Narcotic analgesic“Opioid analgesics”
Opium the dried juice of the seed-head of the opium poppy ( F. papaveracae)
Mechanism of action
Opioids act to reduce intensity and unpleasant of pain. They produce their effects by activating specific G-protein coupled receptors in the brain, spinal cord and peripheral nervous system. There are three major classes of opioid receptor µ-opioid, ĸ-opioid, and δ-opioidSystemic effects of opioid analgesics
1- Central nervous systemSedation
Respiratory depression
Cough is inhibited
Miosis
2- Cardiovascular system
Peripheral vasodilatation
Hypotension- seldom troublesome
Benefit in acute myocardial infarction and left ventricular failure (reduce pain and anxiety, and preload)
Systemic effects of opioid analgesics (continued)
3-Gastointestinal tract
Reduced peristalsis and delayed gastric emptying ( cause constipation)
opioids constrict the sphincter of oddi and thereby increase pressure within the biliary tree ( biliary spasm)
4- Urogential tract
urinary retention
Systemic effects of opioid analgesics (continued)
5- OthersCutaneous vasodilatation (flushing of face, neck and thorax)
Adverse effects
* Sedation, euphoria, dysphasia, respiratory depression, constipation, pruritis, and nausea and vomiting.* Many of these effects diminish as tolerance develops.
* Constipation and dry mouth ( lead to dental caries) are more resistance tolerance and remain problems.
Classification
TraditionalStrong ---------------morphine, Fentanyl
Intermediate -------buprenorphine, pentazosine
Weak -----------------codiene
Functional
Pure agonist----------morphine, codiene
Partial agonist-------- buprenophine
Mixed action----------pentazosine
Antagonist-------------naloxone,naltrexone.
1- Pure agonist
Morphine
The most widely used analgesics for the treatment of severe pain. It is the gold standard
Diamorphine (heroin)
It is semisynthetic drug. It is now illegal.
Morphine- (3,6 dihydroxy) Heroin- 3,6 diacetyl morphineCodeine- 3 methyl morphine
Codeine
It is obtained naturally or by methylation of morphine. It has low affinity for opioid receptor and most of the analgesic effects results from its metabolism (10%) to morphine. Its principle uses are for mild and moderate pain and for cough.Methadone
The principle feature of methadone is its long duration of action, due to high protein binding and slow liver metabolism.When used in cancer-related pain or chronic non-malignant pain and opioid of short half life should be provided for break through pain rather than an extra dose of methadone.
Fentanyl
It is of the short acting opiods developed for use in anaesthesia. It is approximately 100 times more potent than morphine.At higher dose, its duration of action is much longer. Fentanyl is ideally used as transdermal patch for highly lipid soluble. It is used in cancer pain and non-malignant pain.
Fentanyl transdermal

2- Partial agonist
BuprenorphineIt acts on µ receptor. It has less liability to induce dependence and respiratory depression than pure agonist. It is 30 times more potent than morphine and dissociates very slowly from the receptor.
Buprenorphine (continue)
The low incidence of drug dependence has led to its increased use in withdrawing opioid addicts and in chronic non-malignant painBecause of the first pass metabolism buprenorphine is given sublingually or IM, or slow intravenous injection
3- Mixed agonist-antagonist
PentazocineIt acts as a partial agonists at the ĸ receptor and as weak antagonists at the µ receptor .
It may cause withdrawal symptoms in patients dependent on other opioids.
It is not as efficacious as pure µ agonist.
Compared with morphine it produces less dependence and less sedation and respiratory depression
4- Opioid with action on other system
Pethidine (meperidine)It is µ,k receptors as agonist. It is similar to morphine but less effective.
It has atropine-like effect.
It can produce euphoria and dependence.
It is used for analgesia in obstetrics, since unlike morphine it did not delay labor
Tramadol
It is relatively weak µ-receptor agonist.
It inhibits neural reuptake of noradrenaline and enhance serotonine release
5-Opioid antagonist naloxone, naltrexone
NaloxoneIt is a competitive antagonist at µ, and δ opioid receptors and reverse the effect of most opioid analgesics. It acts within minutes.
It is usually shorter than that opioid induced respiratory depression. Repeated doses of naloxone may be necessary. Naltrexone long duration of action.
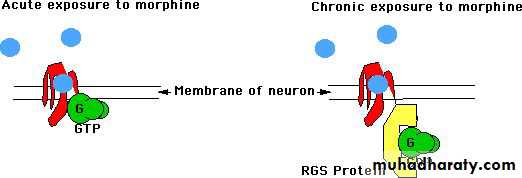
Opioid tolerance, dependence and addiction
ToleranceThe need to increase the dose of a drug with time to achieve the same analgesic effect.
Tolerance to adverse effect as follows
Respiratory depression is tolerated with increasing the dose
Constipation is less predictable
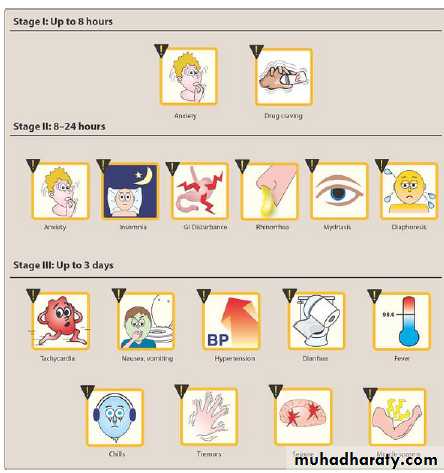
Dependence (physical)
The withdrawal syndrome include:Abdominal cramps, sweating, tremer, coryza, myalagia, vomiting and diarrhoea
Addiction
Negligible in acute pain
Low in chronic pain
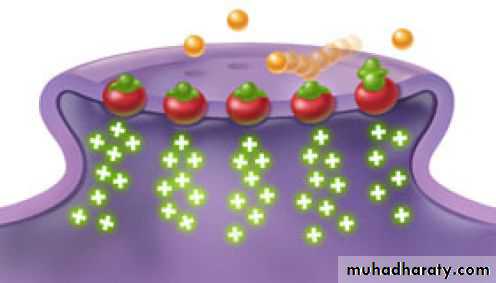

When opiates are taken into the body, dopamine is released which produces a feeling of pleasure and euphoria. As the drugs wear off, the receptors which received the opiates are left empty, causing withdrawal symptoms to begin. The buprenorphine in Suboxone attaches to the empty receptors and stops them from feeling the pangs of craving and withdrawal. It is a partial opioid agonist, which means it completely halts withdrawal without producing the euphoria and unconsciousness that is counterproductive to a healthy, functioning lifestyle. At its best, buprenorphine also blocks other opiates from attaching to the empty receptors and does not allow a high to be felt.