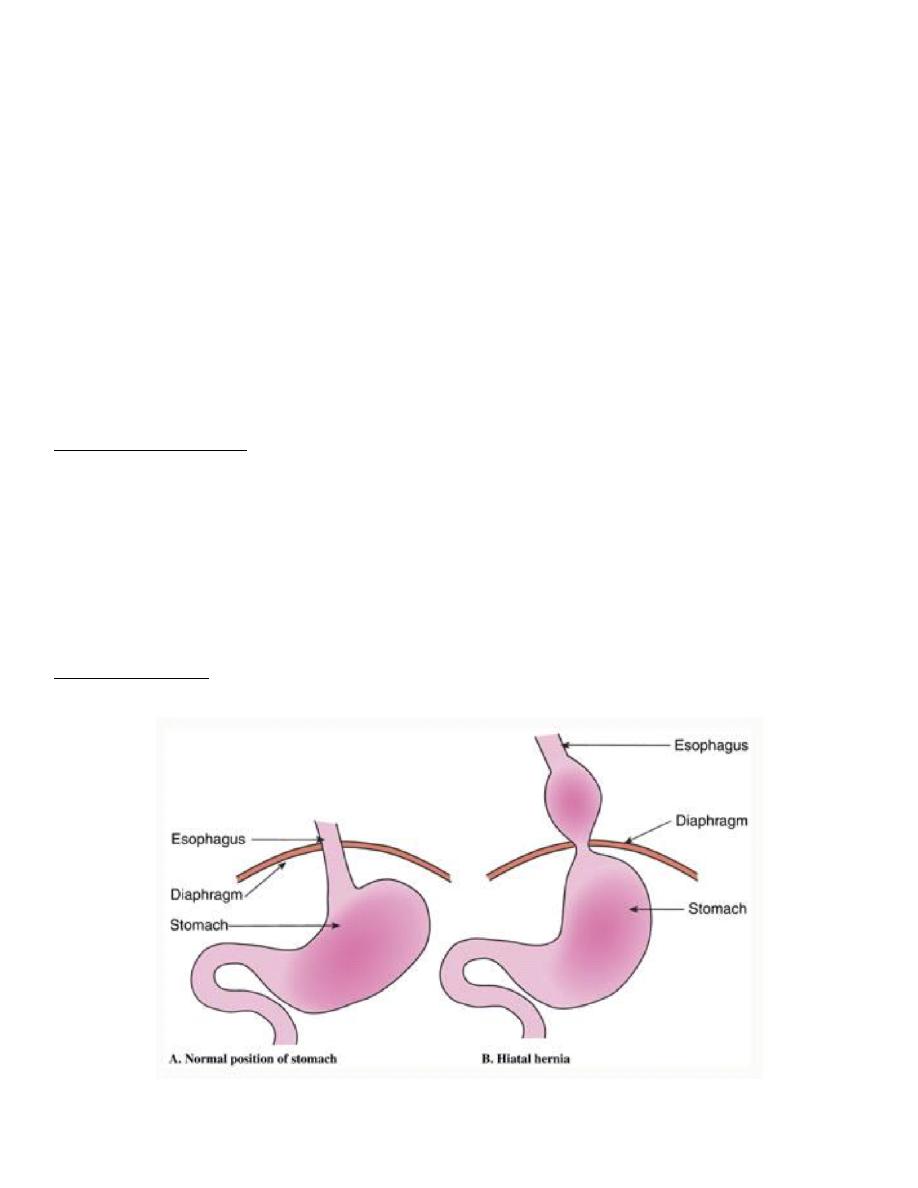
Hiatal Hernia:
-
It means separation of the diaphragmatic crura and widening of the space
between the muscular crura and the esophagus.
-
Two types:
1- Sliding: most common 95% (axial) due to protrusion of the
stomach above the diaphragm.
2- Para-esophageal (non axial) separate portion of the stomach
enter the thorax.
-
Cause unknown.
Clinical features:
-
The hernia prevents the food from moving normally along the digestive
tract.
-
Food moves back into the esophagus, creating a burning sensation
(heartburn), and sometimes food will be regurgitated into the mouth.
-
Can be complicated by strangulation, obstruction, ulceration, bleeding
and perforation.
Hiatal Hernia:
of
5
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
Lacerations (Mallory-Weiss Syndrome):
DIVERTICULA:
1- Proximal: The diverticula appearing in the upper portion of the
esophagus (Zenker's diverticula) are the result of out pouching of
esophageal mucosa at points of weakness in the wall of the esophagus at
the junction with the pharynx( pharyngoesophageal), classified as pulsion
diverticula. They occur at this point because of the relationship between the
inferior constrictor muscle and the obliquely passing fibers of the
cricopharyngeal muscles as they descend on the posterior wall of the
esophagus to become longitudinal.
2- Distal:In the lower third of the esophagus and in the region of the hilum
of the lung, inflammatory lymph nodes (usually tuberculous) can become
firmly attached to the esophagus and produce traction diverticula.
Definition
Longitudinal tears in the esophagus at the EG junction
Cause
Severe retching or vomiting.
Clinical
Upper GI bleeding
Morphology
Tear in mucosa, perforation or esophageal rupture
of
6
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
Esophageal Diverticulum:
varices:
-
Occur due to portal hypertension as a result of formation of collateral
bypass channels between portal system and caval system, along the
coronary veins of the stomach into the plexus of esophageal subepithelial
and submucosal veins into the azygos vein.
-
Gross: turtuous dilated veins in submucosa of distal esophagus and
proximal stomach, ero, inf.
-
Rupture causes massive bleeding.
-
May die from bleeding or hepatic coma (blood digestion).
of
7
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
ESOPHAGITIS:
-
Aetiology:
1- RE.
2- prolonged intubation.
3- irritants.
4- Cytotoxic, radiation.
5- Viral and fungal infection.
6- uremia and hypothyroidism.
Gross and microscopy:
-
Hyperemia, inflammation, ulceration and granulation tissue.
-
MIC:
1- eosinophilic infiltration. + neutrophil.
2- basal cell hyperplasia.
3- elongation of the lamina properia papillae.
pathogenesis
1- decreased efficacy of esophageal anti-reflux mechanism.
2- Inadequate or slowed esophageal clearance of refluxed material.
3- presence of sliding hiatal hernia.
4- increased gastric volume.
5-reduction in the reparative capacity of the esophageal mucosa by
protracted exposure to gastric juices.
Severe, long term affects
-
Gastrointestinal bleeding.
-
Stricture.
-
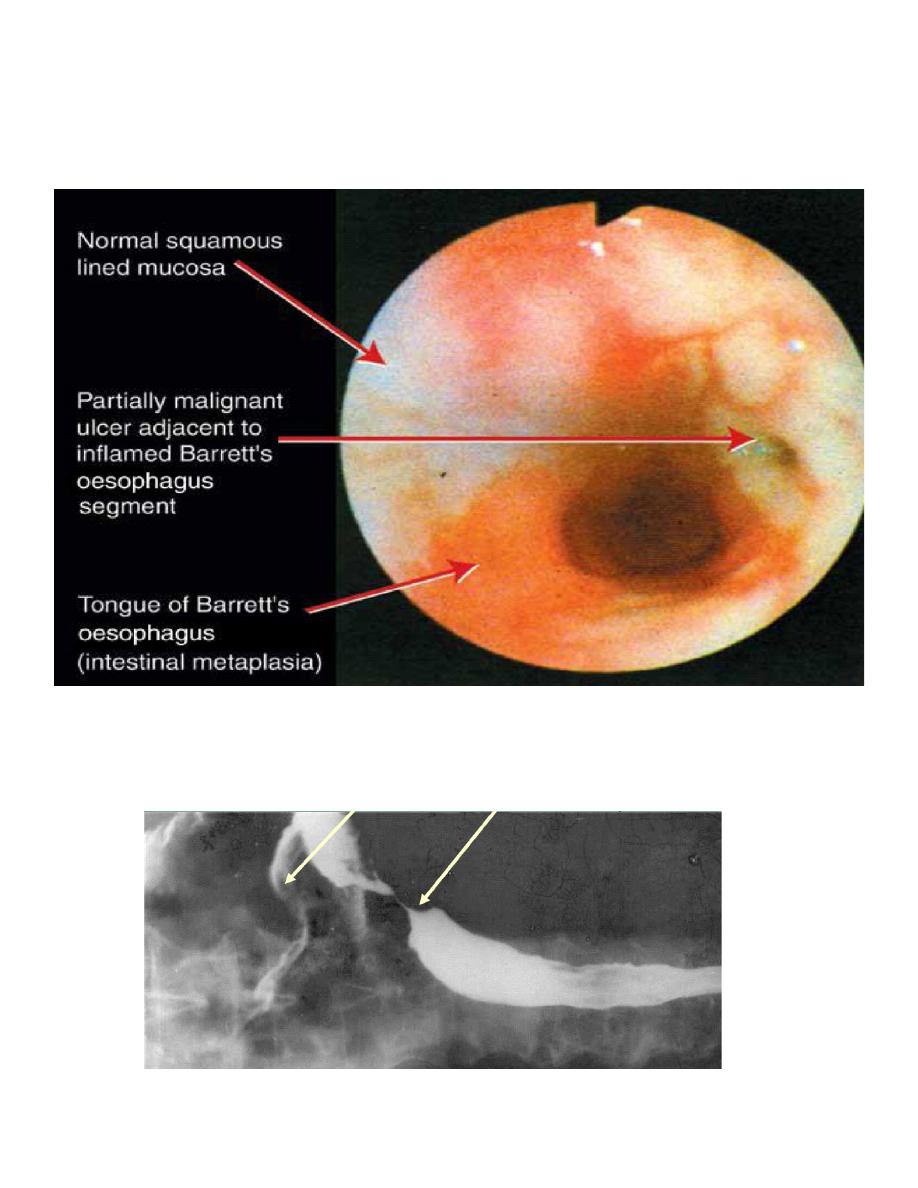
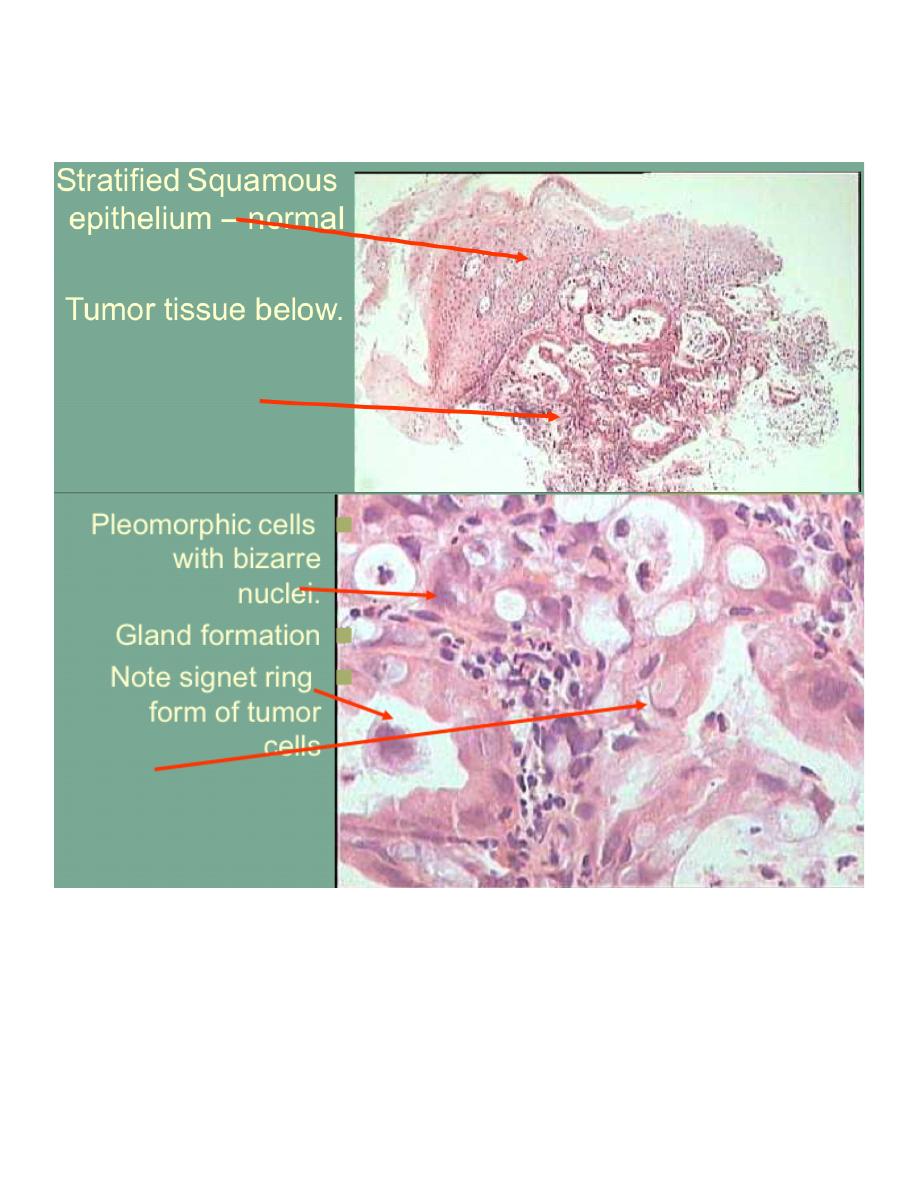
Barrett’s esophagus.
-
There is columnar epithelium in the esophagus where stratified
squamous epithelium should be .
of
8
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
-
And its risk = Cancer .
BARRETTS ESOPAHGUS
-
11 % of symptomatic reflux disease.
-
Pathogenesis: prolonged recurrent GER leads to inflammation, ulceration
of Sq.ep.
-
Which heal by re epithelialization and in growth of pluripotent stem cells,
which in acidic microenvironment differentiate into gastric cells or
intestinal which is more resistant to acids.
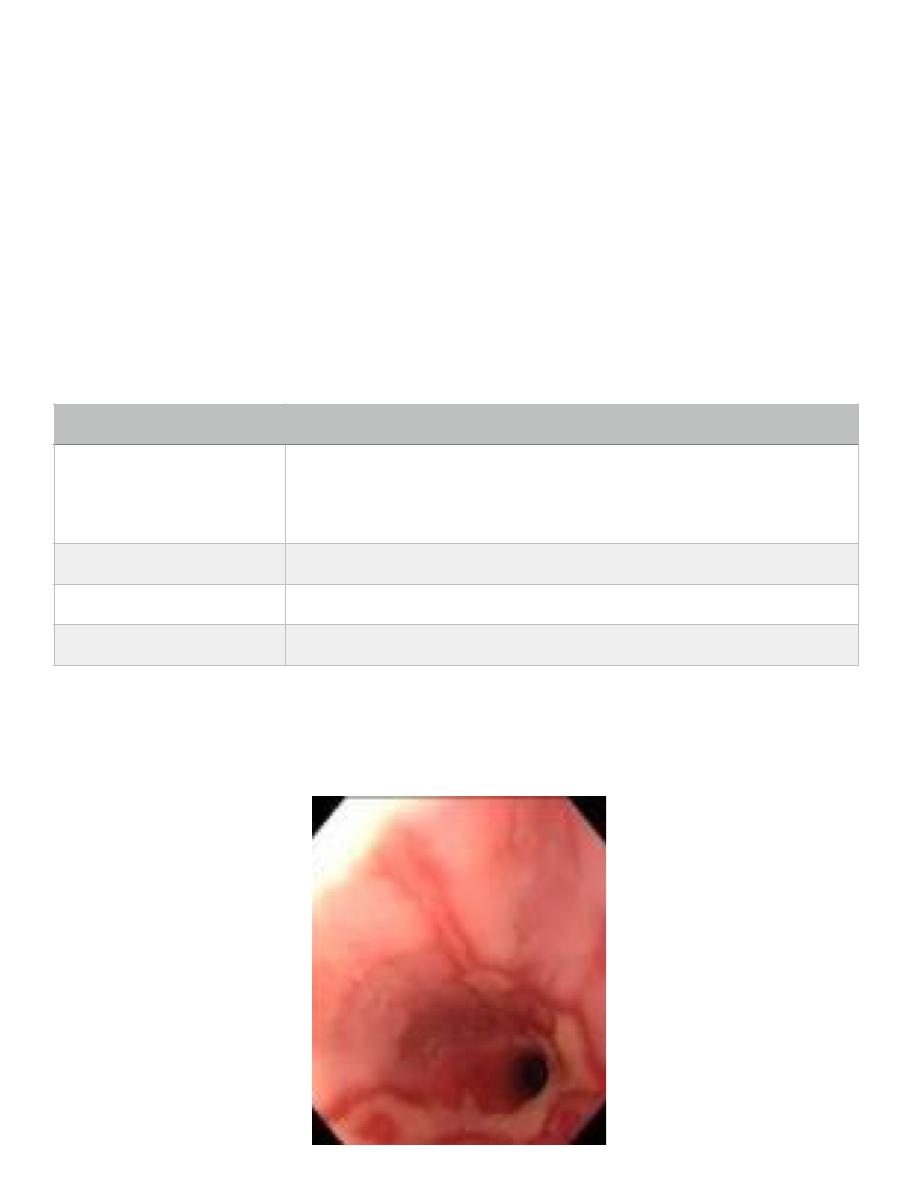
Barrett
RE
Barrett esophagus
Cause →
Long standing GE reflux. risk to get Barrett ́ s
esophagus increases with the duration and amount
of acid reflux
Clinical →
Heart burn, pain
Morphology →
Gross and microscopy: columnar metaplasia
Compilation →
Adenocarcinoma 0.5% per year
of
9
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
BE & CA
Barium Swallow:
Little entry into stomach. Narrowing
of
10
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
Esophageal
of
11
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
ESOPHAGEAL TUMORS:
-
BENIGN :
-
leiomyoma, fibroma, lipoma, hemangioma, neurofibroma.
-
MALIGNANT:
1- SCC.
2- UNDIFFERENTIATED.
3- CARCINOID.
4- MALIGNANT MELANOMA.
SQUAMOUS CELL Esophageal Carcinoma:
SQUAMOUS CELL CARCINOMA:
Etiology:
1- vit A and C def.
2-Alcohol and tobacco.
3- esophagitis and achalasia.
4-high content of nitrites in diet.
5-fungal infection.
6-HPV might play an etiologic role in esophageal carcinogenesis either by
producing carcinogens or promoters or by acting directly on the host cells.
Etiopathogenesis
A c h a l a s i a , P l u m m e r - V i n s o n
syndrome, alcohol, tobacco, HPV,
deficiency of vitamins A, C, B1, B6 ;
fungal contamination.
Type of tumor
Squamous cell carcinoma
Morphology
Gross and microscopy
of
12
13
GASTROINTESTINAL T
Lectures 3&4
Depart. Of pathology
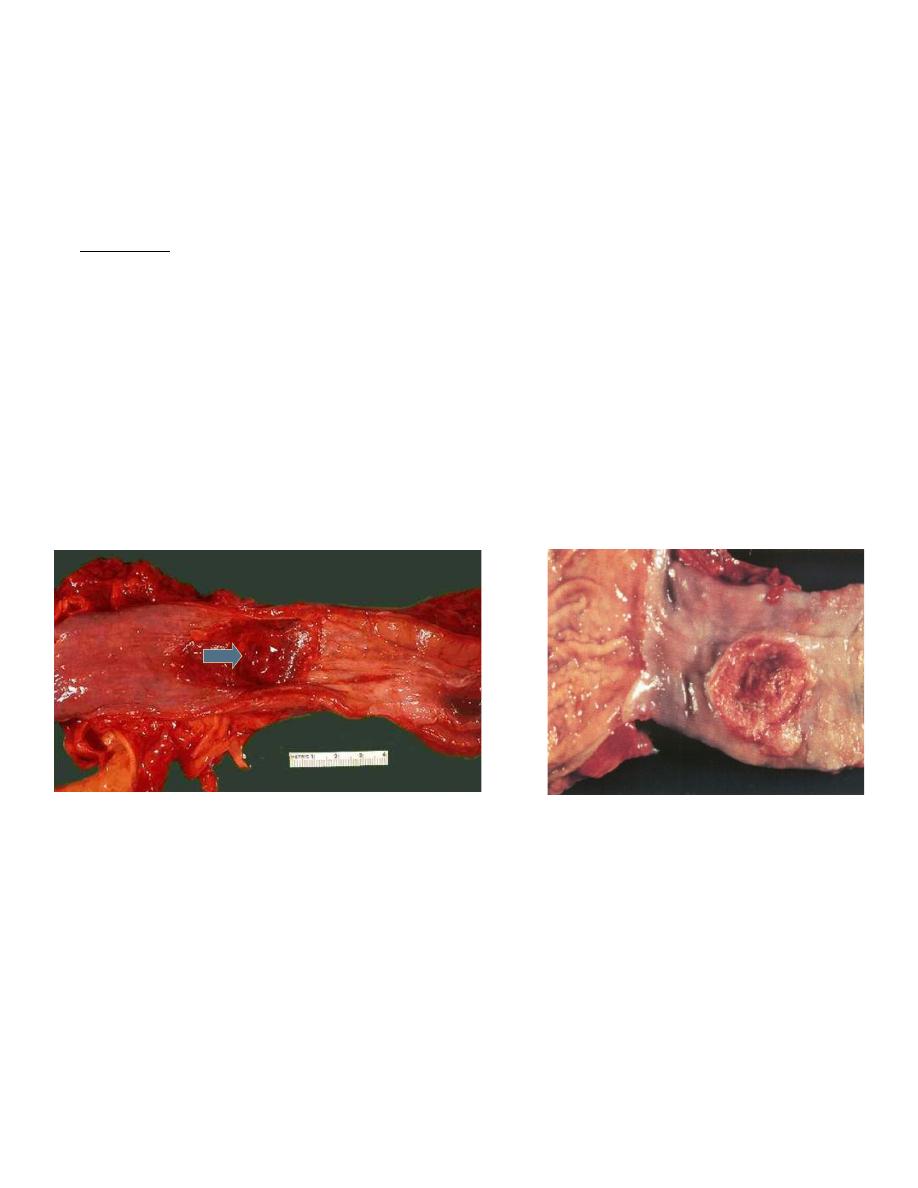
Morphologic features and local spread:
-
Squamous cell carcinoma can occur in any portion of the esophagus but
is most common in the middle and then lower thirds in areas of normal
anatomic constrictions.
-
Grossly: the tumor usually is circumferential, often ulcerated, with
sharply demarcated margins. Polypoid forms occur, but are much less
common than in adenocarcinoma. --On cut section, a grayish white tumor
is seen to invade part or all of the muscular wall, from which it may
extend into the surrounding soft tissues and trachea.
-
Intraluminal growth also occurs and may eventually lead to total
obstruction.
-
Distally located tumors often invade the stomach.
Esophageal Carcinoma:
of
13
13