4
TH
stage.Lec 3 GIT أ.م.د.حسن الجميلي
Functional dyspepsia
chronic dyspepsia in the absence of organic disease. Symptoms include early satiety,
fullness, bloating and nausea.
Pathophysiology
The cause is poorly understood but probably there is spectrum of mucosal, motility
and psychiatric disorders.
Clinical features
usually young (< 40 years) and women are affected twice as commonly as men.
Abdominal discomfort and nausea, satiety and bloating after meals. Morning
symptoms are characteristic and pain or nausea may occur on waking.
DDX: irritable bowel syndrome, Peptic ulcer disease in older subjects intra-
abdominal malignancy.
▲There are no diagnostic signs, apart perhaps from inappropriate tenderness on
abdominal palpation. Symptoms may appear disproportionate to clinical well-being
and there is no weight loss. Patients often appear anxious.
▲A drug history should be taken and the possibility of a depressive illness should be
considered.
▲ Pregnancy should be ruled out in young women before radiological studies are
undertaken.
▲ Alcohol misuse should be suspected when early morning nausea and retching are
prominent.
Investigations
1-The history will often suggest the diagnosis.
2-All patients should be checked for H. pylori infection
3-patients over the age of 55 years should undergo endoscopy to exclude mucosal
disease.
4-an ultrasound scan may detect gallstones, these are rarely responsible for
dyspeptic symptoms.
Management
▲explanation and reassurance. Possible psychological factors should be Explored.
▲Up to 10% of patients benefit from H. pylori eradication and this should be offered
to infected patients.
▲ Drug treatment is not especially successful. Antacids are sometimes helpful.
Prokinetic drugs, such as metoclopramide or domperidone, may be given before
meals if nausea, vomiting or bloating is prominent.. H2-receptor antagonist drugs
may be tried if night pain or heartburn is troublesome. Low-dose tricyclic agents,
such as amitriptyline, are of value in up to two-thirds.
Gastroparesis
Defective gastric emptying without mechanical obstruction of the stomach or
duodenum.
Primary : due to inherited or acquired disorders of the gastric pacemaker
secondary :
▲disorders of autonomic nerves (particularly diabetic neuropathy)
▲gastroduodenal musculature (systemic sclerosis, myotonic dystrophies and
amyloidosis).
▲Drugs such as opiates, calcium channel antagonists and those with anticholinergic
activity (tricyclics, phenothiazines) can also cause gastroparesis.
C.F: Early satiety and recurrent vomiting are the major symptoms; abdominal
fullness and a succussion splash may be present on examination.
Treatment is based upon small, frequent, low-fat meals
-use of metoclopramide and domperidone.
-Insevere cases, nutritional failure can occur and long-term jejunostomy feeding or
total TPN is required.
-Surgical insertion of a gastric neuro stimulator has been successful in some cases,
especially those complicating diabetic autonomic neuropathy.
SYN
Irritable bowel syndrome (IBS)
Recurrent abdominal pain in association with abnormal defecation in the absence of
a structural abnormality of the gut. Young women are affected 2–3 times more often
than men. Coexisting conditions, such as non-ulcer dyspepsia, chronic fatigue
syndrome, dysmenorrhoea and fibromyalgia, are common.
Pathophysiology
1-Behavioural and psychosocial factors:
50% of patients referred to hospital have a psychiatric illness, such as anxiety,
depression, somatisation and neurosis. Panic attacks are also common. Acute
psychological stress and overt psychiatric disease are known to alter visceral
perception and gastrointestinal motility.
2-Physiological factors
IBS may be a serotoninergic (5-HT) disorder, as evidenced by relatively excessive
release of 5-HT in diarrhoea-predominant IBS (D-IBS) and relative deficiency with
constipation-predominant IBS (C-IBS). Accordingly, 5-HT3 receptor antagonists are
effective in D-IBS, while 5-HT4 agonists improve bowel function in C-IBS. There is
some evidence that IBS may represent a state of low-grade gut inflammation or
immune activation, not detectable by tests, with raised numbers of mucosal mast
cells, which sensitise enteric neurons by releasing histamine and tryptase. Some
patients respond positively to mast cell stabilisers, such as ketotifen, which supports
a pathogenic role of mast cells in at least some patients. Immune activation may be
associated with altered CNS processing of visceral pain signals. This is more common
in women and in D-IBS, and may be triggered by a prior episode of gastroenteritis
with Salmonella or Campylobacter species.
3-Luminal factors
Both quantitative and qualitative alterations in intestinal bacterial contents (the gut
microbiota) have been reported. Small intestinal bacterial overgrowth (SIBO) may be
present in some patients and lead to symptoms.This ‘gut dysbiosis’ may explain the
response to probiotics or the non-absorbable antibiotic rifaximin that has been
reported in trials. Dietary factors are also important. Some patients have chemical
food intolerances (not allergy) to poorly absorbed, short-chain carbohydrates
(lactose, fructose and sorbitol, among others), collectively known as FODMAPs
(fermentable oligo-, di- and monosaccharides, and polyols). Their fermentation in
the colon leads to bloating, pain, wind and altered bowel habit. Noncoeliac gluten
sensitivity (negative coeliac serology and normal duodenal biopsies) seems to be
present in some IBS patients, while others may be intolerant of chemicals such as
salicylates or benzoates, found in certain foods.

Clinical features
Rome III criteria for diagnosis of irritable bowel syndrome:
Recurrent abdominal pain or discomfort at least 3 days/mth in the last 3 months,
associated with two or more of the following:
• Improvement with defecation
• Onset associated with a change in frequency of stool
• Onset associated with a change in form (appearance) of stool.
This is usually colicky or cramping in nature, felt in the lower abdomen and relieved
by defecation. Abdominal bloating worsens throughout the day; . The bowel habit is
variable. Most patients alternate between episodes of diarrhea and constipation, but
it is useful to classify patients as having predominantly constipation or
predominantly diarrhoea. Those with constipation tend to pass infrequent pellety
stools, usually in association with abdominal pain or proctalgia. Those with diarrhoea
have frequent defecation but produce low-volume stools and rarely have nocturnal
symptoms. Passage of mucus is common but rectal bleeding does not occur. Patients
do not lose weight and are constitutionally well. Physical examination is generally
unremarkable, with the exception of variable tenderness to palpation.
Diagnosis
supporting a diagnosis of IBS
• Symptoms > 6 mths
• Frequent consultations for non-gastrointestinal problems
• Previous medically unexplained symptoms
• Stress worsens symptoms
Alarm features
• Age > 50 yrs; male gender
• Weight loss
• Nocturnal symptoms
• Family history of colon cancer
• Anaemia
• Rectal bleeding
♠Full blood count and faecal calprotectin, with or without sigmoidoscopy, are usually
done and are normal in IBS.
♠Colonoscopy should be undertaken in older patients (over 40 years of age) to
exclude colorectal cancer. Endoscopic examination is also required in patients who
report rectal bleeding to exclude colon cancer and IBD. Those who present atypically
require investigations to exclude other gastrointestinal diseases.
♠ Diarrhoea predominant patients justify investigations to exclude coeliac disease ,
microscopic colitis lactose intolerance ,bile acid malabsorption , thyrotoxicosis and,
in developing countries, parasitic infection
Management
♠The most important steps are to make a positive diagnosis and reassure the
patient.
♠In patients who fail to respond to reassurance, treatment is traditionally tailored to
the predominant symptoms . Up to 20% may benefit from a wheat-free diet, some
may respond to lactose exclusion, and excess intake of caffeine or artificial
sweeteners, such as sorbitol, should be addressed. A more restrictive, ‘low-
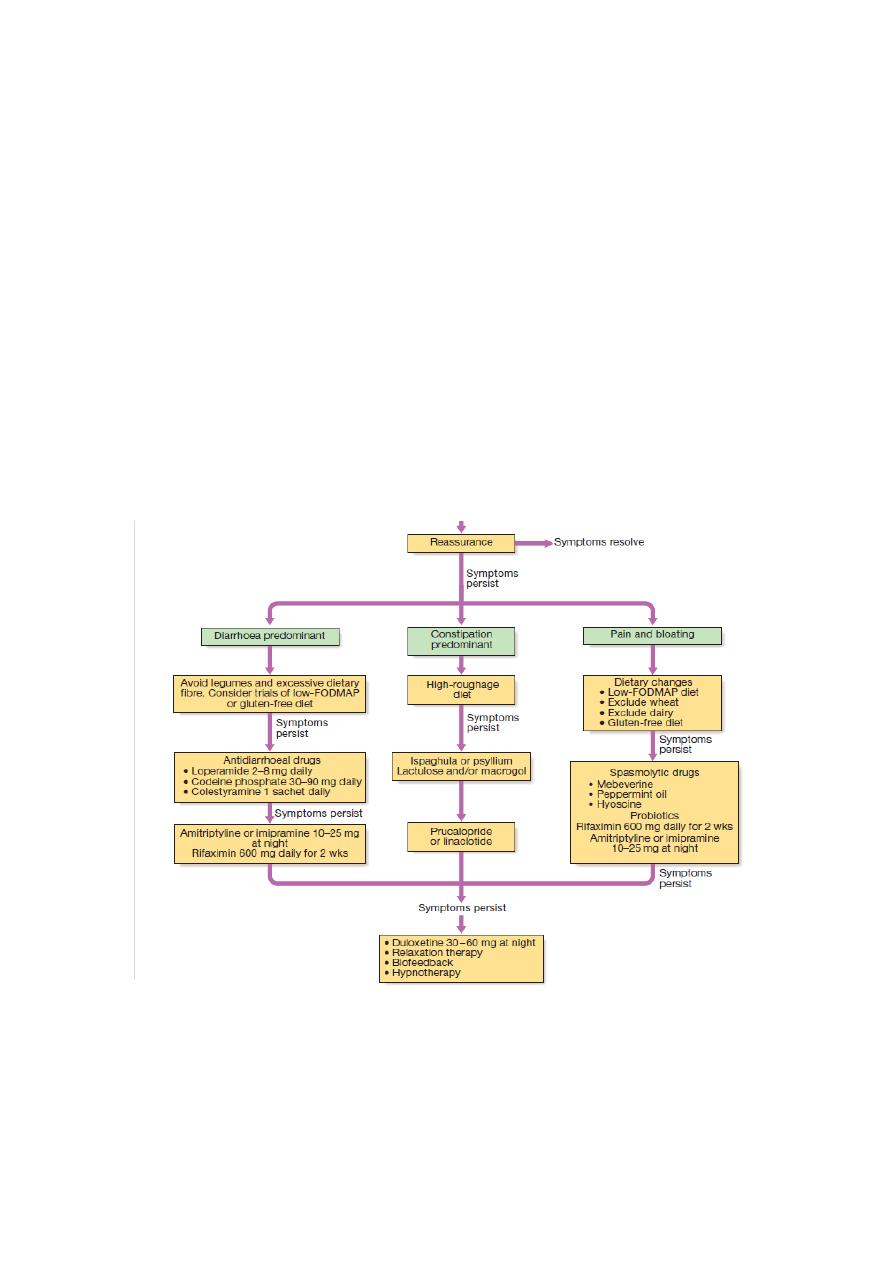
FODMAP’ diet, supervised by a dietitian, with gradual re-introduction of different
food groups, may help some patients, as may a trial of a gluten-free diet.
♠Probiotics, in capsule form, can be effective if taken for several months in patients
with intractable symptoms.
♠sometimesbenefit from several months of therapy with a tricyclic antidepressant,
such as amitriptyline or imipramine . It may act by reducing visceral sensation and
by altering gastrointestinal motility. Anxiety and affective disorders may also require
specific treatment.
♠The 5-HT4 agonist prucalopride, the guanylate cyclase-C receptor agonist
linaclotide, and chloride channel activators, such as lubiprostone, can be effective in
constipation predominant IBS.
♠Trials of anti-inflammatory agents, such as ketotifen or mesalazine, and the
antibiotic rifaximin may be considered in some patients with difficult symptoms but
are best prescribed only after specialist referral.
♠Psychological interventions, such as cognitive behavioural therapy, relaxation and
gut-directed hypnotherapy, should be reserved for the most difficult cases.
IBS
Functional causes of vomiting
Psychogenic retching or vomiting may arise in anxiety. It typically occurs on
wakening or immediately after breakfast and only rarely later in the day. The
disorder . Early morning vomiting also occurs in pregnancy, alcohol misuse and
depression. Although functional vomiting may occur regularly over long periods,
there is little or no weight loss.. The cause of this cyclical vomiting syndrome is
unknown, but in some adults it is associated with cannabis use. In all patients, it is
essential to exclude other common causes. Tranquillisers and antiemetic drugs
(metoclopramide, domperidone, prochlorperazine have only a secondary place in
management. Antidepressants in full dose may be effective…
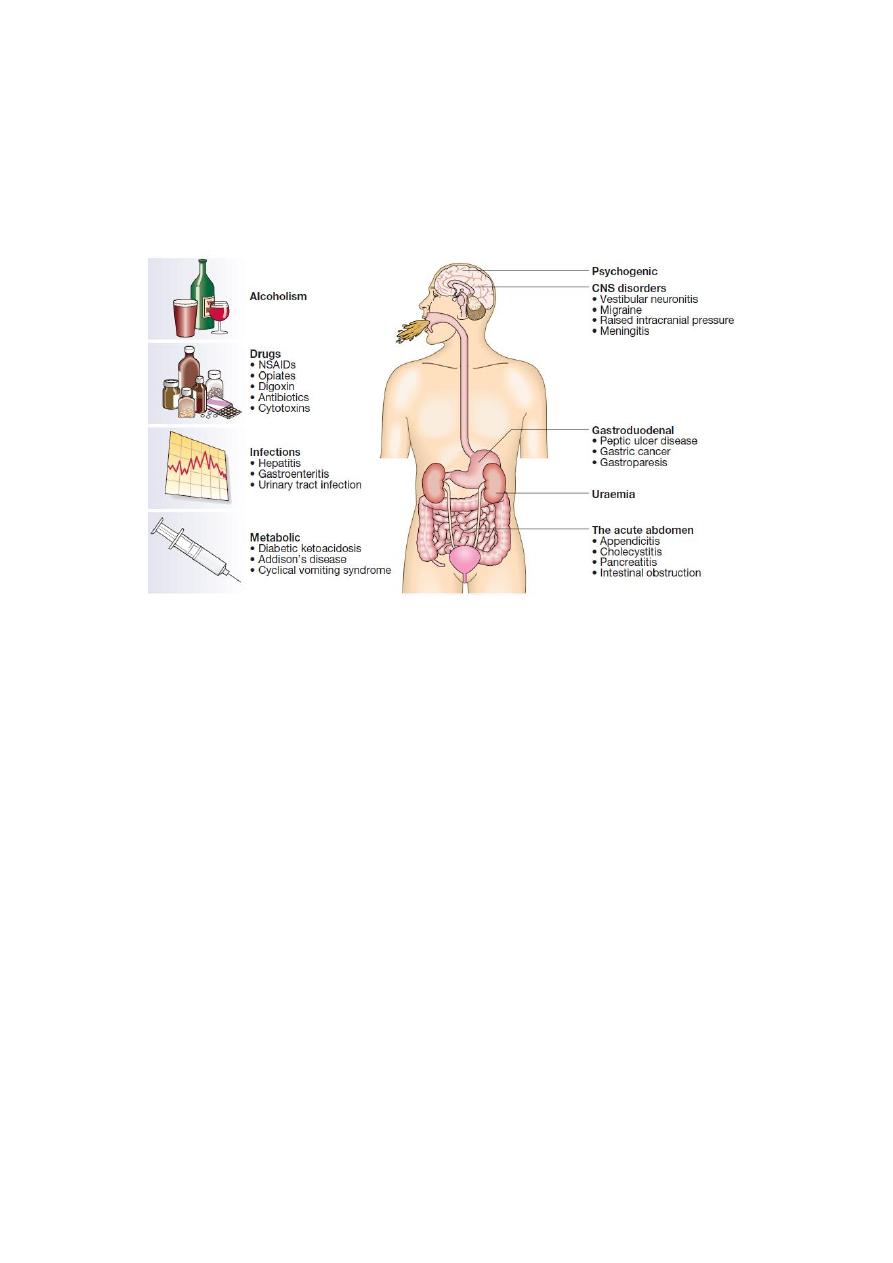
Causes of vomiting: