Peptic ulcer disease
The term ‘peptic ulcer’ refers to an ulcer in the lower oesophagus, stomach or duodenum, in the jejunum
after surgical anastomosis to the stomach or, rarely, in the ileum adjacent to a Meckel’s diverticulum.
Ulcers in the stomach or duodenum may be acute or chronic; both penetrate the muscularis mucosae but
the acute ulcer shows no evidence of fibrosis.
Erosions do not penetrate the muscularis mucosae.
Gastric and duodenal ulcer
The prevalence of peptic ulcer (0.1–0.2%) is decreasing in many Western communities as a result of
widespread use of Helicobacter pylori eradication therapy but it remains high in developing countries.
The male-to-female ratio for duodenal ulcer varies from 5 : 1 to 2 : 1, while that for gastric ulcer is 2 : 1 or
less.
Chronic gastric ulcer is usually single; 90% are situated on the lesser curve within the antrum or at the
junction between body and antral mucosa.
Chronic duodenal ulcer usually occurs in the first part of the duodenum and 50% are on the anterior wall.
Gastric and duodenal ulcers coexist in 10% of patients and more than one peptic ulcer is found in 10–15%
of patients.
Pathophysiology
H. pylori
Peptic ulceration is strongly associated with H. pylori infection. The prevalence of the infection in
developed nations rises with age and in the UK approximately 50% of people over the age of 50 years are
infected. In the developing world infection is more common, affecting up to 90% of adults.
These infections are probably acquired in childhood by person-to-person contact. The vast majority of
colonised people remain healthy and asymptomatic, and only a minority develop clinical disease. Around
90% of duodenal ulcer patients and 70% of gastric ulcer patients are infected with H. pylori. The
remaining 30% of gastric ulcers are caused by NSAIDs and this proportion is increasing in Western
countries as a result of H. pylori eradication strategies.
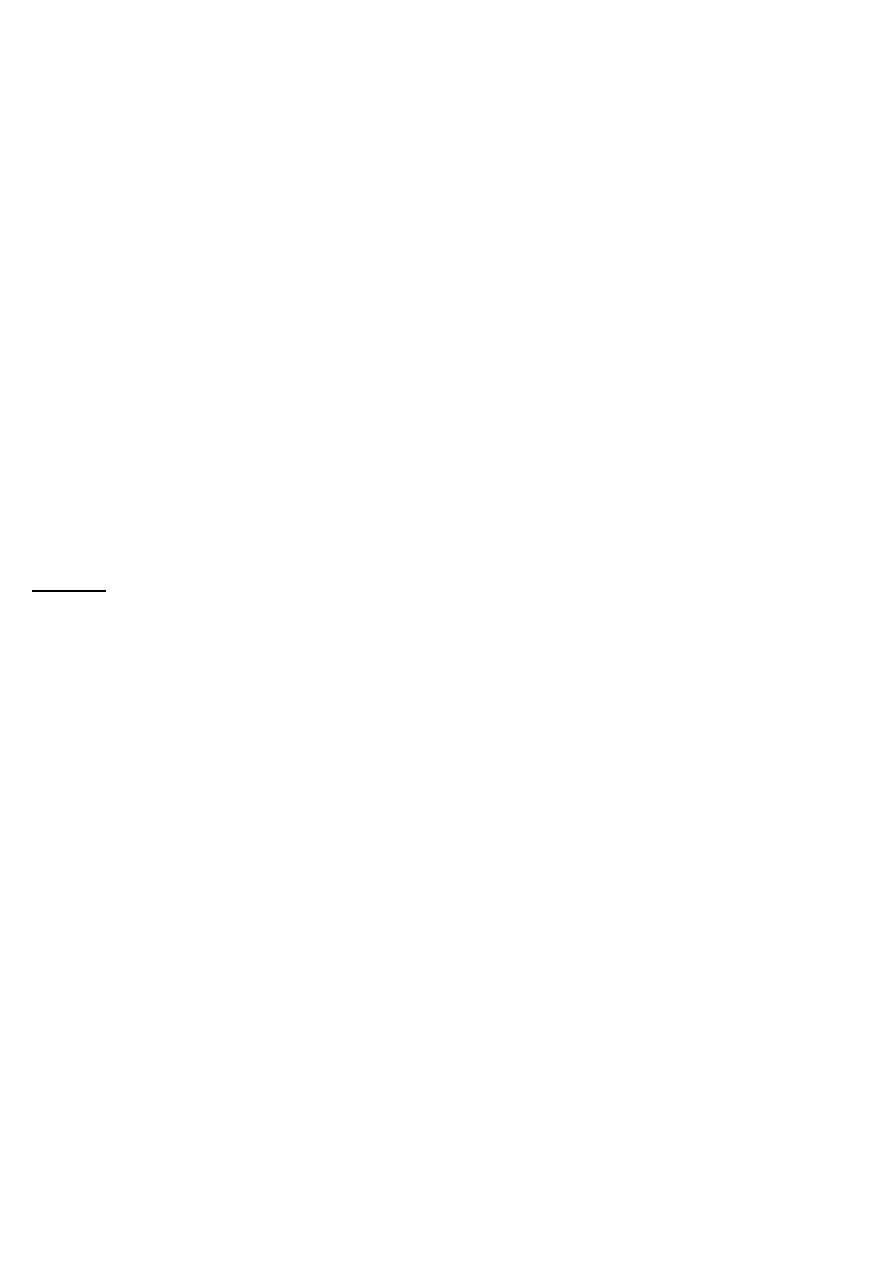
H. pylori is Gram-negative and spiral, and has multiple flagella at one end, which make it motile, allowing
it to burrow and live beneath the mucus layer adherent to the epithelial surface. It uses an adhesin
molecule (BabA) to bind to the Lewis b antigen on epithelial cells. Here the surface pH is close to neutral
and any acidity is buffered by the organism’s production of the enzyme urease. This produces ammonia
from urea and raises the pH around the bacterium and between its two cell membrane layers.
H. pylori exclusively colonises gastric-type epithelium and is found in the duodenum only in association
with patches of gastric metaplasia. It causes chronic gastritis by provoking a local inflammatory response
in the underlying epithelium .
This depends on numerous factors, notably expression of bacterial cagA and vacA genes. The CagA gene
product is injected into epithelial cells, interacting with numerous cell-signalling pathways involved in cell
replication and apoptosis. H. pylori strains expressing CagA (CagA+) are more often associated with
disease than CagA− strains. Most strains also secrete a large pore-forming protein called VacA, which
causes increased cell permeability, efflux of micronutrients from the epithelium, induction of apoptosis
and suppression of local immune cell activity. Several forms of VacA exist and pathology is most strongly
associated with the s1/ml form of the toxin. The distribution and severity of H. pylori–induced gastritis
determine the clinical outcome.
In most people, H. pylori causes a mild pangastritis with little effect on acid secretion and the majority
develop no significant clinical outcomes.
In a minority (up to 10% in the West), the infection causes an antral-predominant pattern of gastritis
characterised by hypergastrinaemia and a very exaggerated acid production by parietal cells, which could
lead to duodenal ulceration .
In a much smaller number of infected people, H. pylori causes a corpus-predominant pattern of gastritis
leading to gastric atrophy and hypochlorhydria. This phenotype is much more common in Asian countries,
particularly Japan, China and Korea. The hypochlorhydria allows other bacteria to proliferate within the
stomach; these other bacteria continue to drive the chronic inflammation and produce mutagenic nitrites
from dietary nitrates, predisposing to the development of gastric cancer .
The effects of H. pylori are more complex in gastric ulcer patients compared to those with duodenal
ulcers.
The ulcer probably arises because of impaired mucosal defence resulting from a combination of H. pylori
infection, NSAIDs and smoking, rather than excess acid.
NSAIDs
Treatment with NSAIDs is associated with peptic ulcers due to impairment of mucosal defences, as discussed on
page 1002.
Smoking
Smoking confers an increased risk of gastric ulcer and, to a lesser extent, duodenal ulcer. Once the ulcer has
formed, it is more likely to cause complications and less likely to heal if the patient continues to smoke.
Clinical features
Peptic ulcer disease is a chronic condition with spontaneous relapses and remissions lasting for decades,
if not for life.
The most common presentation is with recurrent abdominal pain that has three notable characteristics:
localisation to the epigastrium, relationship to food and episodic occurrence.
Occasional vomiting occurs in about 40% of ulcer subjects; persistent daily vomiting suggests gastric
outlet obstruction.
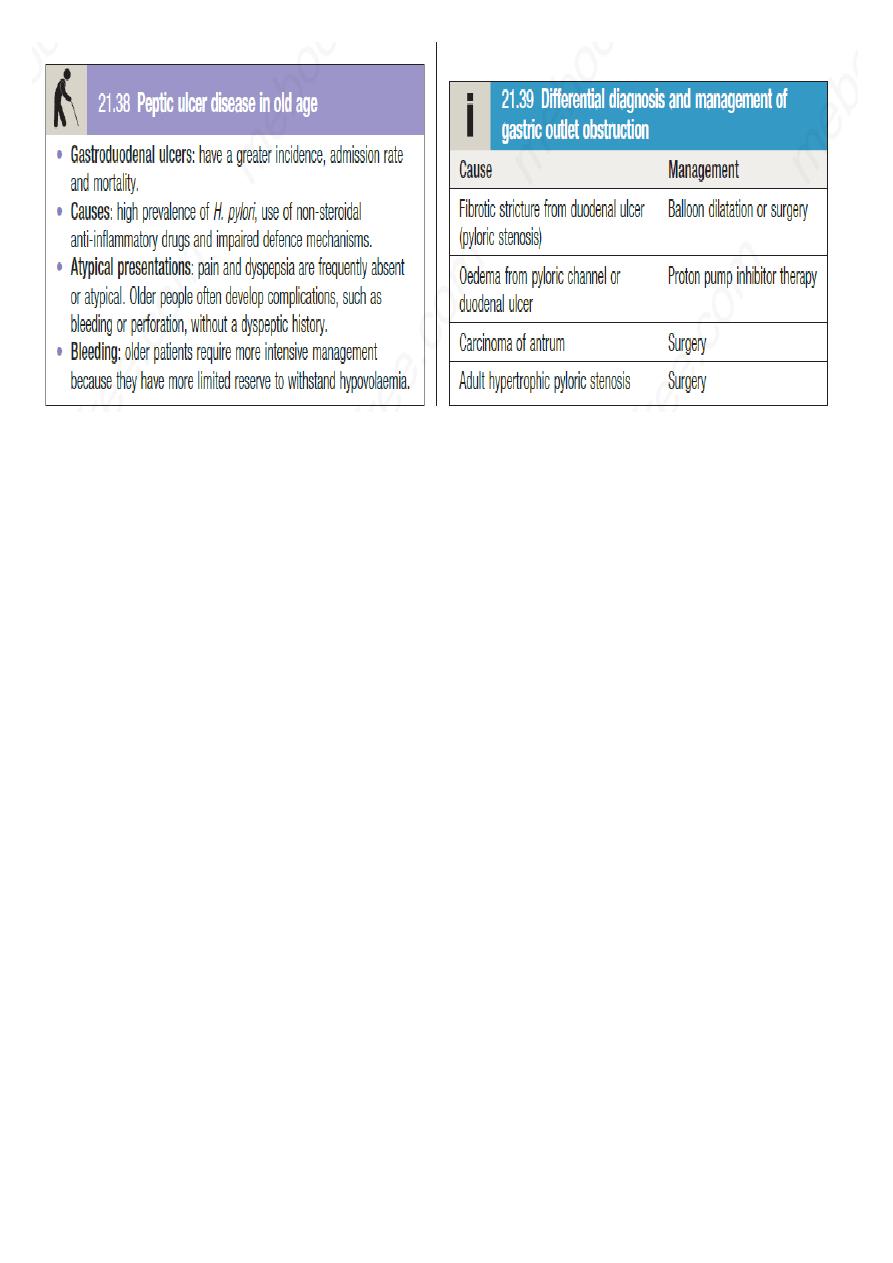
In one-third, the history is less characteristic, especially in elderly people or those taking NSAIDs. In this
situation, pain may be absent or so slight that it is experienced only as a vague sense of epigastric unease.
Occasionally, the only symptoms are anorexia and nausea, or early satiety after meals.
In some patients, the ulcer is completely ‘silent’, presenting for the first time with anaemia from chronic
undetected blood loss, as abrupt haematemesis or as acute perforation; in others, there is recurrent
acute bleeding without ulcer pain.
The diagnostic value of individual symptoms for peptic ulcer disease is poor; the history is therefore a
poor predictor of the presence of an ulcer.
Investigations
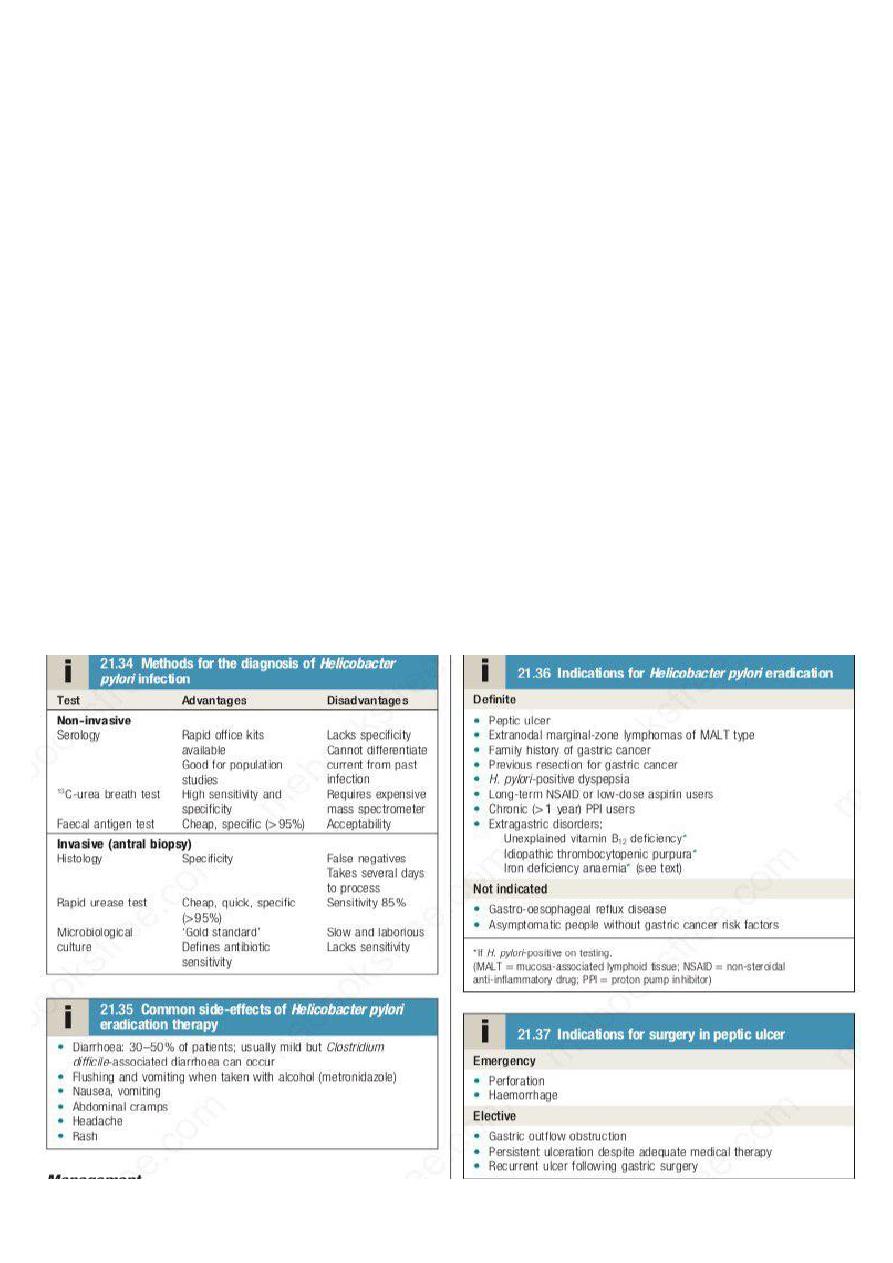
Endoscopy is the preferred investigation (Fig. 21.38). Gastric ulcers may occasionally be malignant and therefore
must always be biopsied and followed up to ensure healing. Patients should be tested for H. pylori infection. The
current options available are listed in Box 21.34. Some are invasive and require endoscopy; others are non-
invasive. They vary in sensitivity and specificity. Breath tests or faecal antigen tests are best because of accuracy,
simplicity and non-invasiveness.

Management
The aims of management are to relieve symptoms, induce healing and prevent recurrence.
H. pylori eradication is the cornerstone of therapy for peptic ulcers, as this will successfully prevent relapse and
eliminate the need for long-term therapy in the majority of patients.
H. pylori eradication
All patients with proven ulcers who are H. pylori-positive should be offered eradication as primary
therapy. Treatment is based on a PPI taken simultaneously with two antibiotics (from amoxicillin,
clarithromycin and metronidazole) for at least 7 days.
High-dose, twice-daily PPI therapy increases efficacy of treatment, as does extending treatment to 10–14
days. Success is achieved in 80–90% of patients, although adherence, side-effects and antibiotic
resistance influence this.
Resistance to amoxicillin is rare but rates of metronidazole resistance reach more than 50% in some
countries and rates of clarithromycin resistance of 20–40% have recently become common. Where the
latter exceed 15%,
a quadruple therapy regimen, consisting of omeprazole (or another PPI), bismuth subcitrate,
metronidazole and tetracycline (OBMT) for 10–14 days, is recommended. In areas of low clarithromycin
resistance, this regimen should also be offered as second-line therapy to those who remain infected after
initial therapy, once adherence has been checked.
For those who are still colonised after two treatments, the choice lies between a third attempt guided by
antimicrobial sensitivity testing, rescue therapy (levofloxacin, PPI and clarithromycin) or long-term acid
suppression.
H. pylori and NSAIDs are independent risk factors for ulcer disease and patients requiring long-term
NSAID therapy should first undergo eradication therapy to reduce ulcer risk.
Subsequent co-prescription of a PPI along with the NSAID is advised but is not always necessary for
patients being given low-dose aspirin, in whom the risk of ulcer complications is lower.
Eradication of the infection has proven benefits in several extragastric disorders, including unexplained
B12 deficiency and iron deficiency anaemia, once sources of gastrointestinal bleeding have been looked
for and excluded.
Platelet counts improve and may normalise after eradication therapy in patients with idiopathic
thrombocytopenic purpura (p. 979); the mechanism for this is unclear.
General measures
Cigarette smoking, aspirin and NSAIDs should be avoided. Alcohol in moderation is not harmful and no
special dietary advice is required.
Maintenance treatment
Continuous maintenance treatment should not be necessary after successful H. pylori eradication. For the
minority who do require it, the lowest effective dose of PPI should be used.

Complications of peptic ulcer disease
Perforation
When perforation occurs, the contents of the stomach escape into the peritoneal cavity, leading to
peritonitis. This is more common in duodenal than in gastric ulcers and is usually found with ulcers on the
anterior wall. About one-quarter of all perforations occur in acute ulcers and NSAIDs are often
incriminated.
Perforation can be the first sign of ulcer and a history of recurrent epigastric pain is uncommon.
The most striking symptom is sudden, severe pain; its distribution follows the spread of the gastric
contents over the peritoneum.
The pain initially develops in the upper abdomen and rapidly becomes generalised; shoulder tip pain is
caused by irritation of the diaphragm. The pain is accompanied by shallow respiration, due to limitation
of diaphragmatic movements, and by shock.
The abdomen is held immobile and there is generalised ‘board-like’ rigidity. Bowel sounds are absent and
liver dullness to percussion decreases due to the presence of gas under the diaphragm.
After some hours, symptoms may improve, although abdominal rigidity remains. Later, the patient’s
condition deteriorates as general peritonitis develops.
In at least 50% of cases, an erect chest X-ray shows free air beneath the diaphragm (see Fig. 21.11B, p.
773). If not, a water-soluble contrast swallow will confirm leakage of gastroduodenal contents.
After resuscitation, the acute perforation should be treated surgically, either by simple closure or by
conversion of the perforation into a pyloroplasty if it is large. On rare occasions, a ‘Polya’ partial
gastrectomy is required. Following surgery, H. pylori should be treated (if present) and NSAIDs avoided.
Perforation carries a mortality of 25%, reflecting the advanced age and significant comorbidity of the
population that are affected.
Gastric outlet obstruction
The causes are shown in Box 21.39. The most common is an ulcer in the region of the pylorus. The
presentation is with nausea, vomiting and abdominal distension. Large quantities of gastric content are
often vomited and food eaten 24 hours or more previously may be recognised.
Physical examination may show evidence of wasting and dehydration. A succussion splash may be elicited
4 hours or more after the last meal or drink. Visible gastric peristalsis is diagnostic of gastric outlet
obstruction.
Loss of acidic gastric contents leads to alkalosis and dehydration with low serum chloride and potassium
and raised serum bicarbonate and urea concentrations (hypochloraemic metabolic alkalosis).
Paradoxical
aciduria occurs because of enhanced renal absorption of Na+ in exchange for H+.
Endoscopy should be performed after the stomach has been emptied using a wide-bore nasogastric tube.
Intravenous correction of dehydration is undertaken and, in severe cases, at least 4 L of isotonic saline
and 80 mmol of potassium may be necessary during the first 24 hours. In some patients, PPI drugs heal
ulcers, relieve pyloric oedema and overcome the need for surgery. Endoscopic balloon dilatation of
benign stenoses may be possible in some patients but in others partial gastrectomy is necessary; this is
best done after a 7-day period of nasogastric aspiration, which enables the stomach to return to normal
size. A gastroenterostomy is an alternative operation but, unless this is accompanied by vagotomy,
patients will require long-term PPI therapy to prevent stomal ulceration.