SYMPTOMS OF LIVER DISEASE
Acute liver diseaseThis may be asymptomatic and anicteric. Symptomatic disease, which is often viral, produces generalized symptoms of malaise, anorexia and fever. Jaundice may appear as the illness progresses.
Chronic liver disease
Patients may be asymptomatic or complain of nonspecific symptoms, particularly fatigue. Specific symptoms include:
Right hypochondrial pain due to liver distension
Abdominal distension due to ascites
Ankle swelling due to fluid retention
Haematemesis and melaena from gastrointestinal haemorrhage
Pruritus due to cholestasis – this is often an early symptom of primary biliary cirrhosis
Breast swelling (gynaecomastia), loss of libido and amenorrhoea due to endocrine dysfunction
Confusion and drowsiness due to neuropsychiatric complications (portosystemic encephalopathy).
Jaundice (icterus) is a yellow coloration of the skin and mucous membranes and is best seen in the conjunctivae and sclerae.
In the cholestatic phase of the illness, pale stools and dark urine are present.
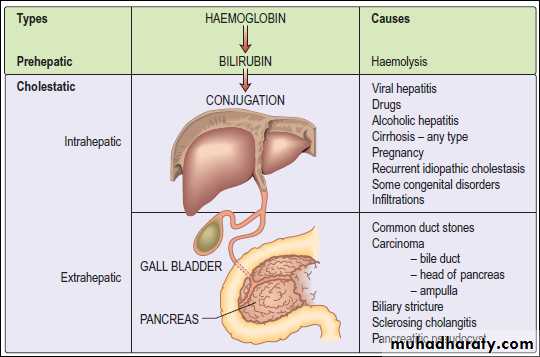
Jaundice is detectable clinically when the serum bilirubin is >50 μmol/L (3 mg/dL). In a patient with jaundice it is useful to consider whether the cause might be pre-hepatic, hepatic or post-hepatic.
Pre-hepatic jaundice
This is caused either by haemolysis or by congenital hyperbilirubinaemia, and is characterised by an isolated raised bilirubin level.Hepatocellular jaundice
Hepatocellular jaundice results from an inability of the liver to transport bilirubin across the hepatocyte into the bile, occurring as a consequence of parenchymal liver disease.
Obstructive (cholestatic) jaundice
Cholestatic jaundice may be caused by:• failure of hepatocytes to initiate bile flow
• obstruction of bile flow in the bile ducts or portal tracts
• obstruction of bile flow in the extrahepatic bile ducts
between the porta hepatis and the papilla of Vater.
spider naevi these are telangiectases that consist of a central arteriole with radiating small vessels. They are found in the distribution of the superior vena cava (i.e. above the nipple line) – commonly more
than five is taken as diagnostic. They are also found in pregnancy.
palmar erythema, which is a nonspecific change indicative of a hyperdynamic circulation; it is also seen in pregnancy, thyrotoxicosis or rheumatoid arthritis.
Xanthomas (cholesterol deposits) are seen in the palmar creases or above the eyes in primary biliary cirrhosis.
Gynaecomastia (occasionally unilateral) and testicular atrophy may be found in males. The cause of gynaecomastia is complex, but it is probably related to altered oestrogen metabolism or to treatment with spironolactone.
Ascites
Ascites is fluid within the peritoneal cavity and is a common complication of cirrhosis. The pathogenesis of ascites in liver disease is secondary to renal sodium and water retention.Several factors are involved.
Sodium and water retention results from peripheral arterial vasodilatation and consequent reduction in the effective blood volume.
Portal hypertension exerts a local hydrostatic pressure and leads to increased hepatic and splanchnic production of lymph and transudation of fluid into the peritoneal cavity.
Low serum albumin (a consequence of poor synthetic liver function) may further contribute by a reduction in plasma oncotic pressure.
CLINICAL PRESENTATION OF DIABETES
Presentation may be acute, subacute or asymptomatic.
Acute presentation
Young people often present with a 2–6-week history and report the classic triad of symptoms:
Polyuria – due to the osmotic diuresis that results when blood glucose levels exceed the renal threshold
Thirst (polydipsia) – due to the resulting loss of fluid and electrolytes
Weight loss – due to fluid depletion and the accelerated breakdown of fat and muscle secondary to insulin deficiency.
Ketonuria is often present in young people and may progress to ketoacidosis if these early symptoms are not recognized and treated.
Subacute presentation
The clinical onset may be over several months or years, particularly in older patients. Thirst, polyuria and weight loss are typically present but patients may complain of such symptoms as lack of energy, visual blurring (owing to glucose-induced changes in refraction) or pruritus vulvae or balanitis that is due to Candida infection.
Complications as the presenting feature
These include:
Staphylococcal skin infections
Retinopathy noted during a visit to the optician
A polyneuropathy causing tingling and numbness in the feet
Erectile dysfunction
Arterial disease , resulting in myocardial infarction or peripheral gangrene.
Asymptomatic diabetes
Glycosuria or a raised blood glucose may be detected on routine examination (e.g. for insurance purposes).Polydipsia is the term given to excessive thirst and is one of the initial symptoms of diabetes. It is also usually accompanied by temporary or prolonged dryness of the mouth.
Polyphagia - Increased Appetite
Polyphagia is the medical term used to describe excessive hunger or increased appetite and is one of the 3 main signs of diabetes.
Ketonuria: A condition in which abnormally high amounts of ketones and keytone bodies (a byproduct of the breakdown of cells) are present in the urine.
Presenting problem in Neurology
Weakness
Establishing the diagnosis in a patient with weakness requires the application of basic anatomy, physiology and some pathology to the interpretation of the history and clinical findings
Weakness in only some muscles in a limb suggests a problem in the peripheral nerve(s) or motor root(s).
Weakness of the whole of one limb may be due to problems in the brachial or lumbosacral plexus, or to a central lesion.
Weakness in both lower limbs (paraparesis) or in all four limbs (tetraparesis) suggests either a spinal cord lesion or a diffuse peripheral nerve problem such as Guillain–Barré syndrome.
The paraparesis or tetraparesis of spinal cord lesions may be associated
with a specific pattern of sensory loss which gives a clue to the site of the cord lesion.
Weakness down one side of the body (hemiparesis) is almost always due to a cerebral hemisphere lesion, although it can be caused by spinal cord or brain-stem lesions.
Dizziness, vertigo and blackouts
Dizziness covers many complaints, from a vague feeling of unsteadiness to severe, acute vertigo. It is frequently used to describe light-headedness, panic, anxiety, palpitations and chronic ill-health. The real nature of this symptom must be determined.
Vertigo means the illusion of movement, a sensation of rotation or tipping. The patient feels the surroundings are spinning or moving. This is distressing and often accompanied by nausea or vomiting.
Blackout, like dizziness, is simply descriptive, implying either altered consciousness, visual disturbance or falling.
Epilepsy An epileptic seizure can be defined as: a sudden synchronous
discharge of cerebral neurones causing symptoms or signs that are apparent either to the patient or an observer.
A seizure is any clinical event caused by an abnormal electrical discharge in the brain, whilst epilepsy is the tendency to have recurrent seizures. Epilepsy should be regarded as a symptom of brain disease rather than
a disease itself. A single seizure is not epilepsy
Faints
The simple faint that over half the population experiences at some time (particularly in childhood, in youth or in pregnancy( is due to sudden reflex bradycardia with vasodilatation of both peripheral and splanchnic vasculature (neurocardiogenic or vasovagal syncope).
Collapse is a vague term, but often used. Avoid it. No serious disease is found in many patients (>20%) referred with symptoms suggestive of possible neurological conditions.
Fatigue is common: when it is an isolated symptom, neurological disease is rarely discovered. There is a borderland (sometimes contentious) between neurology and psychiatry.
Coma
Persistent loss of consciousness or coma indicates disorder of the arousal mechanisms in the brain stem and diencephalon, and indicates bilateral hemisphere or brain-stem disease.
Amnesia (Memory loss)
Loss of memory for a period of time may be due to a transient toxic, confusional state, a psychological fugue state, the post-ictal period after seizure or the syndrome known as transient global amnesia.
Dementia
It is a clinical syndrome characterised by a loss of previously acquired intellectual function in the absence of impairment of arousal. There
are many underlying causes but Alzheimer’s disease and diffuse vascular disease are the most common.
Personality change
While this is most often due to psychiatric illness, many neurological conditions present with altered personality and behaviour. This particularly applies to conditions which alter the function of the frontal lobes where control of executive function, movement and behaviour resides.
Abnormal gait
Many neurological disorders are associated with an abnormal gait and observing a patient walk can be very informative and assist in coming to a neurological diagnosis.
It is also an important element of assessing disability.Various patterns of weakness, loss of coordination and proprioceptive sensory loss produce an abnormal gait. Neurogenic gait disorders need to be distinguished
from those due to skeletal abnormalities, usually characterized by pain producing an antalgic gait, or limp.
Gaits that do not fit either pattern may be due to psychiatric disorders and are usually incompatible with any anatomical or physiological deficit.
Dysphonia
Dysphonia is the term used to describe hoarse or whispered speech. This can occur because the vocal cords fail to generate sounds properly during speech, or can be due to a higher-level problem of vocal cord operation (dystonia). The most common cause is laryngitis, but dysphonia can also result from a lesion of the 10th cranial nerve or a problem with the vocal cords.
Dysarthria
Dysarthria is characterised by poorly articulated or slurred speech and can occur in association with lesions of the cerebellum, brain-stem disease and lower cranial nerves, as well as in myasthenia and patients withmuscle disease. Dysarthric patients have no problem with choice of words, but there is a defect in delivery of speech which can sometimes be unintelligible, depending on severity of the underlying disorder.
Dysphasia
Dysphasia (also termed aphasia) is a disorder of the language content of speech. It can occur with lesions over a wide area of the dominant hemisphere.Dysphasia can be subclassified according to whether the speech output is ‘fluent’ or not. In fluent dysphasia, a normal or increased number of (wrong) words are produced, whereas in non-fluent dysphasia, verbal output is reduced.
Double vision
Double vision (diplopia) arises when eye movement is impaired so that the image of an object is not projected to homologous points on the two retinae. This may result from central disorders or from disturbance of the ocular motor nerves, muscles or the neuromuscular junction.
Ptosis
drooping of the eyelid called(ptosis) ,Various disorders may leads to ptosis.
Nystagmus
Nystagmus is the term given to describe a repetitive to-and-fro movement of the eyes. Usually the drifts are slower than the corrections giving rise to slow and fast phases. Nystagmus occurs because the control systems of the eyes are defective, causing them to drift off target;corrections then become necessary to return fixation to the object of interest, causing nystagmus.Headache and facial pain
Headache is a common presenting complaint but unless it is accompanied by other symptoms or neurological signs, is seldom associated with significant neurological disease. Nevertheless, patients suffering from headache usually fear serious brain disease and, in order to manage
them effectively, it is important to be aware of this.
The likely underlying cause of headache or facial pain can usually be identified after taking a careful history and performing the appropriate general and neurological
examinations.