KEY LEARNING POINTS of the previous lecture:
• The pelvic inlet is wider in the transverse than in the AP diameter.
• The pelvic outlet is wider in the AP than in the transverse diameter.
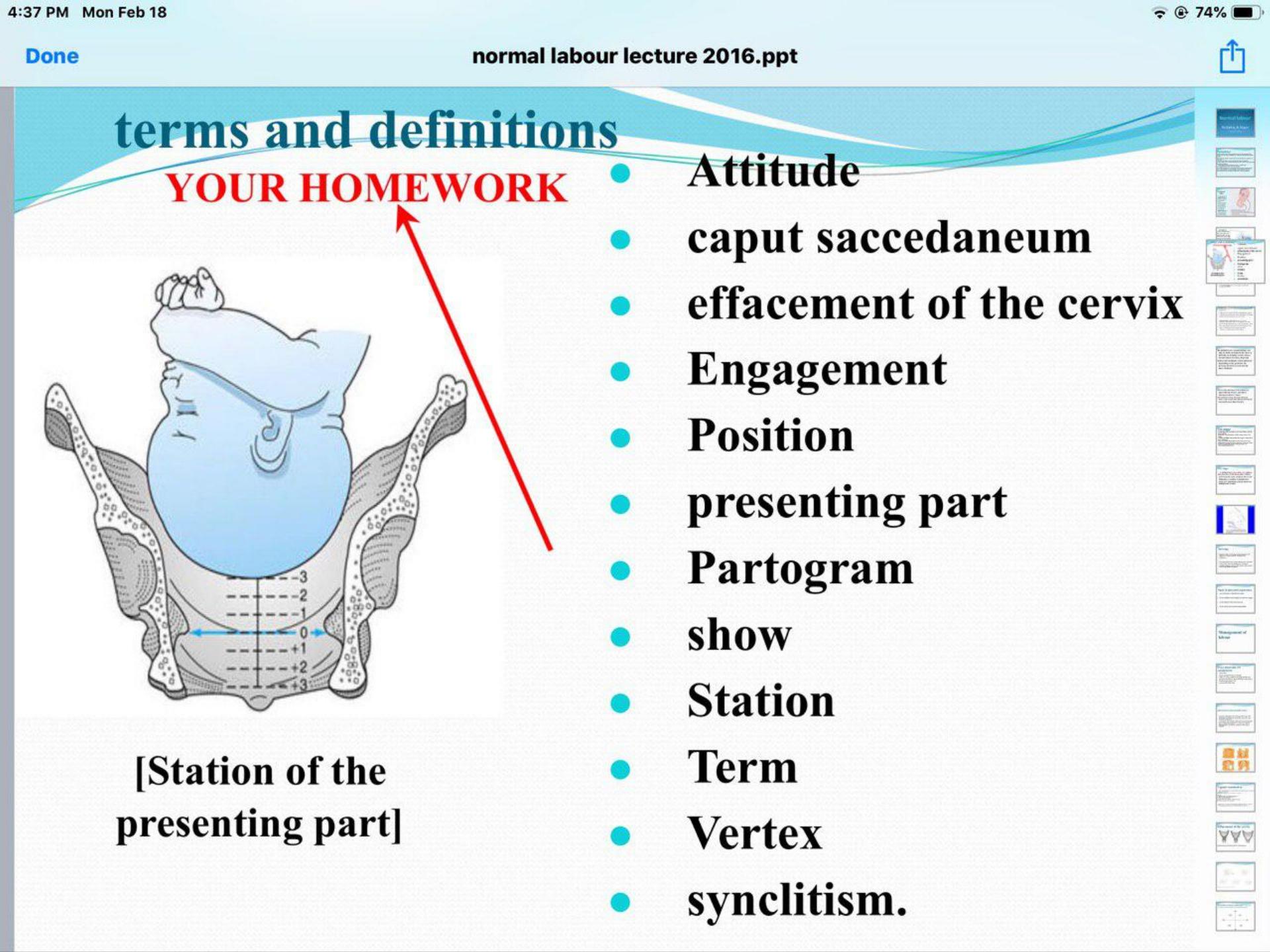
• The ischial spines are located in the midpelvis and denote station zero.
• The fetal head enters the pelvis in a transverse position, rotates in the midpelvis and
delivers in an AP position.
• Pelvic dimensions may increase during labour due to pelvic ligament laxity.
• The shape of the pelvis and pelvic floor muscles aid flexion and rotation of the fetal head.
• The sutures and fontanelles are used to assess the position and attitude of the fetal head.
• Moulding of the skull bones during labour reduces the measurements of the fetal head.
• A fetus in a flexed OA (occipito-anterior) position with a gynaecoid pelvis is most
favorable for vaginal birth.
• Perineal tissues offer resistance to delivery especially in a nulliparous woman.
Physiology of labour
The mechanisms underlying human parturition are not fully understood and differ from other
animal models that have been studied. In particular, the process that initiates labour is poorly
understood. There are a number of important elements.
The cervix, which is initially long, firm, and closed, with a protective mucus plug, must soften,
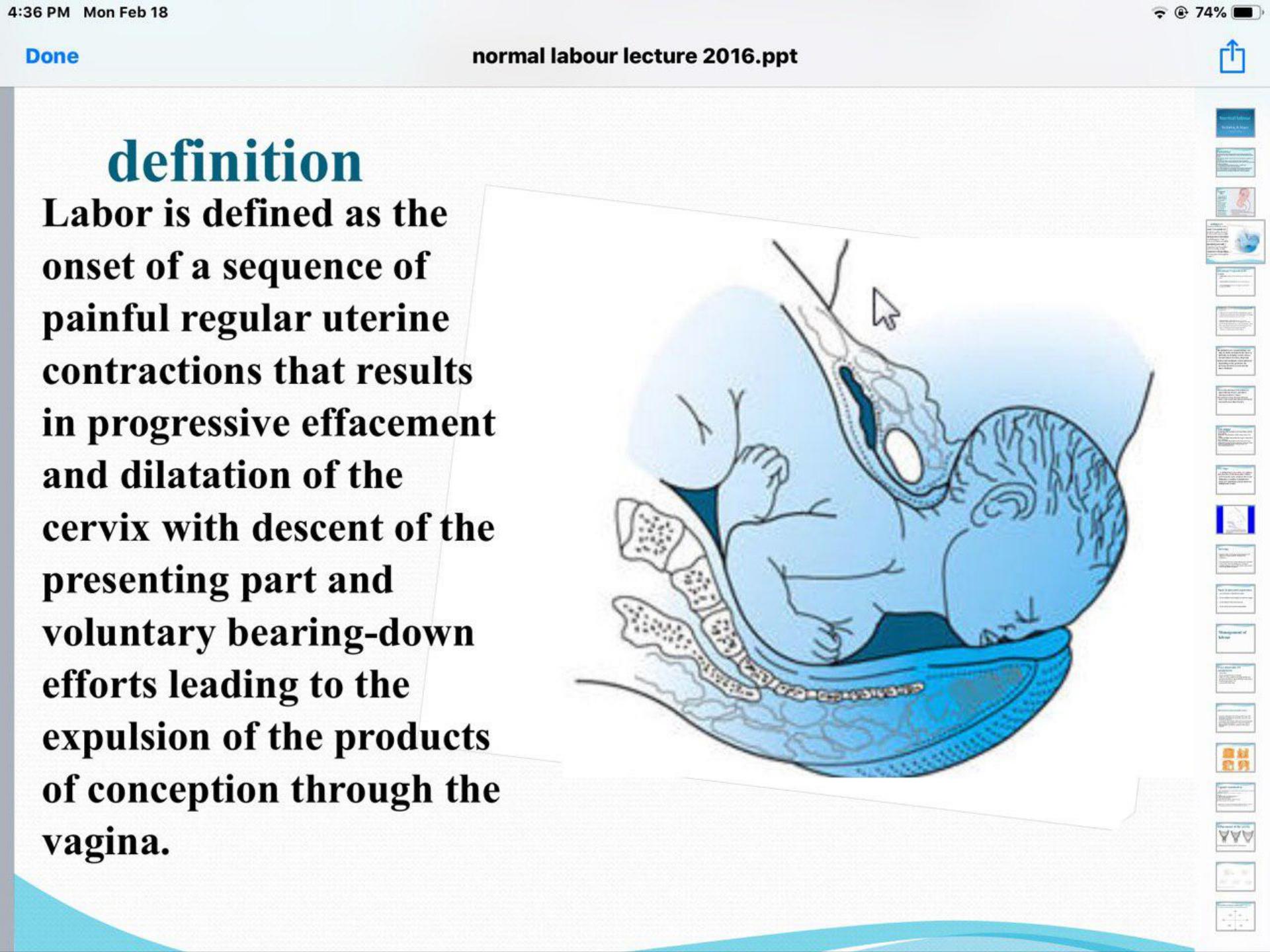
shorten, thin out (effacement) and dilate for labour to progress. The uterus must change from a
state of relaxation to an active state of regular, strong, frequent contractions to facilitate transit
of the fetus through the birth canal. Each contraction must be followed by a resting phase in
order to maintain placental blood flow and adequate perfusion of the fetus. The pressure of the
presenting part on the pelvic floor muscles as the fetus descends from the midpelvis to the
pelvic outlet produces a maternal urge to push, enhanced further by stretching of the perineum.
The onset of labour occurs when the factors that inhibit contractions and maintain a closed
cervix diminish and are overtaken by the actions of factors that do the opposite. Both mother
and fetus appear to contribute to this process.

The uterus
Myometrial cells of the uterus contain filaments of actin and myosin, which interact and bring
about contractions in response to an increase in intracellular calcium. Prostaglandins and
oxytocin increase intracellular free calcium ions, whereas beta-adrenergic compounds and
calcium-channel blockers do the opposite. Separation of the actin and myosin filaments brings
about relaxation of the myocyte; however, unlike any other muscle cell of the body, this actin–
myosin interaction occurs along the full length of the filaments so that a degree of shortening
occurs with each successive interaction. This progressive shortening of the uterine smooth
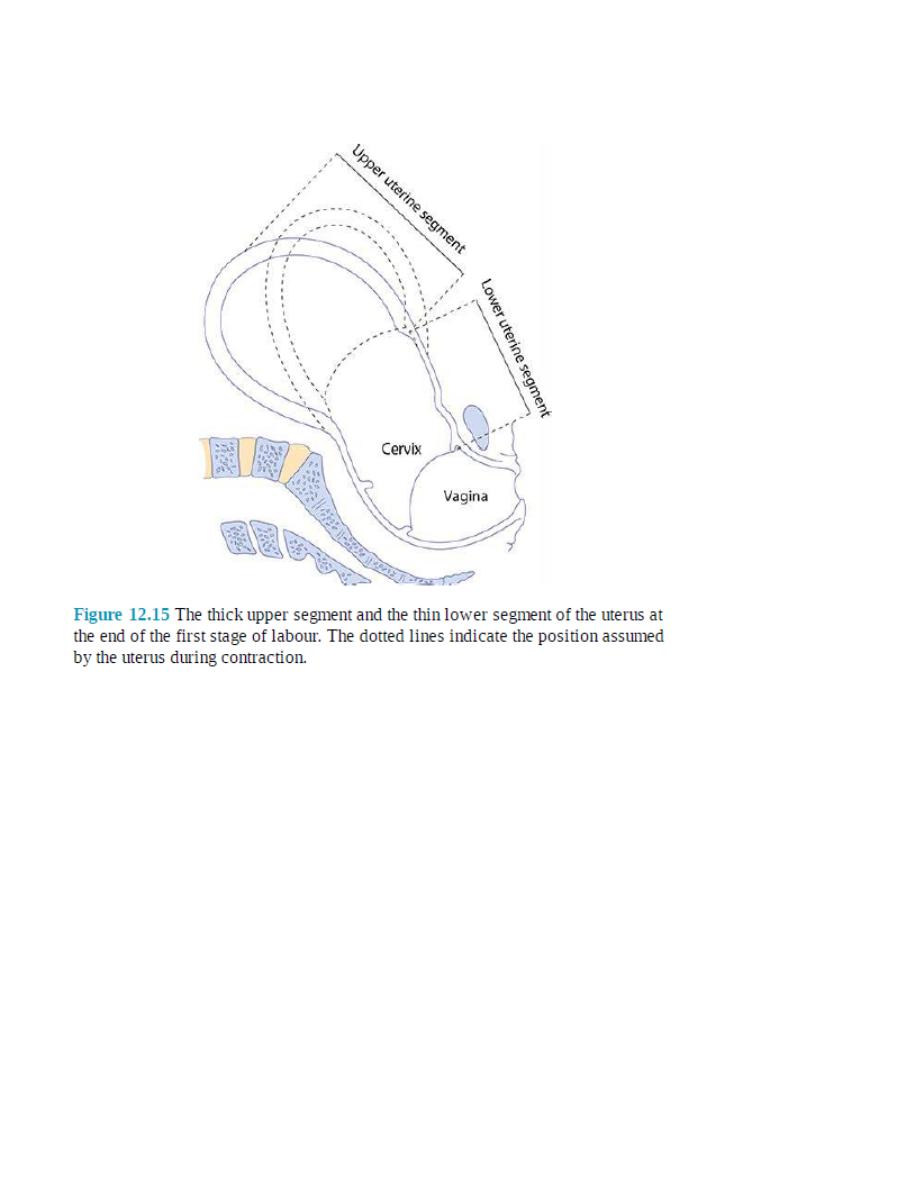
muscle cells is called retraction and occurs in the cells of the upper part of the uterus. The result
of this retraction process is the development of the thicker, actively contracting ‘upper
segment’. At the same time, the lower segment of the uterus becomes thinner and more
stretched. Eventually, this results in the cervix being ‘taken up’ (effacement) into the lower
segment of the uterus so forming a continuum with the lower uterine segment (Figure 12.15).
The cervix effaces and then dilates, and the fetus descends in response to this directional force.
It is essential that the myocytes of the uterus contract in a coordinated way.
Individual myometrial cells are laid down in a mesh of collagen. There is cell-tocell
communication by means of gap junctions, which facilitate the passage of various products of
metabolism and electrical current between cells. These gap junctions are absent for most of the
pregnancy but appear in significant numbers at term. Gap junctions increase in size and number
with the progress of labour and allow greater coordination of myocyte activity. Prostaglandins
stimulate their formation, while beta-adrenergic compounds are thought to do the opposite.
A uterine pacemaker from which contractions originate probably exists but has not been
demonstrated histologically.
Uterine contractions are involuntary in nature and there is relatively little extrauterine neuronal
control. The frequency of contractions may vary during labour and with parity. Throughout the
majority of labour, they occur at intervals of 2–4 minutes and are described in terms of the
frequency within a 10-minute period (i.e. 2 in 10 increasing to 4–5 in 10 in advanced labour).
Their duration also varies during labour, from 30 to 60 seconds or occasionally longer. The
frequency of contractions can be recorded on a cardiotocograph (CTG) using a pressure
transducer (tocodynamometer) positioned on the abdomen at the fundus of the uterus. The
intensity or amplitude of the intrauterine pressure generated with each contraction averages
between 30 and 60 mmHg.
The cervix
The cervix contains myocytes and fibroblasts separated by a ‘ground substance’ made up of
extracellular matrix molecules. Interactions between collagen, fibronectin and dermatan
sulphate (a proteoglycan) during the earlier stages of pregnancy keep the cervix firm and closed.
Contractions at this point do not bring about effacement or dilatation. Under the influence of
prostaglandins, and other humoral mediators, there is an increase in proteolytic activity and a
reduction in collagen and elastin. Interleukins bring about a proinflammatory change with a
significant invasion by neutrophils. Dermatan sulphate is replaced by the more hydrophilic
hyaluronic acid, which results in an increase in water content of the cervix. This causes cervical
softening or ‘ripening’, so that contractions, when they begin, can bring about the processes of
effacement and dilatation.

Hormonal factors
Progesterone maintains uterine relaxation by suppressing prostaglandin production, inhibiting
communication between myometrial cells and preventing oxytocin release. Oestrogen opposes
the action of progesterone. Prior to labour, there is a reduction in progesterone receptors and an
increase in the concentration of oestrogen relative to progesterone. Prostaglandin synthesis by
the chorion and the decidua is enhanced, leading to an increase in calcium influx into the
myometrial cells. This change in the hormonal milieu also increases gap junction formation
between individual myometrial cells, creating a functional syncytium, which is necessary for
coordinated uterine activity. The production of corticotrophin-releasing hormone (CRH) by the
placenta increases in concentration towards term and potentiates the action of prostaglandins
and oxytocin on myometrial contractility. The fetal pituitary secretes oxytocin and the fetal
adrenal gland produces cortisol, which stimulates the conversion of progesterone to oestrogen.
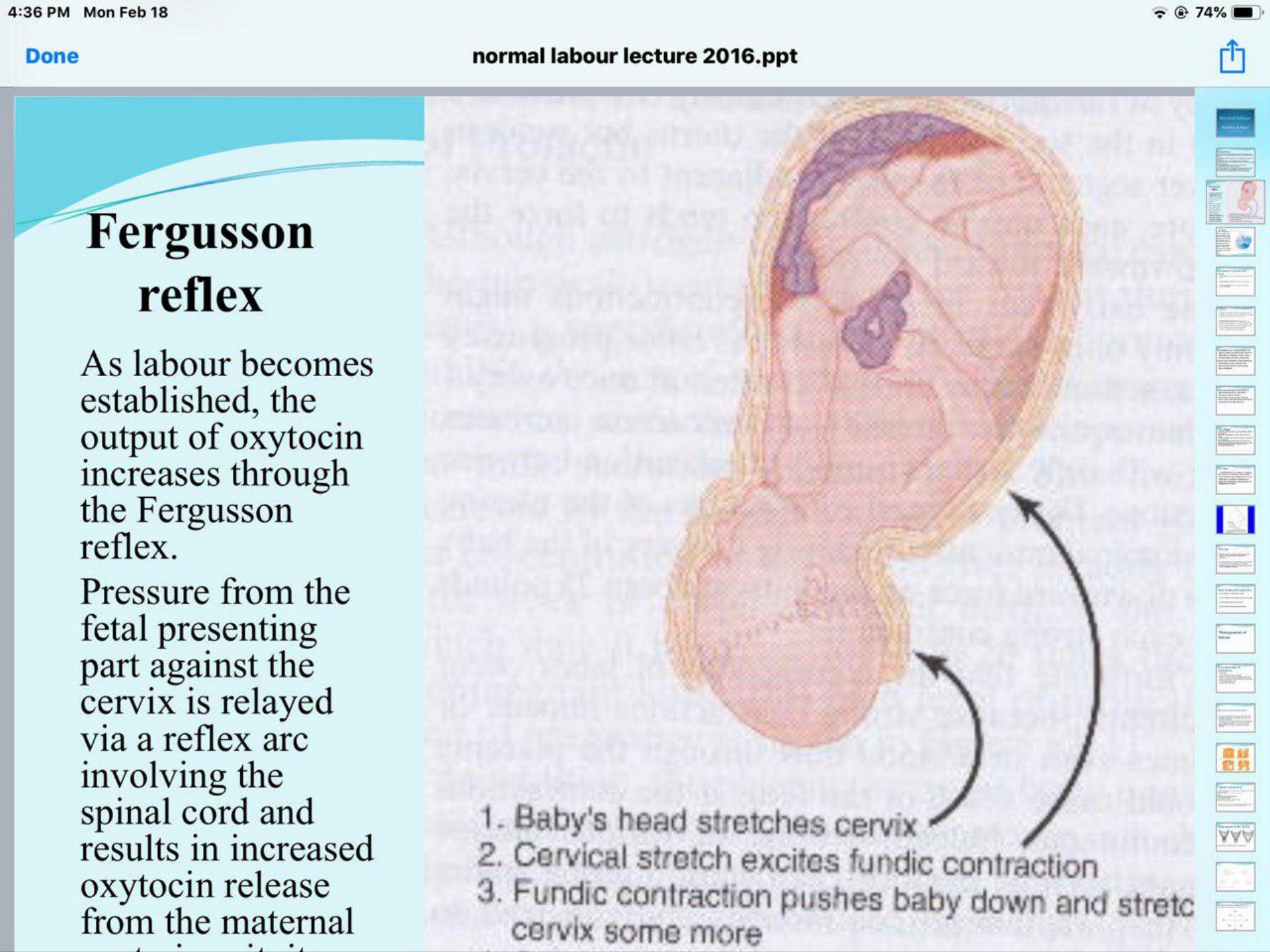
It is unclear which of these hormonal changes actually initiates labour. As labour becomes
established, the output of oxytocin increases through the ‘Fergusson reflex’. Pressure from the
fetal presenting part against the cervix is relayed via a reflex arc involving the spinal cord and
results in increased oxytocin release from the maternal posterior pituitary.
Diagnosis of labour
The onset of labour can be defined as the presence of strong regular painful contractions
resulting in progressive cervical change. Therefore, a diagnosis of labour strictly speaking
requires more than one vaginal examination after an interval and is made in retrospect. In
practice, the diagnosis is suspected when a woman presents with contraction-like pains, and is
confirmed when the midwife performs a vaginal examination that reveals effacement and
dilatation of the cervix. Loss of a ‘show’ (a blood-stained plug of mucus passed from the
cervix) or spontaneous rupture of the membranes (SROM) does not define the onset of labour,
although these events may occur around the same time. Labour can be well established before
either of these events occurs, and both may precede labour by many days. Although much is
understood about the physiology of labour in humans, the initiating process is still unclear. It is

certainly true, however, that the uterus and cervix undergo a number of changes in preparation
for labour, which start a number of weeks before its onset.
Stages of labour
Labour can be divided into three stages. The definitions of these stages rely predominantly on
anatomical criteria, and in real terms the moment of transition from first to second stage may
not be apparent. The important events when labour is normal are the diagnosis of labour and the
maternal urge to push, which usually corresponds with full dilatation of the cervix and the
baby’s head resting on the perineum. Defining the three stages of labour becomes more relevant
if labour is not progressing normally. The average duration of a first labour is 8 hours, and that
of a subsequent labour 5 hours. First labour rarely lasts more than 18 hours, and second and
subsequent labours not usually more than 12 hours.
First stage
This describes the time from the diagnosis of labour to full dilatation of the cervix (10 cm). The
first stage of labour can be divided into two phases. The ‘latent phase’ is the time between the
onset of regular painful contractions and 3–4 cm cervical dilatation. During this time, the cervix
becomes ‘fully effaced’.
Effacement is a process by which the cervix shortens in length as it becomes incorporated into
the lower segment of the uterus. The process of effacement may begin during the weeks
preceding the onset of labour, but will be complete by the end of the latent phase. Effacement
and dilatation should be thought of as consecutive events in the nulliparous woman, but they
may occur simultaneously in the multiparous woman. Dilatation is expressed in centimetres
from 0 to 10 cm.
The duration of the latent phase is variable, and time limits are arbitrary.
However, it usually lasts between 3 and 8 hours, being shorter in multiparous women.
The second phase of the first stage of labour is called the ‘active phase’ and describes the time
between the end of the latent phase (3–4 cm dilatation) and full cervical dilatation (10 cm). It is
also variable in length, usually lasting between 2 and 6 hours, shorter in multiparous women.

Cervical dilatation during the active phase occurs typically at 1 cm/hour or more in a normal
labour (again, an arbitrary value), but is only considered abnormal if it occurs at less than 1 cm
in 2 hours.
Second stage
This describes the time from full dilatation of the cervix to delivery of the fetus or fetuses. The
second stage of labour may also be subdivided into two phases. The ‘passive phase’ describes
the time between full dilatation and the onset of involuntary expulsive contractions. There is no
maternal urge to push and the fetal head is still relatively high in the pelvis. The second phase is
called the ‘active second stage’. There is a maternal urge to push because the fetal head is low
(often visible), causing a reflex need to ‘bear down’. In a normal labour, the second stage is
often diagnosed at this late point because the maternal urge to push prompts the midwife to
perform a vaginal examination. If a woman never reaches a point of involuntary pushing, the
active second stage is said to begin when she starts making voluntary pushing efforts directed
by her midwife. Conventionally, a normal active second stage should last no longer than 2
hours in a nulliparous woman and 1 hour in women who delivered vaginally before. Again,
these definitions are fairly arbitrary, but there is evidence that a second stage of labour lasting
more than 3 hours is associated with increased maternal and fetal morbidity. Use of epidural
anaesthesia will influence the length and management of the second stage of labour. A passive
second stage of 1 or 2 hours is usually recommended to allow the head to rotate and descend
prior to active pushing.
Third stage
This is the time from delivery of the fetus or fetuses until complete delivery of the placenta(e)
and membranes. The placenta is usually delivered within a few minutes of the birth of the baby.
A third stage lasting more than 30 minutes is defined as abnormal, unless the woman has opted
for ‘physiological management’ in which case it is reasonable to extend this definition to 60
minutes.

The duration of labour
There is no ideal length of labour for all women but morbidity increases when labour is too fast
(precipitous) or two slow (prolonged). From a psychological perspective, the morale of most
women starts to deteriorate after 6 hours in labour, and after 12 hours the rate of deterioration
accelerates. There is a greater incidence of fetal hypoxia and need for operative delivery
associated with longer labours. It is difficult to define prolonged labour, but it would be
reasonable to suggest that labour lasting longer than 12 hours in nulliparous women and 8 hours
in multiparous women should be regarded as prolonged. Precipitous labour is defined as
expulsion of the fetus within less than 3 hours of the onset of regular contractions.