Fifth Stage
Gynecology
Dr. Sumeya – Lecture 3
1
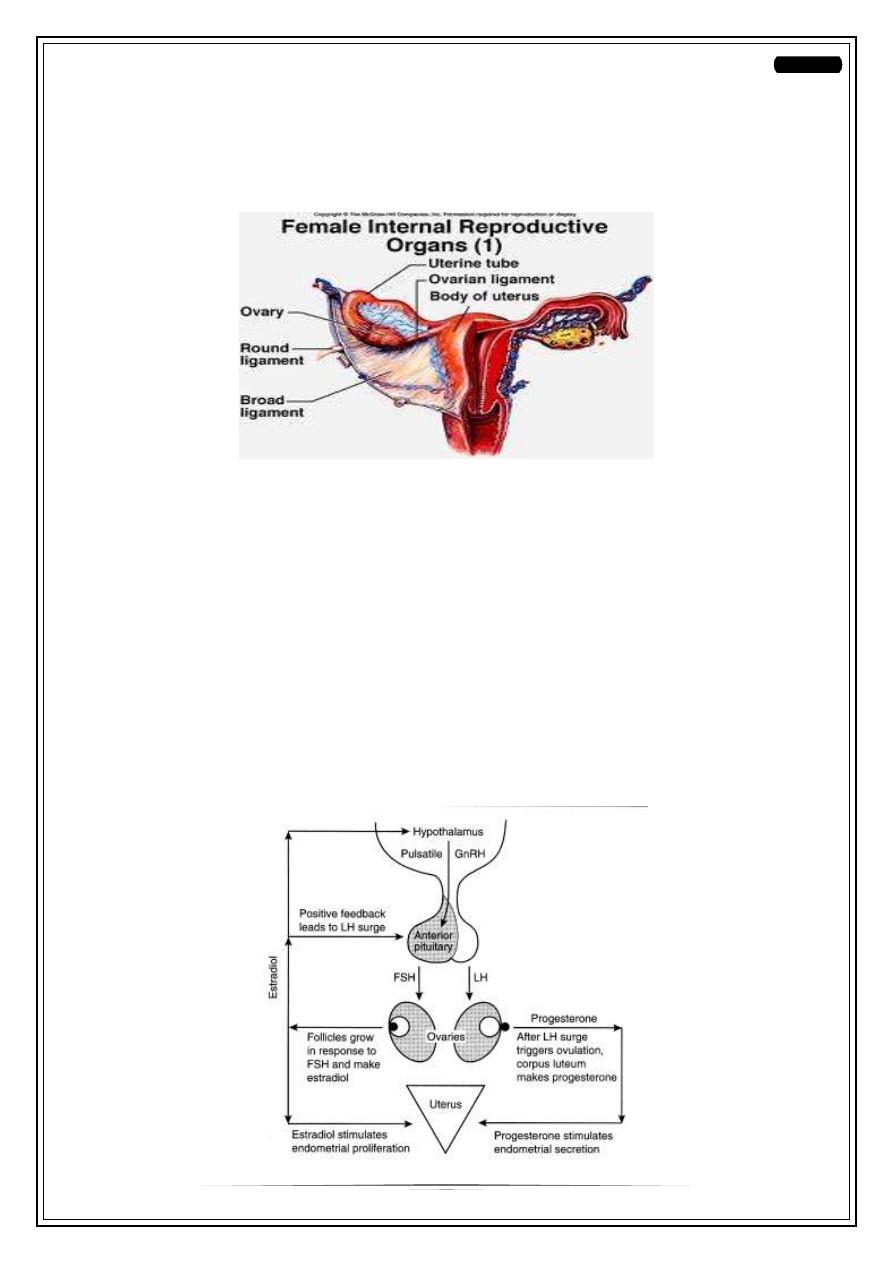
Female Infertility
Fecundability: probability of achieving a pregnancy within 1 menstrual cycle (25%)
Fecundity: ability to achieve a live birth within 1 menstrual cycle (6%)
Causes
—
Hypothalamus
—
Pituitary
—
Ovary
—
Uterus
—
Vagina
—
Fallopian tube
—
Cervix
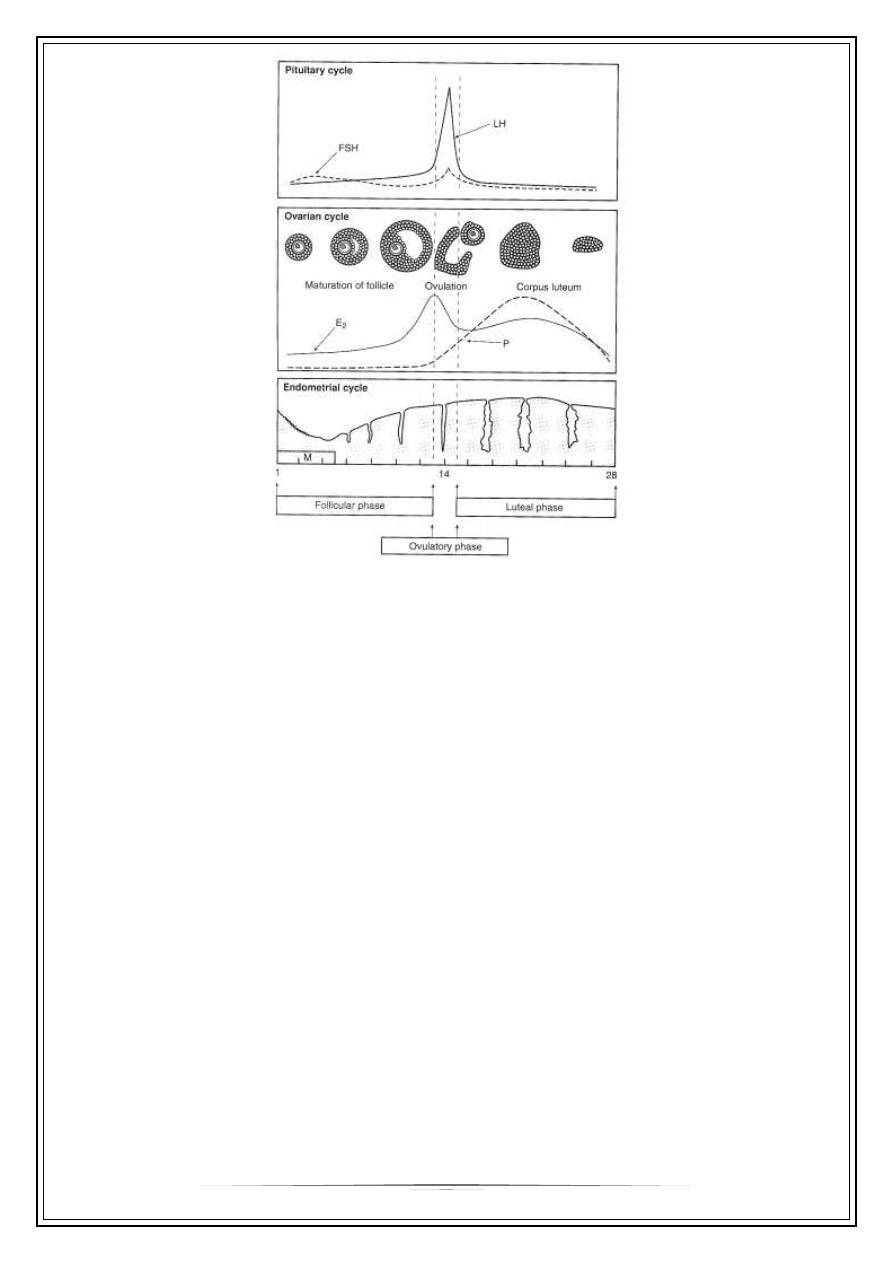
Hypothalamic-Pituitary-Gonadal Axis:
2
Pituitary:
—
Sheehan syndrome
—
Tumors: Pituitary adenoma, metastatic
—
Empty sella syndrome
—
Inappropriate gonadal steroid feedback:
○
estrogen excess: obesity/ tumors
○
estrogen deficiency: aromatase deficiency/ ER gene mutation
○
androgen excess: adrenal or ovarian
—
Hyperprolactinaemia
—
Thyroid dysfunction
Hypothalamus:
—
Stress
—
Exercise
—
Eating disorders
—
Psychogenic
3
—
Starvation/stress or severe illness
—
Tumors (craniopharyngioma, metastatic tumor)
—
Head injury
—
Inflammation (sarcoidosis)
—
Infection (tuberculosis)
—
XRT
—
Drugs
Ovary:
—
Gonadal dysgenesis - Turner’s Syndrome 45XO
—
XRT / Chemo for childhood malignancies
○
Premature ovarian failure
○
PCOS
Uterine abnormalities:
—
Mullerian Agenesis: Mayer-Rokitansky-Kuster-Hauser syndrome
—
Asherman’s syndrome
—
Leiomyoma
—
Luteal phase deficiency
—
Vaginal septum
—
Tubal Disease
○
Infections/ STD/PID
○
Ruptured appendix
○
Septic abortion
—
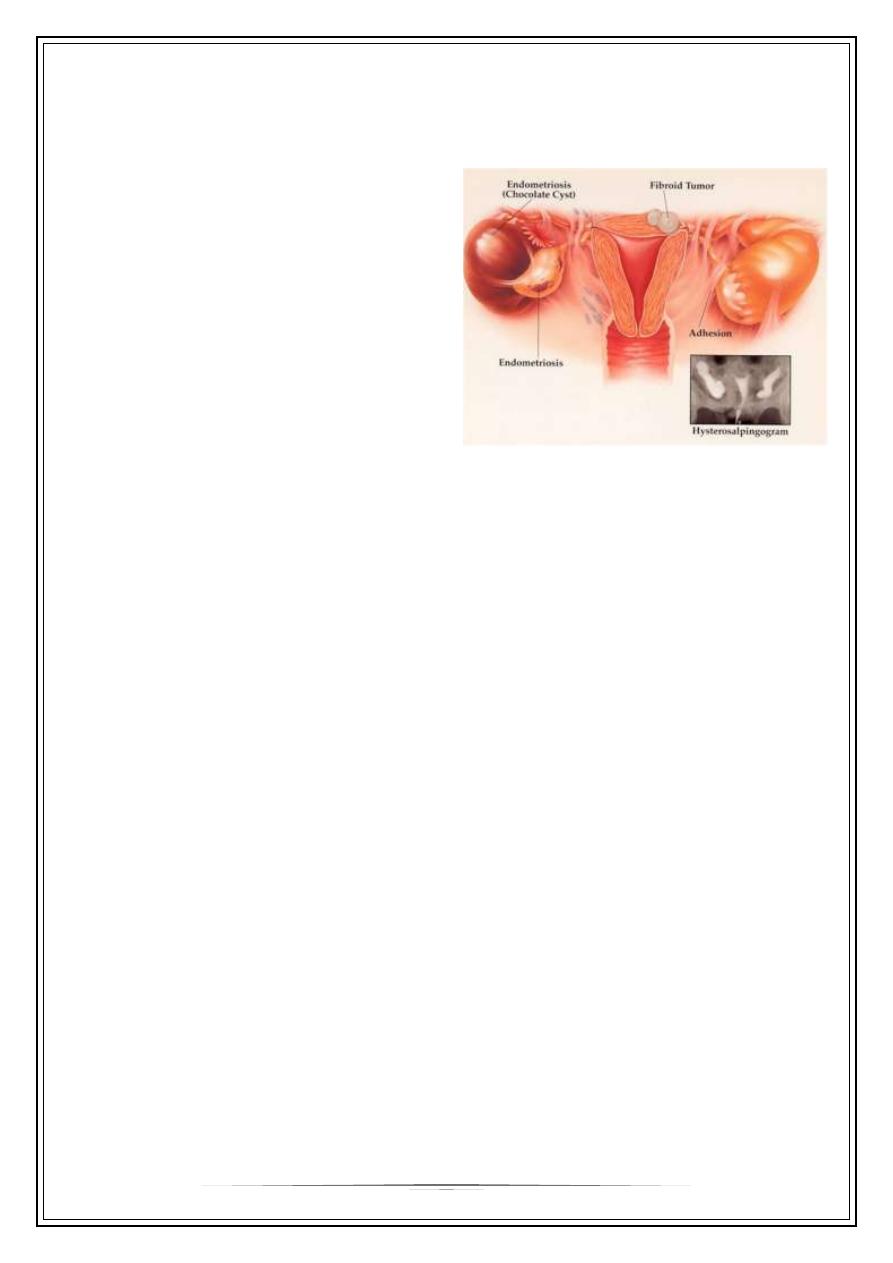
Endometriosis
—
Cervical
4
Investigations
ž
Blood work:
—
TSH
—
PRL
—
D3 FSH
—
D3 LH
—
Luteal phase Progesterone
ž
Imaging:
—
Pelvic Ultrasound
—
HSG
ž
Diagnostic
—
Laparoscopy (later)
—
Cervical(post coital test)
Marker of ovarian reserve
In the ovary, anti-Müllerian hormone (AMH) is produced by the granulosa cells.
AMH levels can be measured in blood and are shown to be proportional to the number of
small antral follicles. In women, serum AMH levels decrease with age and are
undetectable in the post-menopausal period. AMH levels represent the quantity of the
ovarian follicle pool and are a useful marker of ovarian reserve. AMH measurement can
also be useful in the prediction of the extremes of ovarian response to gonadotrophin
stimulation for in vitro fertilization, namely poor and hyper-response.
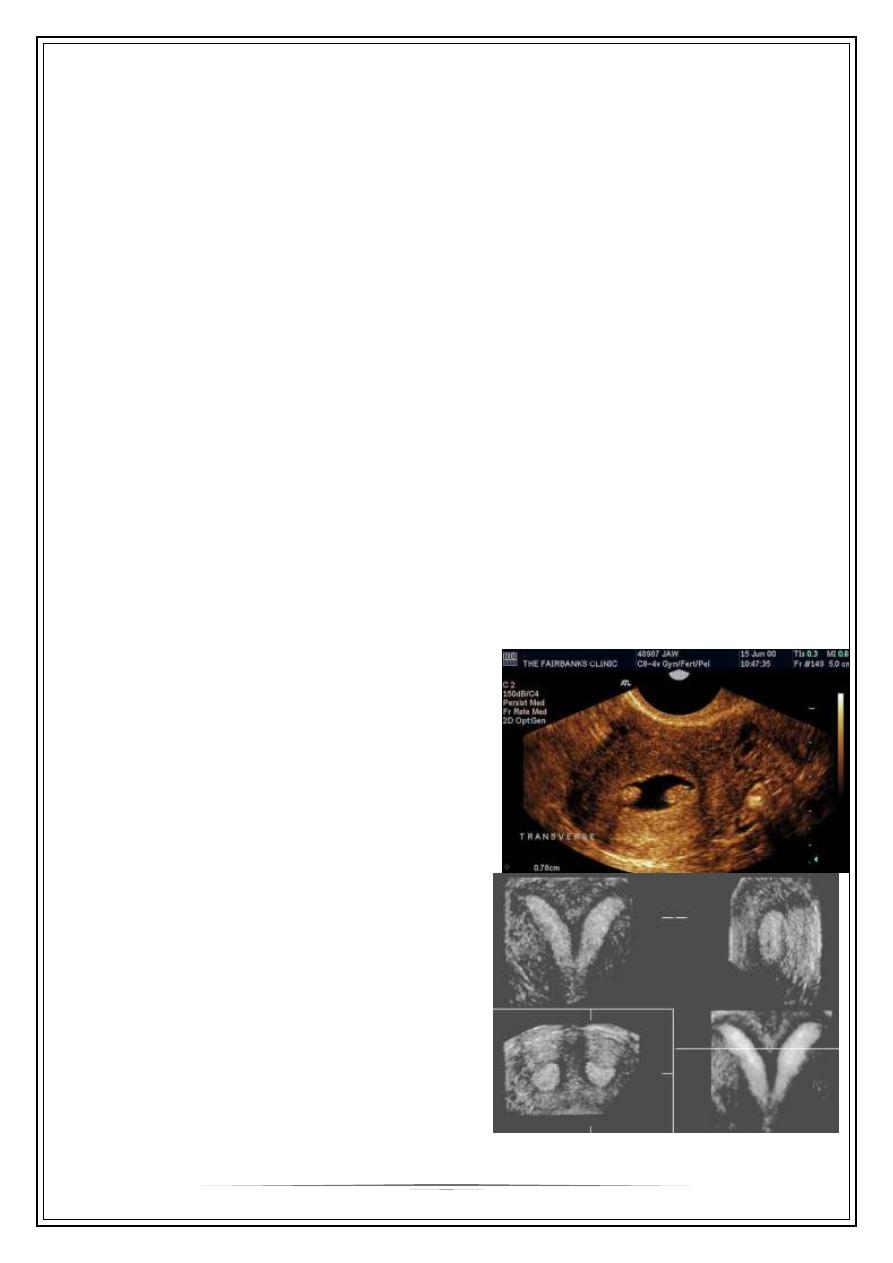
Ovulation testing
Various methods of predicting fertility exist, to either aid or avoid pregnancy.
Stretch test
Cervical mucus becomes clear and stretchy during the fertile window, to allow sperm to
survive in and travel through it.
Ovulation Prediction Kit
Ovulation prediction kits are usually antibody tests for luteinising hormone, which peaks
in urine around the time of ovulation.
Cervical position
The cervix becomes soft, high, open and wet during the fertile window.
5
Basal body temperature
Basal body temperature changes during the menstural cycle. Progesterone released
during the menstrual cycle causes an abrupt increase in basal body temperature by
0.5°C at the time of ovulation.This enables identification of the fertile window through
the use of commercial thermometers.
Progesterone level
Measurement of progesterone in the second half of the cycle to help confirm ovulation
Treatment
ž
Treat the underlying cause
ž
Medical
ž
Surgical
Medical treatments
Drugs
•
Clomiphene
•
Human menopausal gonadotropin, hMG
•
FSH
•
Human chorionic gonadotropin, hCG
•
Gonadotropin – releasing hormone (Gn-RH) analogs
•
Aromatase inhibitors
•
Metformin
•
Bromocriptine
Gonadotropin-releasing hormone
ž
Either Gonadotropin-releasing hormone (GnRH) or
ž
any Gonadotropin-releasing hormone agonist (i.e. Lupron) may be used.
ž
GnRH stimulates the release of gonadotropins (LH and FSH) from the anterior
pituitary in the body.
Clomiphene
ž
is a selective estrogen receptor modulator (SERM). It is the most widely used
fertility drug. It is used as an ovarian stimulator by inhibiting the negative
feedback of estrogen at the hypothalamus. As the negative feedback of estrogen
6
is inhibited, the hypothalamus secretes GnRh which in turn stimulates the anterior
pituitary to secrete LH and FSH which help in ovulation.
Aromatase inhibitors
Although primarily a breast cancer treatment, aromatase inhibitors can also work as
fertility medication, probably through a mechanism similar to clomiphene.
Gonadotropins
Gonadotropins are the hormones in the body that normally stimulate
the gonads (testes and ovaries). For medication, they can be extracted from urine or by
genetic modification.
For example, the so-called menotropins consist of LH and FSH extracted from
human urine from menopausal women. FSH and FSH analogues are mainly used
for ovarian hyperstimulation as well as reversal of anovulation.
There are also recombinant variants which are created by inserting the DNA coding for it
into bacteriae. The bacterial DNA is then called Recombinant DNA. Examples of
recombinant FSH are Follistim and Gonal F, while Luveris is a recombinant LH.
Human chorionic gonadotropin
ž
Human chorionic gonadotropin (hCG) is normally produced during pregnancy.
However, it can also replace LH as an ovulation inducer.
Others
ž
dopamine agonist, such as cabergoline or bromocriptine. For treatment of
hyperprolactinaemia
ž
Metformine in PCOS
COMPLICATIONS
Fertility drugs have the risk of multiple pregnancies
•
Injectable fertility drugs increase the chance of multiple births
•
Careful monitoring: blood tests, hormone tests, ultrasound measurement of
ovarian follicle size
Because of risk of ovarian hyperstimulation syndrome
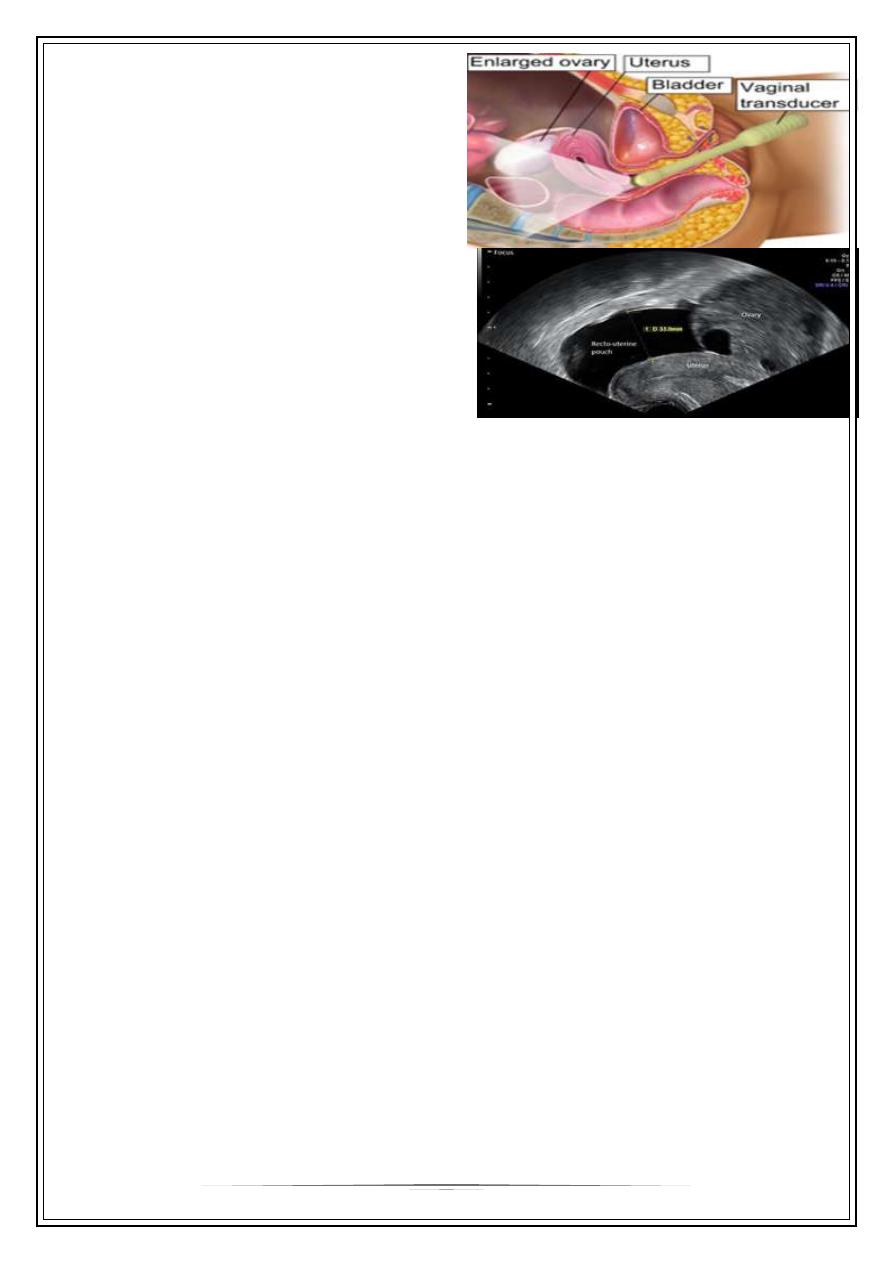
Ovarian hyperstimulation syndrome (OHSS)
is a medical condition affecting the ovaries of some women who take fertility
medication to stimulate egg growth. Most cases are mild, but rarely the condition
is severe and can lead to serious illness or death.
7
OHSS is divided into the categories
mild, moderate, severe, and critical. In
mild forms of OHSS the ovaries are
enlarged (5–12 cm) and there may be
additional accumulation of ascites with
mild abdominal distension, abdominal
pain, nausea, and diarrhea. In severe
forms of OHSS there may
be hemoconcentration, thrombosis and
distension, oliguria (decreased urine
production), pleural effusion,
and respiratory distress. Early OHSS
develops before pregnancy testing and
late OHSS is seen in early pregnancy.
Surgical treatment
ž
Hysteroscopy - A hysteroscopy is an outpatient procedure in which a narrow
fiberoptic telescope inserted into uterus through the cervix, to look for and
sometimes remove adhesions inside uterus.
ž
Laparoscopy -
A laparoscopy is surgical procedure in which a narrow fiberoptic telescope
inserted through an incision near navel to look for and sometimes remove
adhesions in pelvic cavity, remove ovarian cysts or remove or repair a fluid-filled
hydrosalpinx or ovarian drilling
ž
Fallopian Tube Sterilization Reversal (reanastomosis) - A tubal reversal is a
surgical procedure performed to reconnect the two ends of the fallopian tubes in
an effort to reverse sterilization.
ž
Hydrosalpinx removal - A hydrosalpinx is an obstructed fallopian tube that leads to
an accumulation of fluid. Removal of the affected tube can increase IVF success
rates.
Combined infertility
ž
In some cases, both the man and woman may be infertile or sub-fertile, and the
couple's infertility arises from the combination of these conditions.
ž
In other cases, the cause is suspected to be immunological or genetic; it may be
that each partner is independently fertile but the couple cannot conceive together
without assistance.
8
Unexplained infertility
ž
up to 20% of infertile couples have unexplained infertility. In these cases
abnormalities are likely to be present but not detected by current methods.
Possible problems could be that the egg is not released at the optimum time for
fertilization, that it may not enter the fallopian tube, sperm may not be able to
reach the egg, fertilization may fail to occur, transport of the zygote may be
disturbed, or implantation fails. It is increasingly recognized that egg quality is of
critical importance and women of advanced maternal age have eggs of reduced
capacity for normal and successful fertilization.
Thank You,,,
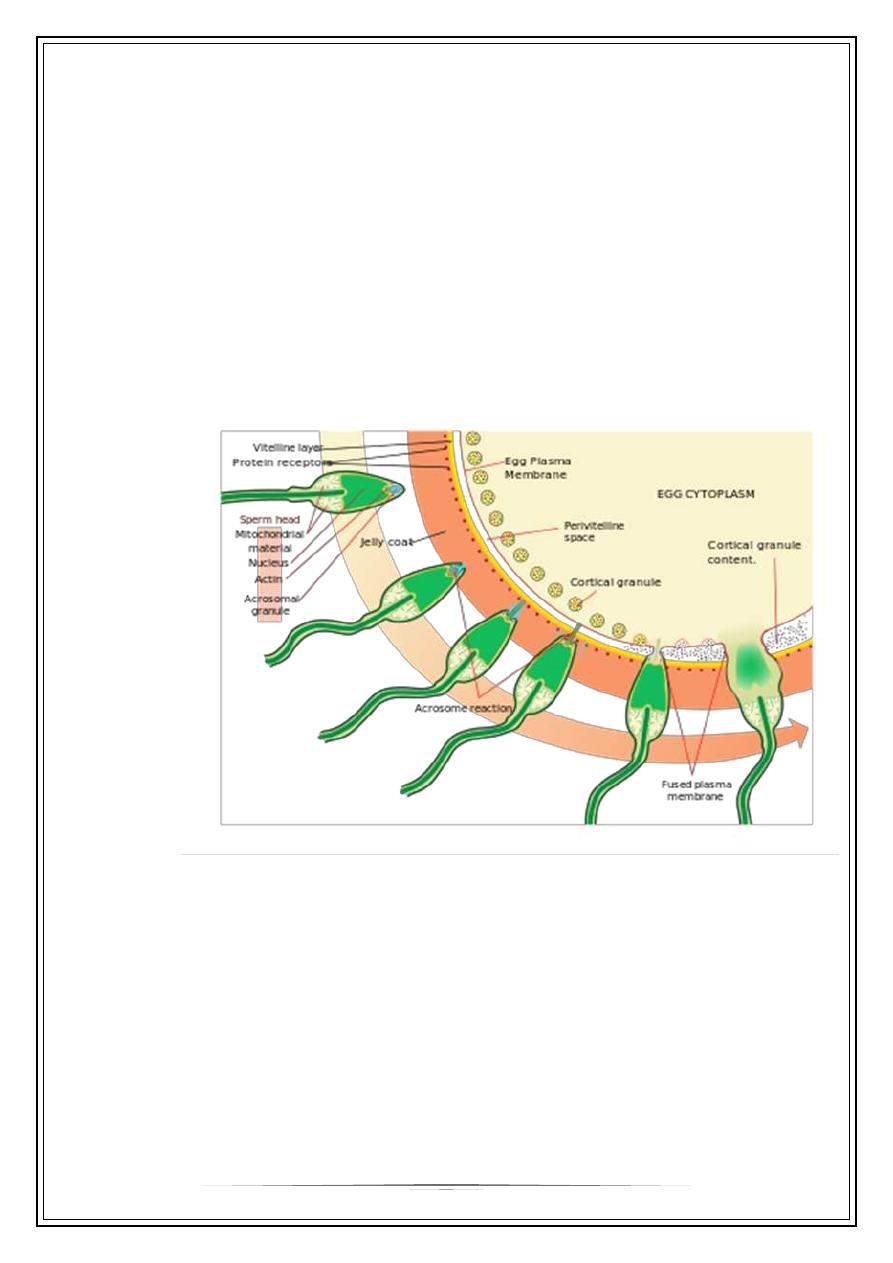
Fertilization