Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
Graves’ disease
Graves’ disease can occur at any age but is unusual before puberty and most
commonly affects women aged 30–50 years .The most common
manifestation is thyrotoxicosis with or without a diffuse goitre. Graves’
disease also causes ophthalmopathy and, rarely, pretibial myxoedema .
These extrathyroidal features usually occur in thyrotoxic patients but can
arise in the absence of thyroid dysfunction.
Graves’ thyrotoxicosis
Pathophysiology
The thyrotoxicosis results from the production of immunoglobulin G (IgG)
antibodies directed against the TSH receptor on the thyroid follicular cell,
which stimulate thyroid hormone production and proliferation of follicular
cells, leading to goitre in the majority of patients. These antibodies are
termed thyroid-stimulating immunoglobulins or TSH receptor antibodies
(TRAb) and can be detected in the serum of 80–95% of patients with
Graves’ disease.
The concentration of TRAb in the serum is presumed to fluctuate to account
for the natural history of Graves’ thyrotoxicosis . Thyroid failure seen in
some patients may result from the presence of blocking antibodies against
the TSH receptor, and from tissue destruction by cytotoxic antibodies and
cell-mediated immunity Graves’ disease has a strong genetic component.
A suggested trigger for the development of thyrotoxicosis in genetically
susceptible individuals may be infection with viruses or bacteria. Certain
strains of the gut organisms Escherichia coli and Yersinia enterocolitica
possess cell membrane TSH receptors and it has been suggested that
antibodies to these microbial antigens may cross-react with the TSH
receptors on the host thyroid follicular cell. In regions of iodine deficiency
,iodine supplementation can precipitate thyrotoxicosis, but only in those with
pre-existing subclinical Graves’ disease.
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
Smoking is weakly associated with Graves’ thyrotoxicosis but strongly
linked with the development of ophthalmopathy.
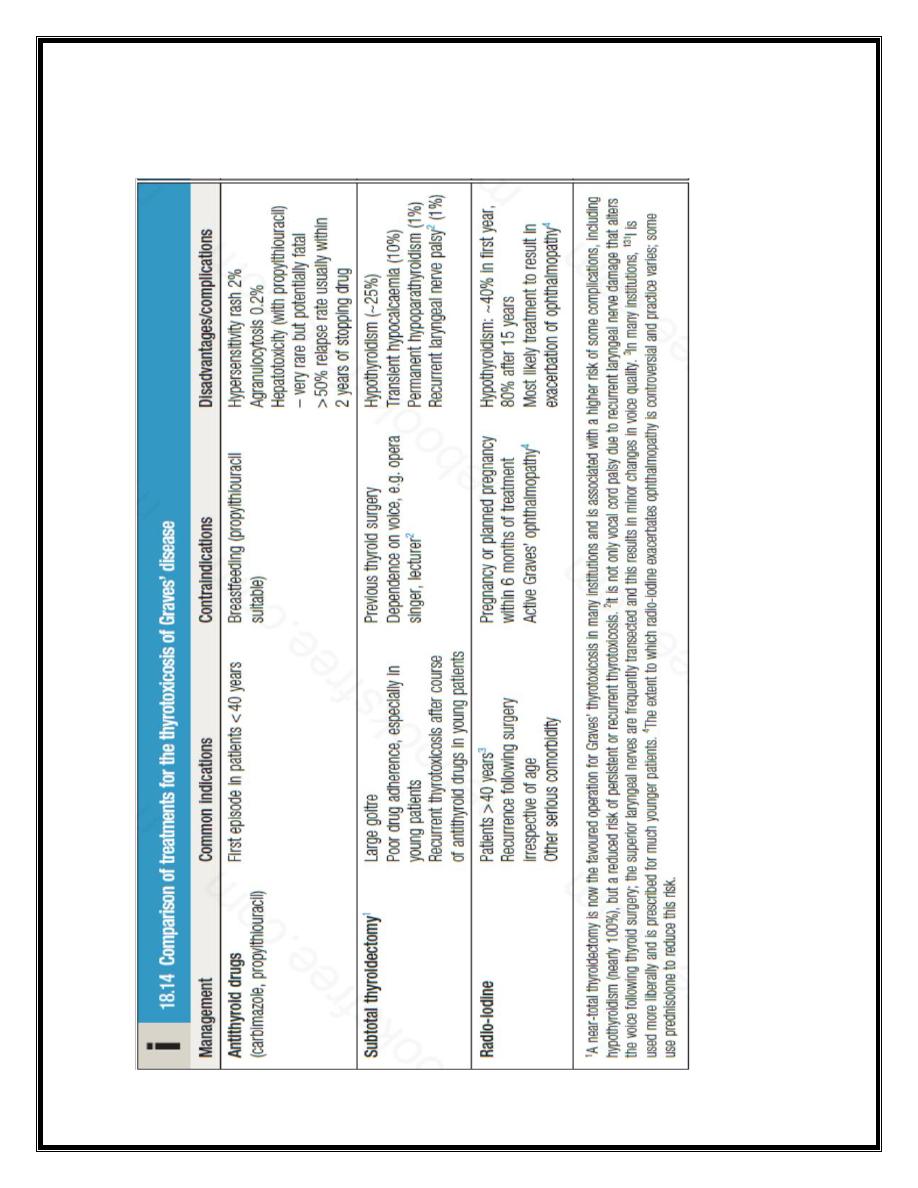
Management
Symptoms of thyrotoxicosis respond to β-blockade but definitive treatment
requires control of thyroid hormone secretion.
Some clinicians adopt an empirical approach of prescribing a course of
antithyroid drug therapy and then recommending 131I or surgery if relapse
occurs.
Antithyroid drugs
:The most commonly used are carbimazole and its active
metabolite, methimazole ,the Propylthiouracil is equally effective. These
drugs reduce the synthesis of new thyroid hormones by inhibiting the
iodination of tyrosine . Carbimazole also has an immunosuppressive action,
leading to a reduction in serum TRAb concentrations, but this is not enough
to influence the natural history of the thyrotoxicosis significantly.
Antithyroid drugs should be introduced at high doses (carbimazole 40–60
mg daily or propylthiouracil 400–600 mg daily). Usually, this results in
subjective improvement within 10–14 days and renders the patient clinically
and biochemically euthyroid at 6–8 weeks. At this point, the dose can be
reduced and titrated to maintain T4 and TSH within their reference range.
In most patients, carbimazole is continued at 5–20 mg per day for 12–18
months in the hope that remission will occur. Between 50% and 70% of
patients with Graves’s disease will subsequently relapse, usually within 2
years of stopping treatment. Risk factors for relapse include younger age,
male sex, presence of a goitre, and higher TRAb titres at both diagnosis and
cessation of antithyroid therapy.
Antithyroid drugs can have adverse effects. The most common is a rash.
Agranulocytosis is a rare but potentially serious complication that cannot be
predicted by routine measurement of white blood cell count but which is
reversible on stopping treatment. Patients should be warned to stop the drug
and seek medical advice immediately, should a severe sore throat or fever
develop while on treatment. Propylthiouracil is associated with a small but
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
definite risk of hepatotoxicity, which, in some instances, has resulted in liver
failure requiring liver transplantation, and even in death. It should therefore
be considered second-line therapy to carbimazole and be used only during
pregnancy or breastfeeding , or if an adverse reaction to carbimazole has
occurred.
Thyroid surgery: Patients should be rendered euthyroid with antithyroid
drugs before operation. Oral potassium iodide, 60 mg three times daily, is
often added for 10 days before surgery to inhibit thyroid hormone release
and reduce the size and vascularity of the gland, making surgery technically
easier. Traditionally, a ‘subtotal’ thyroidectomy is performed, in which a
portion of one lobe of the thyroid is left in situ, with the aim of rendering the
patient euthyroid. While complications of surgery are rare and 80% of
patients are euthyroid, 15% are permanently hypothyroid and 5% remain
thyrotoxic. As a consequence, many endocrine surgeons now opt to perform
a ‘near-total’ thyroidectomy, leaving behind only a small portion of gland
adjacent to the recurrent laryngeal nerves. This strategy invariably results in
permanent hypothyroidism and is probably associated with a higher risk of
hypoparathyroidism, but maximises the potential for cure of thyrotoxicosis.
Radioactive iodine 131I is administered orally as a single dose and is
trapped and organified in the thyroid . 131I emits both β and γ radiation and,
although it decays within a few weeks, it has long-lasting inhibitory effects
on survival and replication of follicular cells. The variable radio-iodine
uptake and radiosensitivity of the gland means that the choice of dose is
empirical. This regimen is effective in 75% of patients within 4–12 weeks.
If thyrotoxicosis persists after 6 months, a further dose of 131I can be given.
The disadvantage of 131I treatment is that the majority of patients eventually
develop hypothyroidism.
131I is usually avoided in patients with Graves’ ophthalmopathy and
evidence of significant active orbital inflammation. It can be administered
with caution in those with mild or ‘burnt-out’ eye disease, when it is
customary to cover the treatment with a 6-week tapering course of oral
prednisolone. In women of reproductive age, pregnancy must be excluded
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
before administration of 131I and avoided for 6 months thereafter; men are
also advised against fathering children for 6 months after receiving 131I.
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
Thyrotoxicosis in pregnancy
Thyrotoxicosis in pregnancy may be associated with significant maternal
and fetal morbidity.
Hyperthyroidism
The coexistence of pregnancy and thyrotoxicosis is unusual, since
anovulatory cycles are common in thyrotoxic patients and autoimmune
disease tends to remit during pregnancy, due to suppression of the maternal
immune response. Thyroid function tests must be interpreted in the
knowledge that thyroid-binding globulin, and hence total T4 and T3 levels,
are increased in pregnancy and that the normal range for TSH is lower.
Despite this, a fully suppressed TSH is usually indicative of Graves’ disease.
When thyroid disease during pregnancy is being dealt with, both mother and
fetus must be considered, since maternal thyroid hormones, TSH receptor
antibodies (TRAb) and antithyroid drugs can all cross the placenta to some
degree, exposing the fetus to the risks of thyrotoxicosis, iatrogenic
hypothyroidism and goitre. Moreover, poorly controlled thyrotoxicosis can
result in fetal tachycardia, intrauterine growth retardation, prematurity,
stillbirth and possibly even congenital malformations.
Antithyroid drugs are the treatment of first choice for thyrotoxicosis in
pregnancy. Newly diagnosed hyperthyroidism during pregnancy can be
treated with β-adrenoceptor antagonists (β-blockers) in the short term,
followed by antithyroid drugs. Propylthiouracil (PTU) is the preferred
antithyroid drug because treatment with carbimazole during the first
trimester has been associated with the occurrence of choanal atresia and
aplasia cutis. Hyperthyroid women who become pregnant while taking
carbimaole or PTU should be advised to continue their current drug in
pregnancy, with close monitoring. Both carbimazole and PTU cross the
placenta and are effective in treating thyrotoxicosis in the fetus caused by
transplacental passage of TRAb. To avoid fetal hypothyroidism, which can
affect brain development and cause goitre, it is important to use the smallest
dose of antithyroid drug (typically < 150 mg PTU or 15 mg carbimazole per
day) that will maintain maternal free T4, T3 and TSH concentrations within
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
their respective reference ranges. Thyroid surgery is sometimes necessary
because of poor drug adherence, drug hypersensitivity or failure of medical
treatment and is most safely performed during the second trimester.
Radioactive iodine is absolutely contraindicated throughout pregnancy, as it
invariably induces fetal hypothyroidism. Frequent review of mother and
fetus (monitoring heart rate and growth) is important during pregnancy and
in the puerperium. Serum TRAb levels can be measured in the third
trimester to predict the likelihood of neonatal thyrotoxicosis. PTU is the
drug of choice in the breastfeeding mother, as it is excreted in the milk to a
much lesser extent than carbimazole. Thyroid function should be monitored
periodically in the breastfed child.
Post-partum thyroiditis
Post-partum thyroiditis typically presents 3–4 months after delivery.
The
maternal immune response, which is modified during pregnancy to allow
survival of the fetus, is enhanced after delivery and may unmask previously
unrecognised
subclinical
autoimmune
thyroid
disease.
However,
symptomatic thyrotoxicosis presenting for the first time within 12 months of
childbirth is likely to be due to post-partum thyroiditis and the diagnosis is
confirmed by a negligible radio-isotope uptake. The clinical course and
treatment are similar to those of painless subacute thyroiditis .Post-partum
thyroiditis tends to recur after subsequent pregnancies, and eventually
patients progress over a period of years to permanent hypothyroidism.
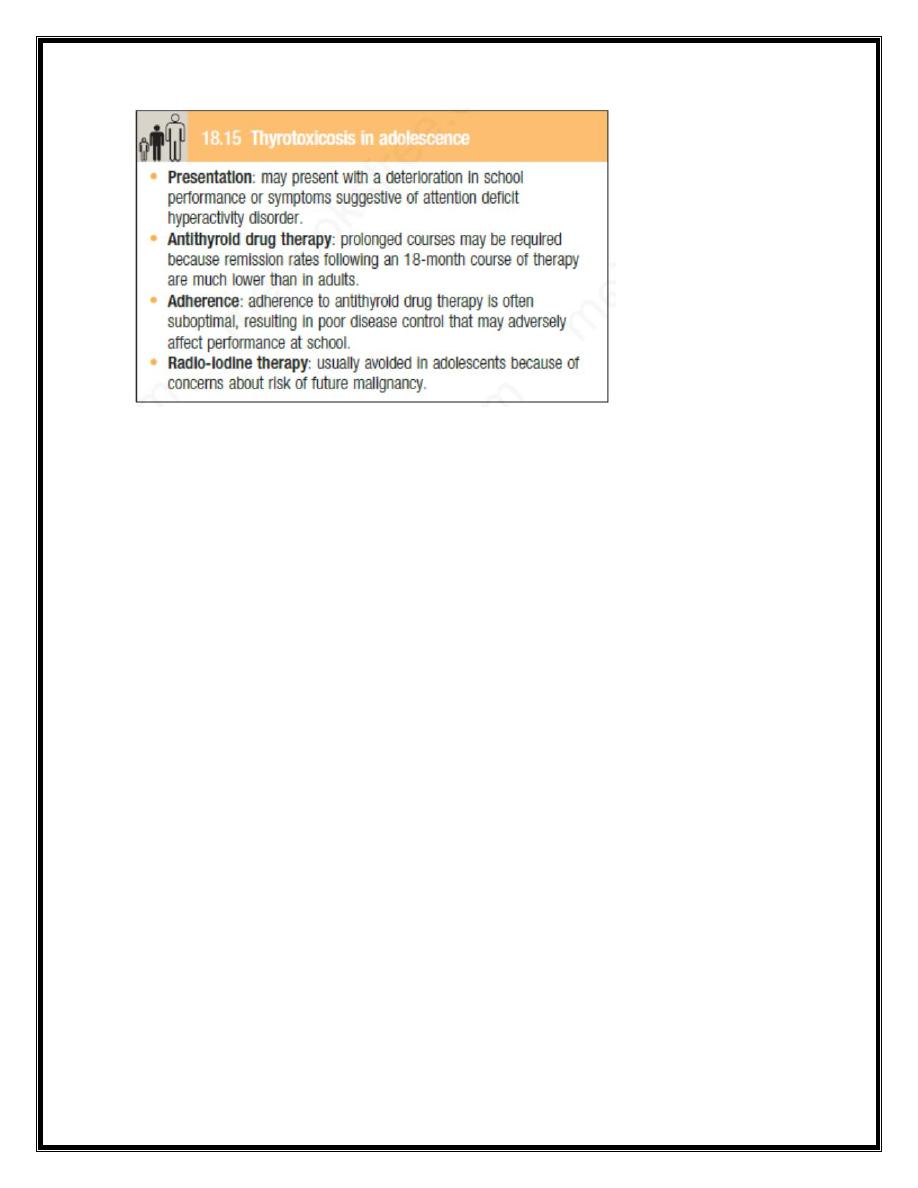
Thyrotoxicosis in adolescence
Thyrotoxicosis can occasionally occur in adolescence and is almost always
due to Graves’ disease. The presentation may be atypical and management
challenging.
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
Graves’ ophthalmopathy
This condition is immunologically mediated but the autoantigen has not
been identified. Within the orbit (and the dermis) there is cytokine-mediated
proliferation of fibroblasts that secrete hydrophilic glycosaminoglycans. The
resulting increase in interstitial fluid content, combined with a chronic
inflammatory cell infiltrate, causes marked swelling and ultimately fibrosis
of the extraocular muscles and a rise in retrobulbar pressure. The eye is
displaced forwards (proptosis, exophthalmos) and in Ophthalmopathy, like
thyrotoxicosis , typically follows an episodic course and it is helpful to
distinguish patients with active inflammation (periorbital oedema and
conjunctival inflammation with changing orbital signs) from those in whom
the inflammation has ‘burnt out’. Eye disease is detectable in up to 50% of
thyrotoxic patients at presentation, but active ocular inflammation may occur
before or after thyrotoxic episodes (exophthalmic Graves’ disease). It is
more common in cigarette smokers and is exacerbated by poor control of
thyroid function, especially hypothyroidism.
The most frequent presenting symptoms are related to increased exposure of
the cornea, resulting from proptosis and lid retraction. There may be
excessive lacrimation made worse by wind and bright light, a ‘gritty’
sensation in the eye, and pain due to conjunctivitis or corneal ulceration. In
addition, there may be reduction of visual acuity and/or visual fields as a
consequence of corneal oedema or optic nerve compression. Other signs of
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
optic nerve compression include reduced colour vision and a relative
afferent pupillary defect . If the extraocular muscles are involved and do not
act in concert, diplopia results. The majority of patients require no treatment
other than reassurance.
Smoking cessation should be actively encouraged. Methylcellulose eye
drops and gel counter the gritty discomfort of dry eyes, and tinted glasses or
side shields attached to spectacle frames reduce the excessive lacrimation
triggered by sun or wind. In patients with mild Graves’ ophthalmopathy, oral
selenium (100 μg twice daily for 6 months) improves quality of life, reduces
ocular involvement and slows progression of disease; the mechanism of
action is not known but may relate to an antioxidant effect. More severe
inflammatory episodes are treated with glucocorticoids (e.g. pulsed
intravenous methylprednisolone) and sometimes orbital radiotherapy. There
is also an increasing trend to use alternative immunosuppressive therapies,
such as rituximab and ciclosporin. Loss of visual acuity is an indication for
urgent surgical decompression of the orbit. In ‘burnt-out’ disease, surgery to
the extraocular muscles, and later the eyelids, may improve diplopia,
conjunctival exposure and cosmetic appearance.
Pretibial myxoedema
This infiltrative dermopathy occurs in fewer than 5% of patient with Graves’
disease and has similar pathological features as occur in the orbit. It takes
the form of raised pink-coloured or purplish plaques on the anterior aspect of
the leg, extending on to the dorsum of the foot . The lesions may be itchy
and the skin may have a ‘peau d’orange’ appearance with growth of coarse
hair; less commonly, the face and arms are affected. Treatment is rarely
required but in severe cases topical glucocorticoids may be helpful.