Lecture 13 pathology LIVER 3
rd
Stage
1
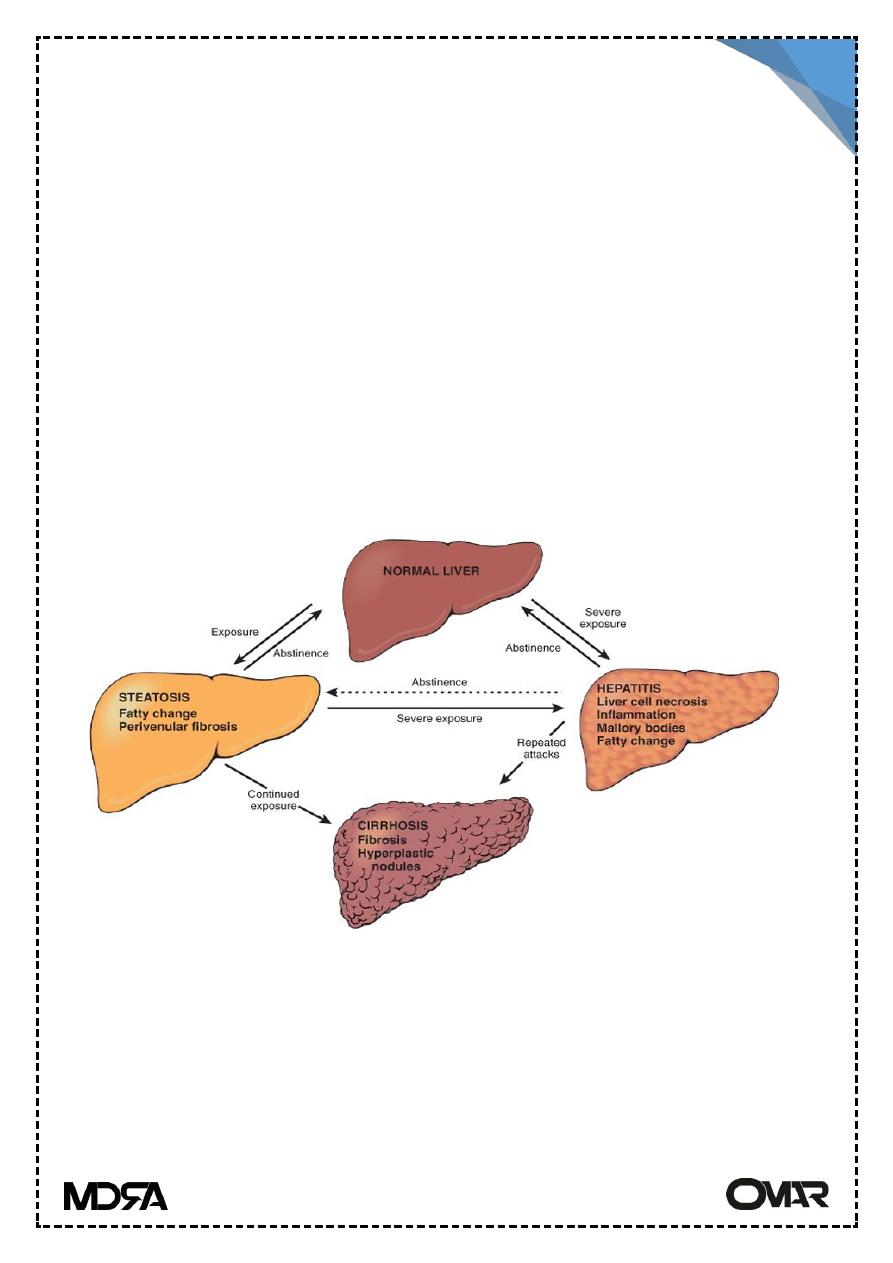
Alcoholic liver disease
Alcoholic abuse constitute the major form of liver disease in most western
countries . Toxicity of ethanol is due to generation of its metabolic
breakdown product acetaldehyde. 3 distinctive forms of liver disease are
characterized are hepatic steatosis (fatty liver), Alcoholic hepatitis &
alcoholic cirrhosis.
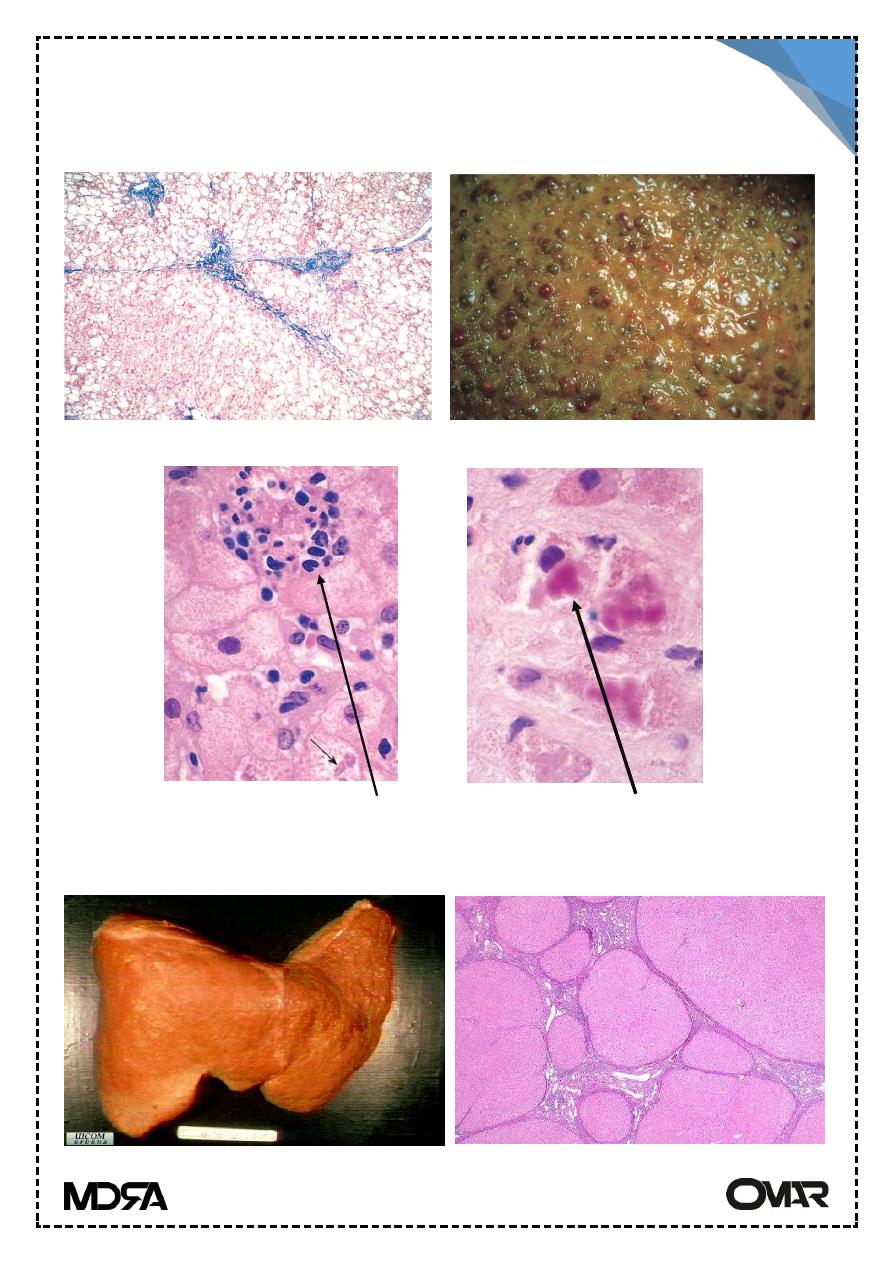
Hepatic steatosis
Small micro-vesicular lipid droplets accumulate in hepatocytes with
moderate alcohol intake. With chronic alcohol intake, lipid accumulate in
macrovesicular droplets, displacing the nucleus. Firstly it's centrilobular,
over time the entire lobule may be involved.
The liver is enlarged & soft & yellow, fibrosis may develop.
Alcoholic hepatitis
liver cell necrosis, especially the centrilobular region. Mallory body
formation (eosinophilic clumped filaments), neutrophilic reaction,
inflammation in the portal tracts spilling into the lobules & fibrosis
Alcoholic liver disease
Lecture 13 pathology LIVER 3
rd
Stage
2
(sinusoidal, periportal). Liver function test show raised levels of
transaminases & γ-glulamyl trans peptidase.
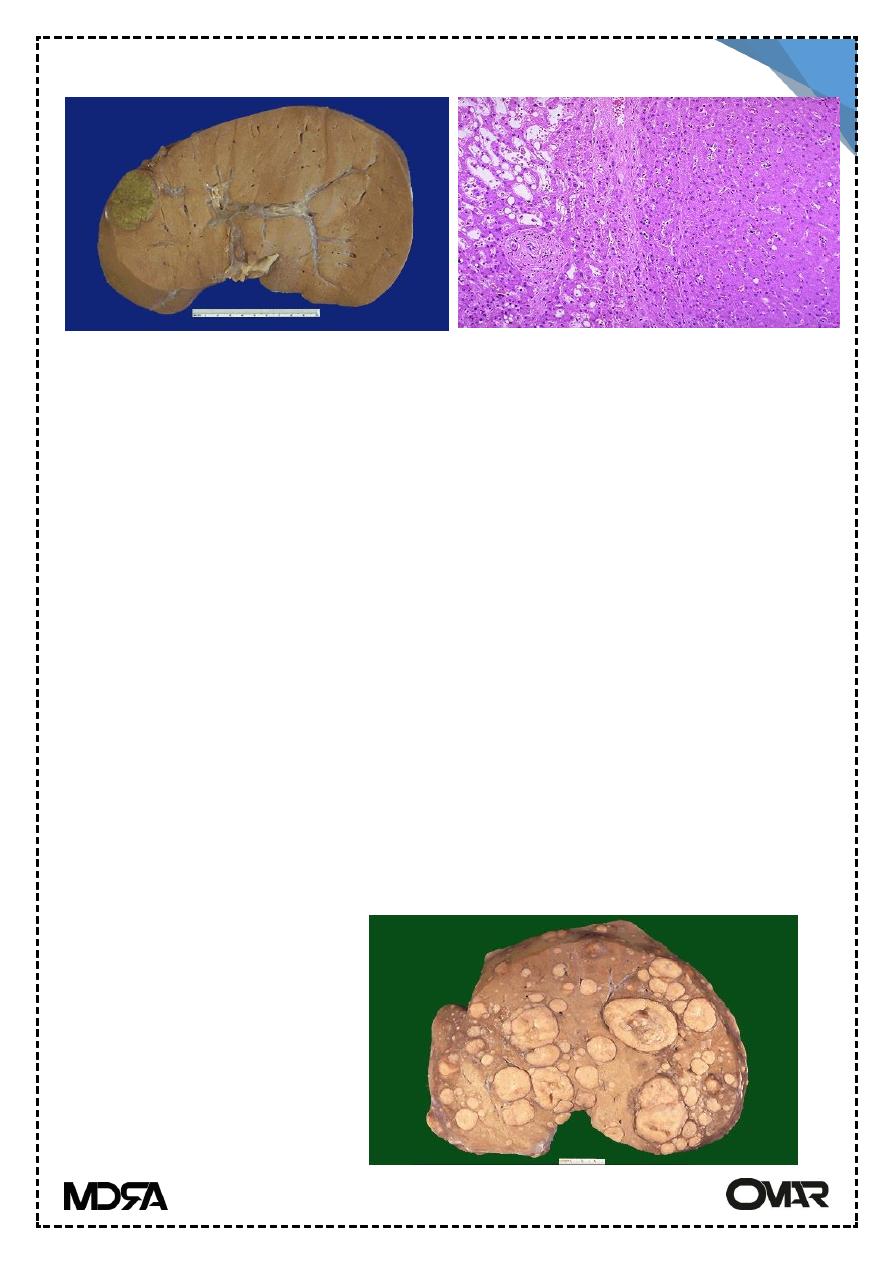
Alcoholic Cirrhosis
Alcoholic steatosis
Alcoholic cirrhosis
Alcoholic hepatitis: inflammation and Mallory bodies
Lecture 13 pathology LIVER 3
rd
Stage
3
Alcoholic cirrhosis
The liver is transformed from fatty & enlarged organ to brown shrunken, non
fatty organ. Regenerative nodule are prominent with dense fibrous bands
Drug induced liver disease
Drugs are very common cause of liver disease. liver pathology as follows:-
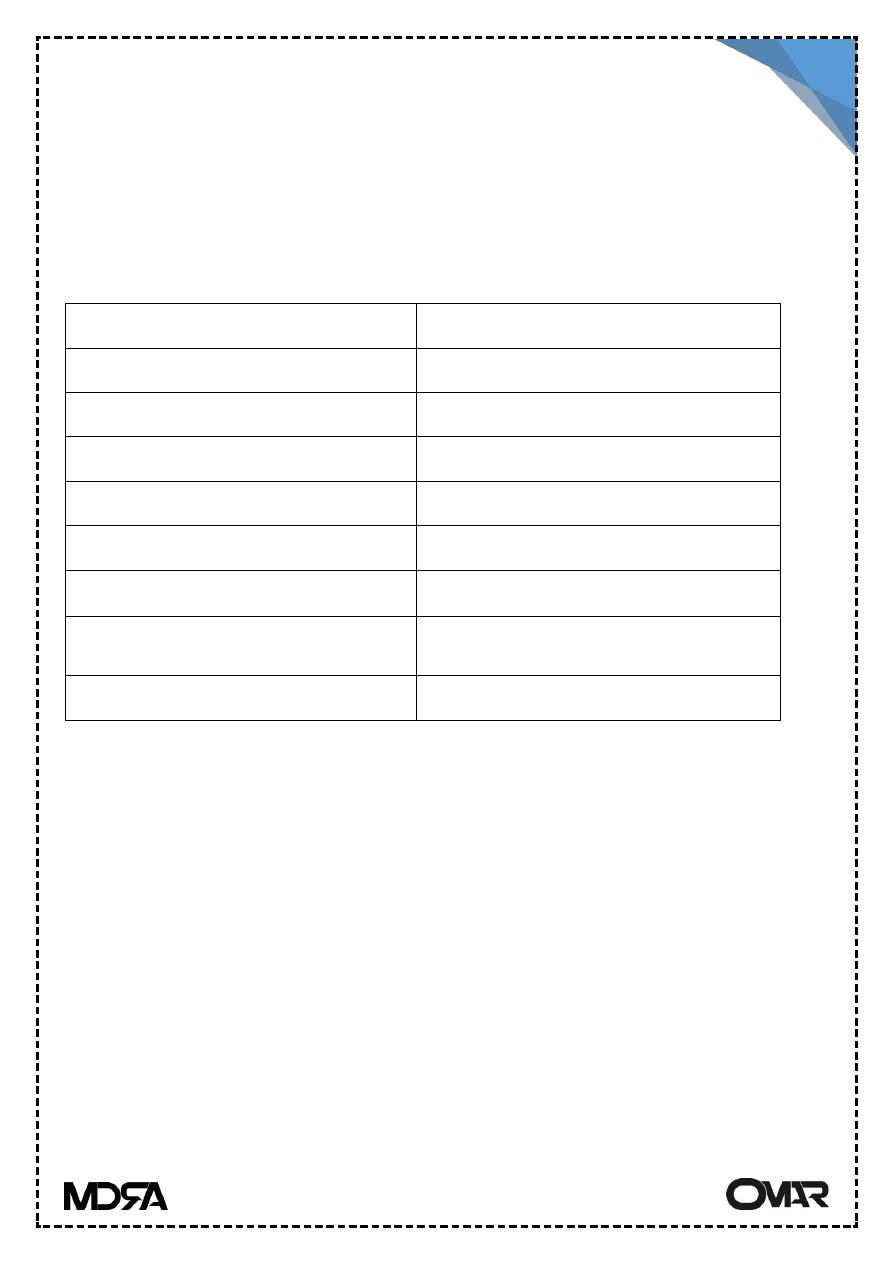
Liver pathology
Drugs causing damage
Fatty change
Methotrexate, tetracycline
Hepatic granulomas
Sulphonamides, allopurinol
Acute Hepatitis
Isoniazid, halothane
Chronic hepatitis
Isoniazid, methyl dopa
Cholestasis
Steroids, chloropromazine
Central vein occlusion
Cytotoxic drugs
Tumors
Oral contraceptives (adenoma )
Anabolic steroids (carcinomas)
Acute necrosis
Paracetamol
Autoimmune hepatitis
Chronic hepatitis in a patient with immunologic abnormalities.
Histologic features are similar to chronic viral hepatitis.
Responds to immunosuppressive Rx.
Characterized by:
Female predominance.
Absence of serological markers of viral infection.
↑↑ level of serum IgG.
High titer of autoantibodies.
Associated other autoimmune diseases.
Lecture 13 pathology LIVER 3
rd
Stage
4
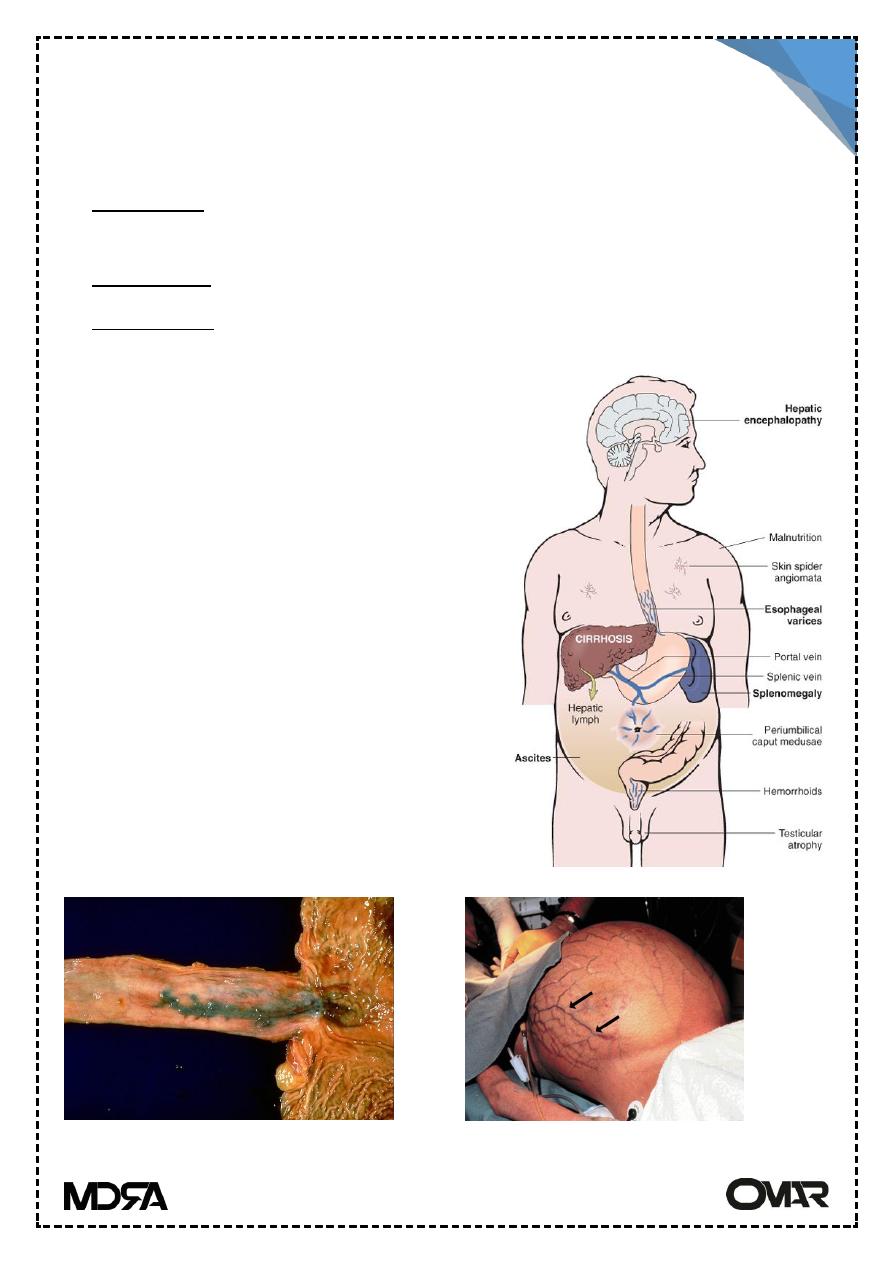
Portal hypertension
Increased resistance to portal blood flow:
pre-hepatic: obstruction or narrowing of portal vein by a thrombus before
the liver, and splenomegally.
Intrahepatic : cirrhosis, massive fatty changes &TB.
Post-hepatic: right sided heart failure, constrictive pericarditis & hepatic
vein out flow obstruction (Budd-chiari synd.).
Clinically
1- Ascites: accumulation of excessive fluid
in the peritoneal cavity-
pathogenesis : a) sinusoidal hypertension
b) movement of hepatic lymph to the
peritoneal cavity.
c) leakage of intestinal fluid.
2- Porto-systemic shunt
esophageal varices, caput meduse.
Hemorrhoids
3- Splenomegaly:
4- Hepatic encephalopathy
Consequences of portal hypertension
Esophageal varices
Caput medusae

Lecture 13 pathology LIVER 3
rd
Stage
5
Tumors and Tumor-like conditions
Nodular hyperplasia
Solitary or multiple hyperplastic hepatocellular nodules developing in non-
cirrhotic liver.
Two types:-
focal : appears as poorly encapsulated well- demarcated nodules, they
develop spontaneously in young to middle aged females.
nodular regenerative hyperplasia roughly spherical nodules affecting the
entire liver in the absence of fibrosis, it is associated with portal
hypertension.
Both conditions are due to augmentation to hepatic art. Blood flow to
compensate portal v. obstruction
Benign tumors
Adenoma: occurs in young ♀ on oral contraceptive if they are interior they
might be mistaken with hepatocellular carcinoma.
Those near the capsule tend to rupture specially during pregnancy (estrogen
dependant). They are composed of sheet or cords of cells resemble normal
hepatocytes.
Esoph. Varieces
Spider angiomas
Lecture 13 pathology LIVER 3
rd
Stage
6
Hemangioma
Haemangioma of the liver is common. It is seen beneath the capsule as a
dark almost black, lesion (typically 2-3 cm in size) which histologically, is
composed of abnormal vascular channels in a collagenous stroma
Malignant tumor : Primary & Secondary
The most common malignant tumor of the liver is metastatic tumor. Spread
to the liver is via the bloodstream, either from the portal vein in the case of
tumors in the gastrointestinal tract, or by the systemic circulation for other
tumors. Clinically the liver is enlarged, feeling hard and craggy on palpation.
The lung, breast, colon, and stomach are the most common primary sites
of tumors metastasizing to the liver.
Many other tumors also spread to the liver, but they are numerically less
frequent. There is often involvement by tumors of the lymphoreticular
system, malignant lymphomas, and by malignant tumors of the bone
marrow leukaemias.
Small deposits of tumor
in the liver have little
clinical effect but, when
extensive,
metastases
cause compression of the
intra-hepatic bile ducts and
lead
to
obstructive
jaundices.
adenoma
Lecture 13 pathology LIVER 3
rd
Stage
7
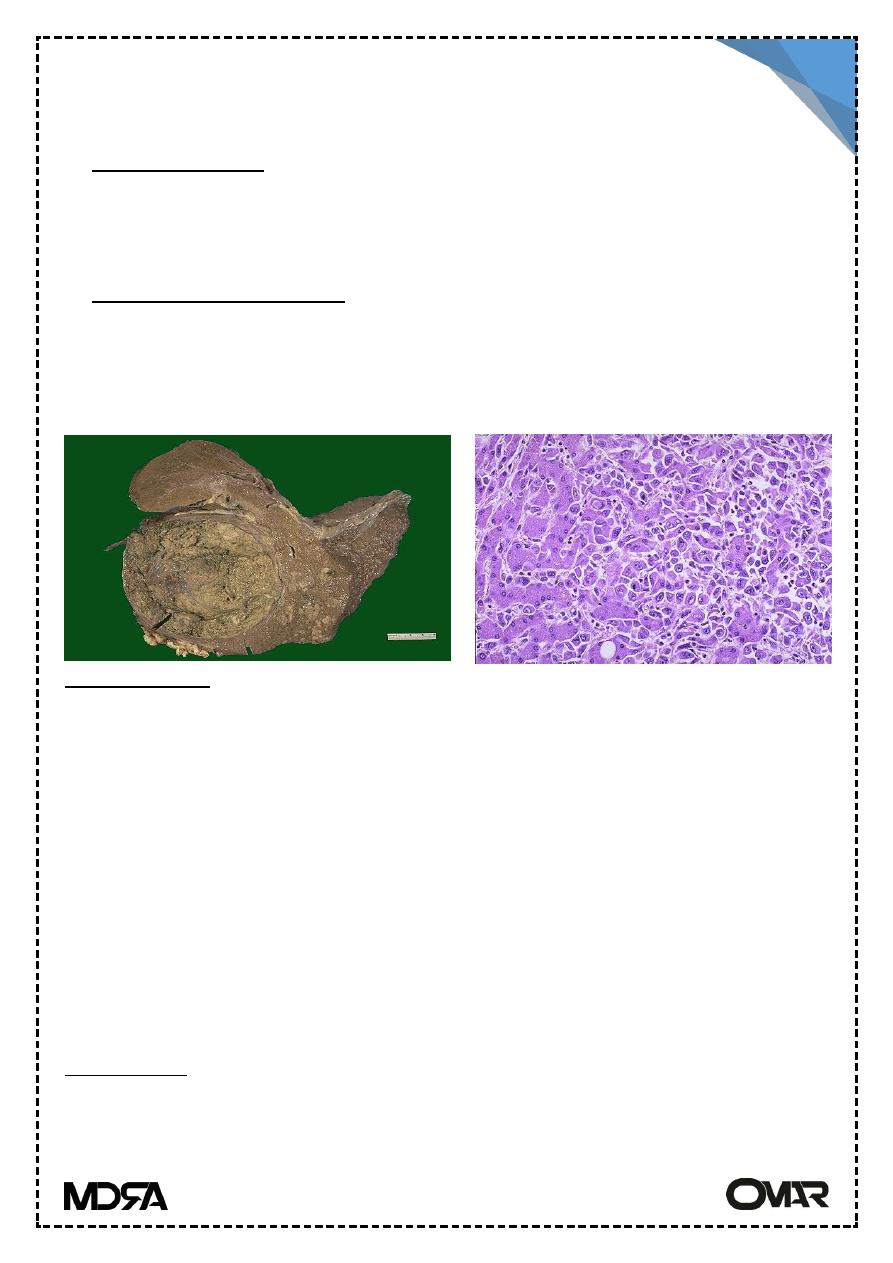
Primary tumors
Hepatoblastoma : in young children usually fatal
Two types : 1- epithelial
mixed epith. & mesenchymal
hepatocellular carcinoma
: tumors of hepatocyte
its distribution is closely linked to HBV infection HCV & alcoholic liver
cirrhosis & hemochromatosis.
Pathogenesis :
1. accumulation of mutation during continuous cell cycles → transformed
hepatocytes.
2. viral integration precedes or accompanies transformations i.e: there is
clonal expansion of transformed cells.
3. Integrated viral DNA effect is not limited to the integrated site but a wide
genomic instability is produced.
4. HBV x protein acts as transactivator of cellular & viral promoters. It acts
as transcriptional activator to some growth factors. it also binds to P53.
5. Food mold aflatoxin are activated in hepatocytes mutagenic adducts.
Morphology
Unifocal, multifocal, diffuse infiltrative type
Lecture 13 pathology LIVER 3
rd
Stage
8
Gross: paler than surroundings. If they are composed of well differentiated
hepatocytes they take a green blue.
Invasion of vascular channels occlusion of portal vein.
Micros.: well differentiated to anaplastic trabecular, acinar,
pseudoglandular patterns.
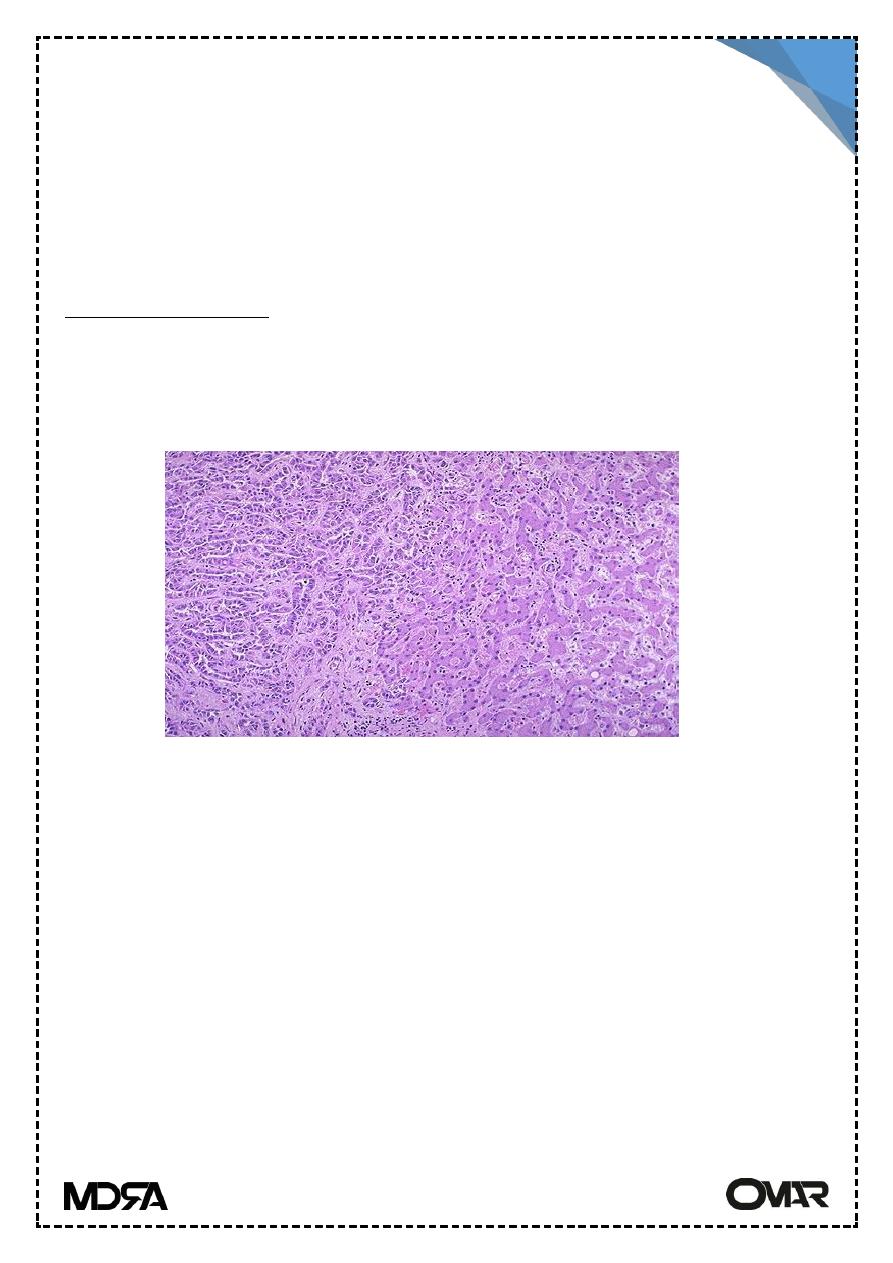
Cholangiocarcinoma :
Related to the use of thorotrast in radiography of biliary tract & to liver
flukes or without any risk factor
It is Adenocarcinoma in type.
Cholangioca.
Angiosarcomas
Derived from vascular endothelium, angiosarcomas are highly malignant
tumors that appear as multifocal haemorrhagic nodules with the liver.
Importantly, such tumors are rare unless there has been exposed to
thorotrast ( a radiological contrast agent used until the 1950s), vinyl chloride
monomer( used in the plastic industry to make PVC), arsenic (administrated
in the past in certain tonics'), or anabolic steroids.