Fifth Stage
Gynecology
Dr. Sumeya – Lecture 2
1
Subfertility / Male Infertility
Background, Definition:
Infertility = “failure to conceive following 1 year of unprotected intercourse if under 35
years of age or six months if over 35”.
•
10-15% couples affected
Etiology:
—
Couples:
○
16% Tubal and pelvic pathology
○
21 % Male problems
○
29% Ovulatory dysfunction
○
18% Unexplaine
○
7% Endometriosis,2%Cervical,3%Uterine,4%Multiple
For a woman with a normal menstrual cycle of 28 days, ovulation occurs around day 14.
The average survival time of the oocyte is around 24 hours, while after ejaculation
sperm may survive for up to 7 days in the female reproductive tract.
* Normal couple: 25-30% chance of pregnancy per ovulatory cycle
Primary -Couple has never conceived
Secondary -
couple has had at least one prior conception
Time of Exposure
% Pregnant
3 months
60%
6 months
70%
1 year
85%
18 months
90%
Causes
ž
Male
ž
Female
ž
Combined
ž
Unexplained
2
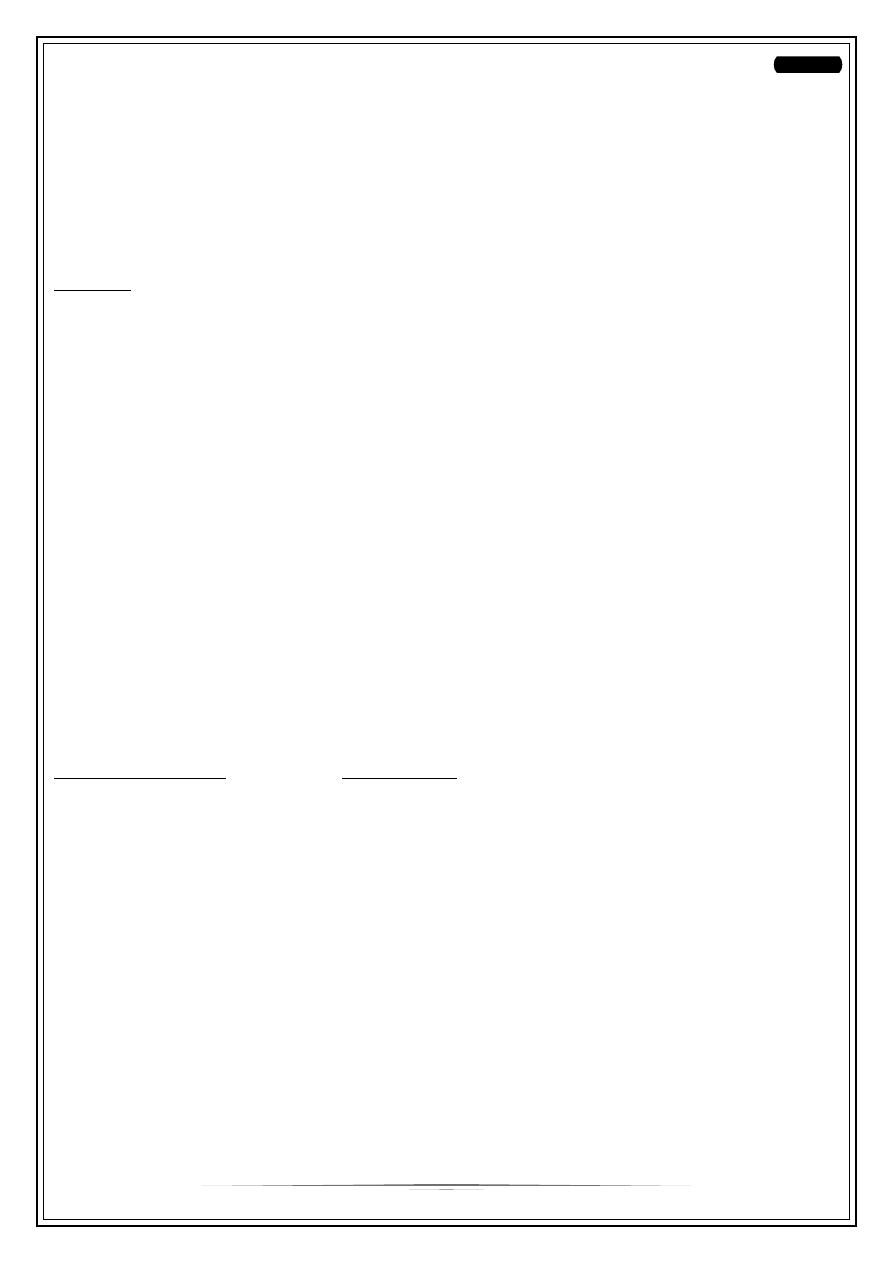
Male Infertility
Anatomy of the testis
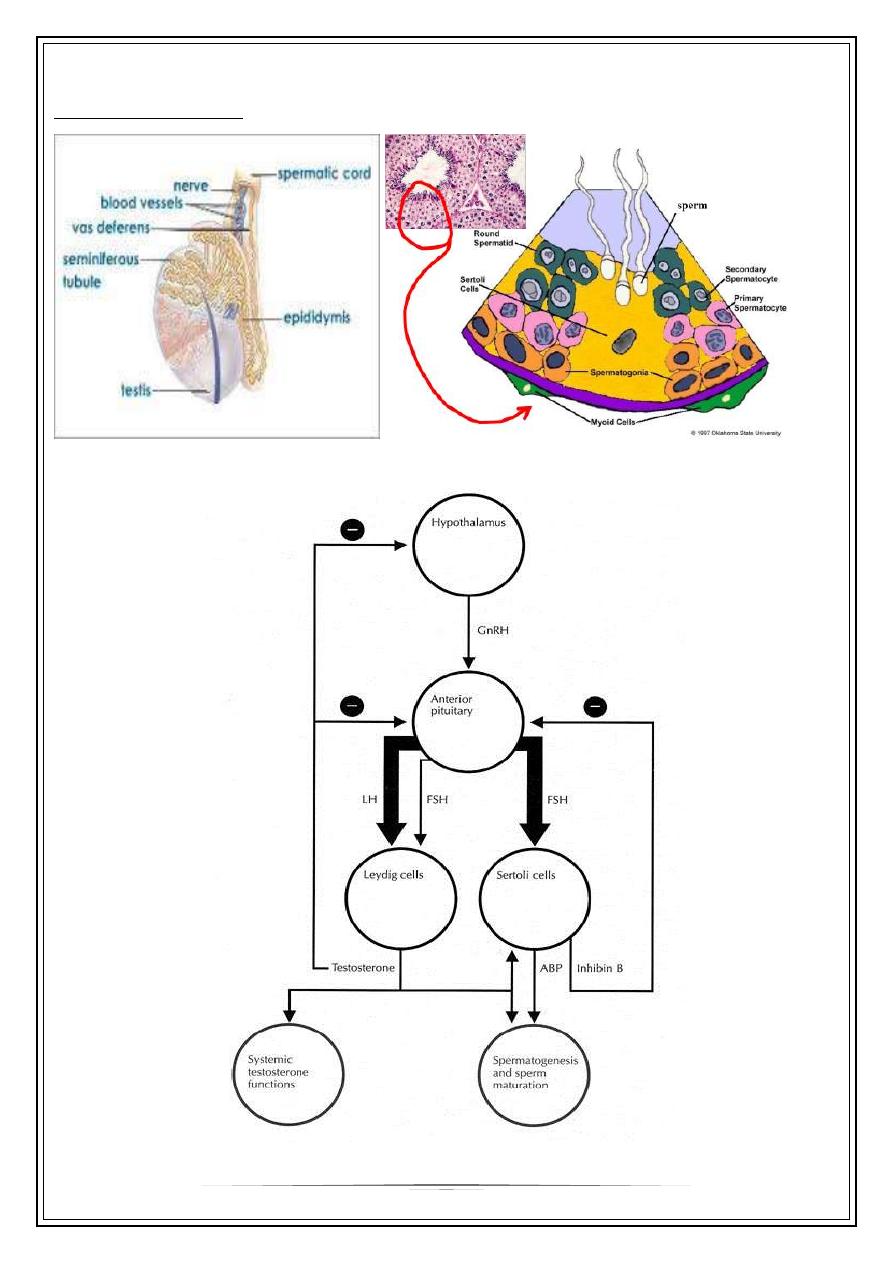
Hypothalamic-Pituitary-Gonadal Axis
3
—
Hypothalamus
○
Congenital abnormalities of hypothalamus
—
e.g. Kallman’s syndrome
○
Starvation, stress or severe illness
○
Tumors (craniopharyngioma, metastatic tumor)
○
Head injury
○
Inflammation (sarcoidosis)
○
Infection (tuberculosis)
○
XRT
○
Drugs: marijuana,
—
Pituitary
○
Endocrine: thyroid, prolactin
○
Tumors
○
Inflammation: sarcoidosis, meningitis
○
Infiltration
○
Infarction
○
Trauma/XRT
○
Drugs: anabolic steroids
—
Testis:
○
Congenital: Klinefelters (XXY), developmental disorders
○
Disorders of gonadal steroidgenesis
○
Infection: chlamydia, prostatitis, mumps orchitis
○
Autoimmune
○
Cryptorchidism
○
Tumors; chemo/XRT
○
Drugs / alcohol
○
Vascular: testicular torsion
4
—
Temperature
○
Rise in scrotal temperature
○
Occupation
○
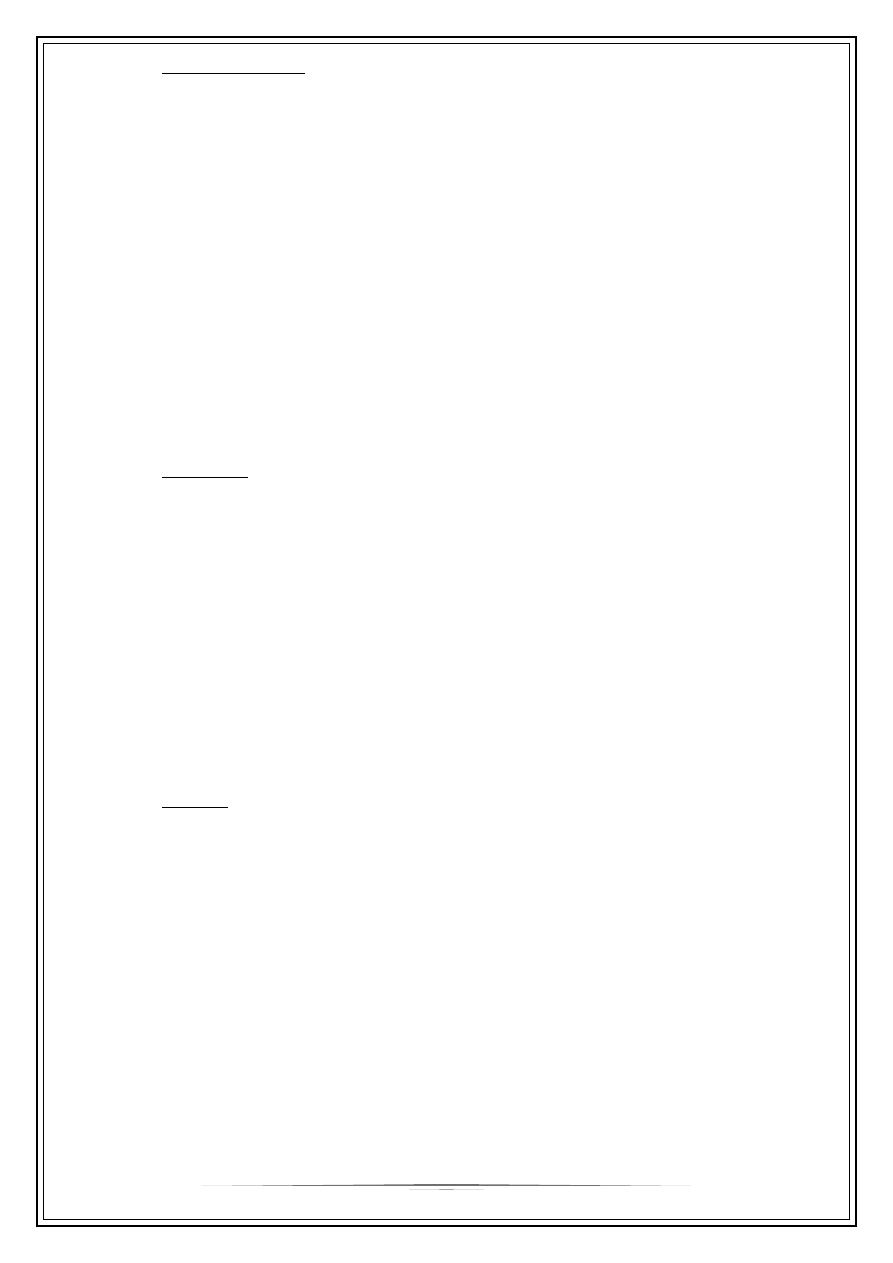
Varicocoele
Post testicular causes:
Impotence/Ejaculation
A-Neurogenic: medications (α-blockers, methyldopa)
B-Endocrine: diabetes
○
Congenital: absence vas deferens (CF)
○
Genetic: cystic fibrosis
○
Primary ciliary dyskinesia:
Kartagener syndrome
○
Hypospadia
○
Vasectomy
Investigations:
—
semen analysis
○
Abstain 2-7 days prior
○
At least 2 samples over different period of time
—
If abnormal:
○
Blood work: FSH, LH, TSH, testosterone, PRL
○
Testicular U/S
○
Chromosomal analysis
Semen
also known as seminal fluid, is an organic
fluid that may contain spermatozoa. It is secreted
by the gonads ( testis and accessory sex glans).
Seminal fluid contains several components besides
spermatozoa: proteolytic and other enzymes as well
as fructose are elements of seminal fluid which
promote the survival of spermatozoa, and provide a
medium through which they can move or "swim".
5
Macroscopical characteristics:
Liquefaction time:
Liquefaction time is a natural change in the consistency of semen from a semi liquid
to a liquid. Immediate coagulation is due to a clot formation from seminal vesicles
material, followed by gradual liquefaction over the next 5-20 minutes due to enzymatic
process involving the prostatic secretion.
In evaluation of liquefaction, ejaculate is
placed in an incubator at 37°C and allowed to be liquefied. Liquefaction time more than
60 minutes or no liquefaction longer is pathologic showing lack of prostatic enzyme or
inadequate prostate function .
Semen viscosity:
Normal semen has a viscous texture. Increase in viscosity may occur due to
hypofunction of seminal vesicles. High viscosity may affect sperm motility and
concentration. Increase in viscosity may reduce the success of intrauterine insemination
(IUI) and in vitro fertilization (IVF) .
Appearance of the ejaculate:
A normal ejaculate has a homogenous grey-opalescent appearance.A whitish colour may
indicate high sperm numbers or presence of leukocytes a yellowish appearance and
purulent smell indicate infections. A reddish-brown colour indicates the presence of red
blood cells (hemospermia) .
Semen volume:
The lower reference limit for semen volume is 1.5 ml (WHO 2010). A small volume may
also be due to loss of part of the specimen, retrograde ejaculation, abnormality or
infection of accessory sex glands, or ejaculatory duct obstruction. An extremely high
volume may indicate inflammation or urine contamination and is associated with lower
conception rates .
Semen pH:
The pH of semen reflects the balance between the pH values of the different accessory
gland secretions, mainly the alkaline seminal vesicular secretion and the acidic prostatic
secretion. A lower threshold value is 7.2
Microscopic characteristics
Agglutination
Agglutination of spermatozoa means that motile spermatozoa stick to each other,
head to head, midpiece to midpiece, tail to tail, or mixed, e.g. midpiece to tail. The
adherence of either immotile or motile spermatozoa to mucus threads, to cells
other than spermatozoa, or to debris is not considered agglutination and should
not be recorded as such. The presence of agglutination is suggestive of, but not
sufficient evidence to prove the existence of an immunological factor of fertility.
6
When agglutination is observed, semen cultures and antibody assessment should
be performed .
The major types of agglutination (WHO 2010):
•
grade 1: isolated <10 spermatozoa per agglutinate, many free spermatozoa.
•
grade 2: moderate 10–50 spermatozoa per agglutinate, free spermatozoa.
•
grade 3: large agglutinates of >50 spermatozoa, some spermatozoa still free.
•
grade 4: gross all spermatozoa agglutinated and agglutinates interconnected.
Sperm count and concentration
According to WHO2010, the lower reference limit for sperm concentration is 15 × 10
6
spermatozoa per ml and the lower reference limit for total sperm number is 39 × 10
6
spermatozoa per ejaculate. A sperm concentration of less than this value is regarded as
abnormal .
Sperm motility
The percentage of motile spermatozoa and their progressiveness usually give a good
indication on sperm quality and are important in predicting men fertility . Several
studies have demonstrated the correlation of motility with the fertilization rate in vivo
and in vitro .
▪
Categories of sperm movement (WHO 2010):
A simple system for grading motility is recommended that distinguishes spermatozoa
with progressive or non-progressive motility from those that are immotile. The motility
of each spermatozoon is graded as follows:
•
Progressive motility (PR): spermatozoa moving actively, either linearly or in a
large circle, regardless of speed.
•
Non-progressive motility (NP): all other patterns of motility with an absence of
progression, e.g. swimming in small circles, the flagellar force hardly displacing
the head, or when only a flagellar beat can be observed.
•
Immotility (IM): no movement ().
Lower reference limit (WHO 2010):
•
The lower reference limit for total motility (PR + NP) is 40%.
•
The lower reference limit for progressive motility (PR) is 32%.
7
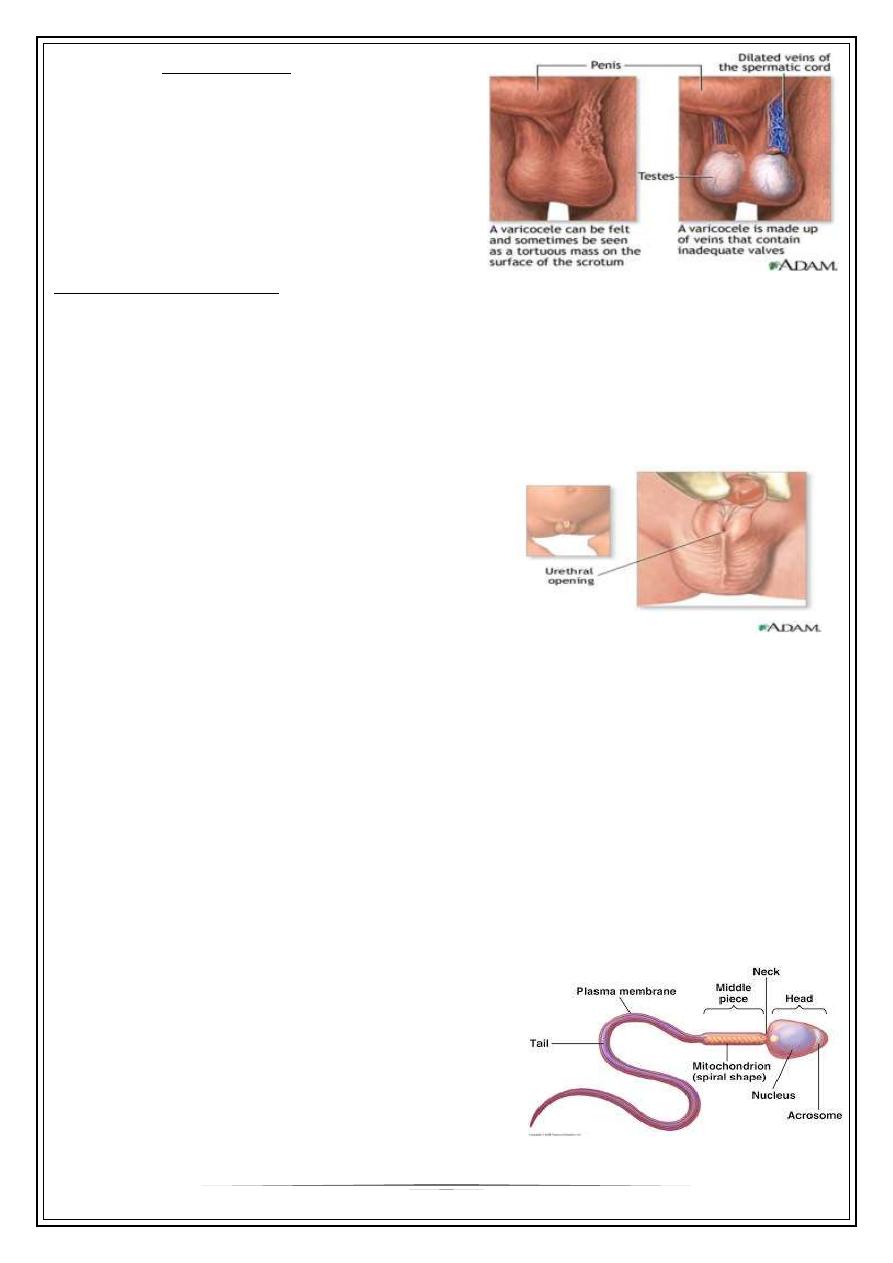
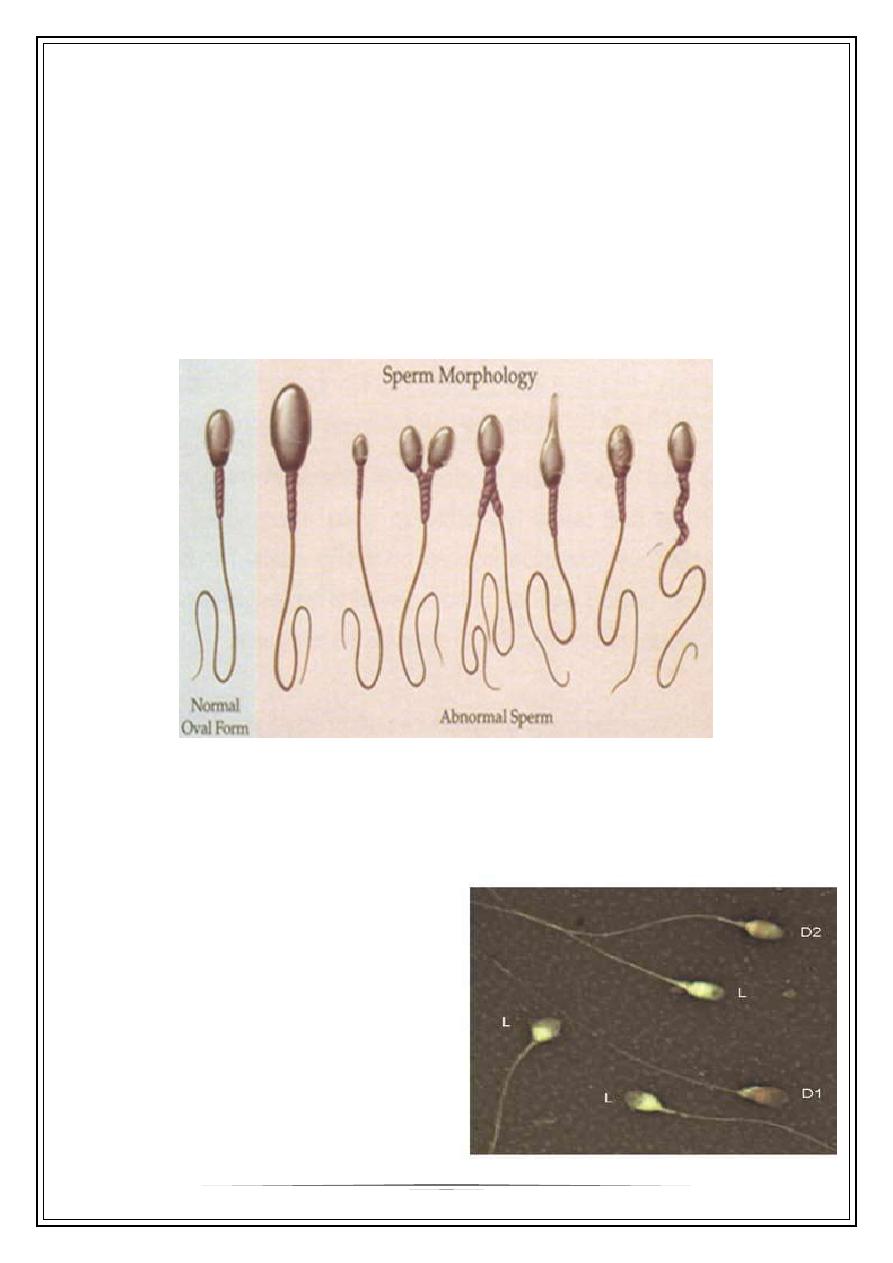
Sperm morphology
Many authors have gone as far as to argue that sperm morphology is a reflection of
sperm functional competence and Sperm morphology assessment has been considered
a valuable and stable method for predicting the in vivo and in vitro sperm fertilizing
ability .
Abnormalities of spermatozoa can be classified into head abnormality, neck/midpiece
abnormality, tail abnormality, or the presence of cytoplasmic residue. These
abnormalities can occur as a single defect or in a combination of two, three or all four
abnormalities simultaneously. The reference value for normal sperm morphology
determined by Kruger is >14% WHO1999 vs. 2010 the WHO reference values for normal
sperm morphology is >4% .
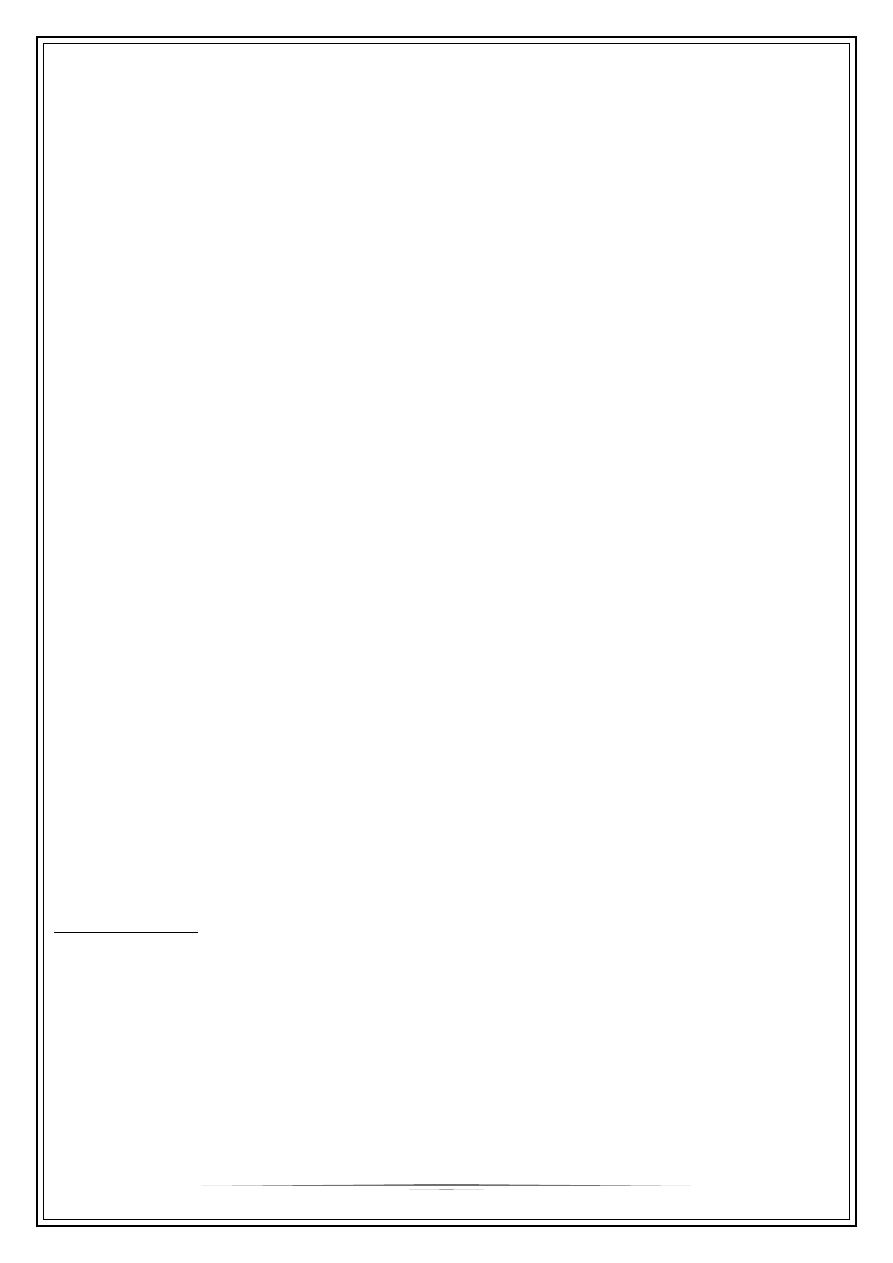
Sperm vitality
It is especially important for samples with less than about 40% progressively motile
spermatozoa. The lower reference limit for vitality (membrane-intact spermatozoa) is 58
%( WHO 2010).
Nowadays, there are several standard tests
available for the assessment of the vitality
of spermatozoa . One of these tests is based
on the principle that dead spermatozoa take
up the supravital red stain of eosin-Y,
whereas living cells, regardless of their
motility stage, will be unstained This assay
reflects sperm membrane integrity,
particularly the head region which takes up
the red stain immediately
8
Round cell count (cells other than spermatozoa)
The existence of round cells in human ejaculates is common. These can be immature
germ cells or somatic cells including epithelial cells of the post-testicular tract and
leucocytes . Epithelial cells are indicative of poor collection when present in high
numbers . Leukocytes are the most significant non sperm cellular elements in the semen
and are a frequent finding in patients who have unexplained infertility. A threshold for
classification of leukocytospermia as high as 1×10
6
/ml .The semen sample with <5
round cells/ HPF was considered normal .
Endocrine Tests
The endocrine assessment of an infertile man includes measurements of serum
testosterone, luteinizing hormone (LH), and follicle-stimulating hormone (FSH), and
perhaps other tests:
Serum Testosterone
Measurement of a morning serum total testosterone is usually sufficient. In men
with borderline values, the measurement should be repeated and measurement of
serum-free testosterone may be helpful.
Serum Luteinizing Hormone and Follicle-Stimulating Hormone
When the serum testosterone concentration is low, high serum FSH and LH
concentrations indicate primary hypogonadism and values that are low or normal
indicate secondary hypogonadism.
Other Hormones
Serum prolactin should be measured in any man with a low serum testosterone
concentration and normal to low serum LH concentration. Although inhibin assays
are not widely available outside of research laboratories, low serum inhibin
concentrations may be an even more sensitive test of primary testicular
dysfunction than high serum FSH concentrations, provided the assay is specific for
inhibin B.
TERMINOLOGY
Oligozoospermia; sperm conc. less than 15 × 10
6
spermatozoa per ml
Teratozoospermia; normal sperm morphology is <4% kruger strict criteria
•
Asthenozoospermia; total motility (PR + NP) < 40% or progressive motility (PR) <
32%.
Azoospermia; no sperm in ejaculate
Aspermia; no semen
9
Tx / Interventions:
—
Treat underlying causes
—
Intrauterine Insemination (IUI)
—
Intracytoplasmic Sperm Injection (ICSI)
Treatment of male infertility involves the couple.
Specific endocrine treatment is available for men whose infertility results from
hypogonadotropic hypogonadism. Hypogonadotropic hypogonadism due to
hyperprolactinemia can often be corrected and fertility restored by lowering the
serum prolactin concentration. If the hyperprolactinemia results from a
medication, as is often the case, that medication should be discontinued, if
possible. The hyperprolactinemia is caused by a lactotroph adenoma. It should be
treated with a dopamine agonist, such as cabergoline or bromocriptine. The
process of spermatogenesis normally takes 3 months. As a result, restoration of a
normal sperm count usually does not occur for at least 3 and sometimes 6 months
or more after the serum prolactin and testosterone concentrations have returned
to normal.
In some patients, who have a lactotroph macroadenoma, the hypogonadotropic
hypogonadism appears to be the result of permanent damage to the gonadotroph
cells by the mass effect of the adenoma. Gonadotropin treatment should be
instituted for these patients.
Gonadotropin therapy: Treatment is initiated with human chorionic gonadotropin
(hCG), 1,500–2,000 IU three times per week subcutaneously or intramuscularly for
at least 6 months. hCG has the biologic activity of LH. The hCG dose should be
adjusted upward according to symptoms of hypogonadism, serum testosterone
concentrations, and semen parameters.
Some patients with acquired hypogonadotropic states can be stimulated with hCG
alone to produce sufficient sperm. If after 6–9 months the patient remains
azoospermic or severely oligospermic, then human menopausal gonadotropin
(hMG) or recombinant FSH should be added.
• Pulsatile GnRH treatment: Pulsatile subcutaneous or intravenous treatment with
GnRH has also been successfully used to treat gonadotropin deficient patients.
GnRH has to be delivered in pulses using a portable pump with an attached
catheter and needle for many months or years; most patients find it inconvenient
to use GnRH therapy for so long.
10
Genital infection
Infertile men rarely present with symptoms or signs of acute genital infections or
prostatitis, but they are sometimes diagnosed as having infections of the
urogenital tract by the presence of increased leukocytes in the semen. Despite the
absence of symptoms, we typically treat patients who have leukospermia, even if
the culture is negative, with at least a 10-day course of antibiotics such as
erythromycin or trimethoprim-sulfamethoxazole. A second course of therapy is
usually given if leukocytes persist in the semen after antibiotics.
Sperm Autoimmunity
Continuous or intermittent high doses of prednisone (from 40 mg/ day to 80
mg/day) for up to 6 months have been shown in placebo-controlled trials to
improve cumulative pregnancy significantly in partners of men with sperm
autoantibodies.
However, many patients cannot tolerate this regimen because of the adverse
effects of high-dose corticosteroid therapy. As a result, most couples prefer to try
an assisted reproductive technique, such as ICSI, as primary treatment for sperm
autoimmunity.
Empirical Therapy
Many treatments have been used empirically for male infertility, including
clomiphene citrate and other hormones and vitamins.
Aromatase inhibitors may improve sperm concentrations in men with severe
oligozoospermia or azoospermia prior to sperm retrieval for ICSI.
To be continued,,,