1
L1
CNS Infection
D. Hazim
CNS infection classified into:
Meningitis
Encephalitis
Brain abscess
Transverse myelitis
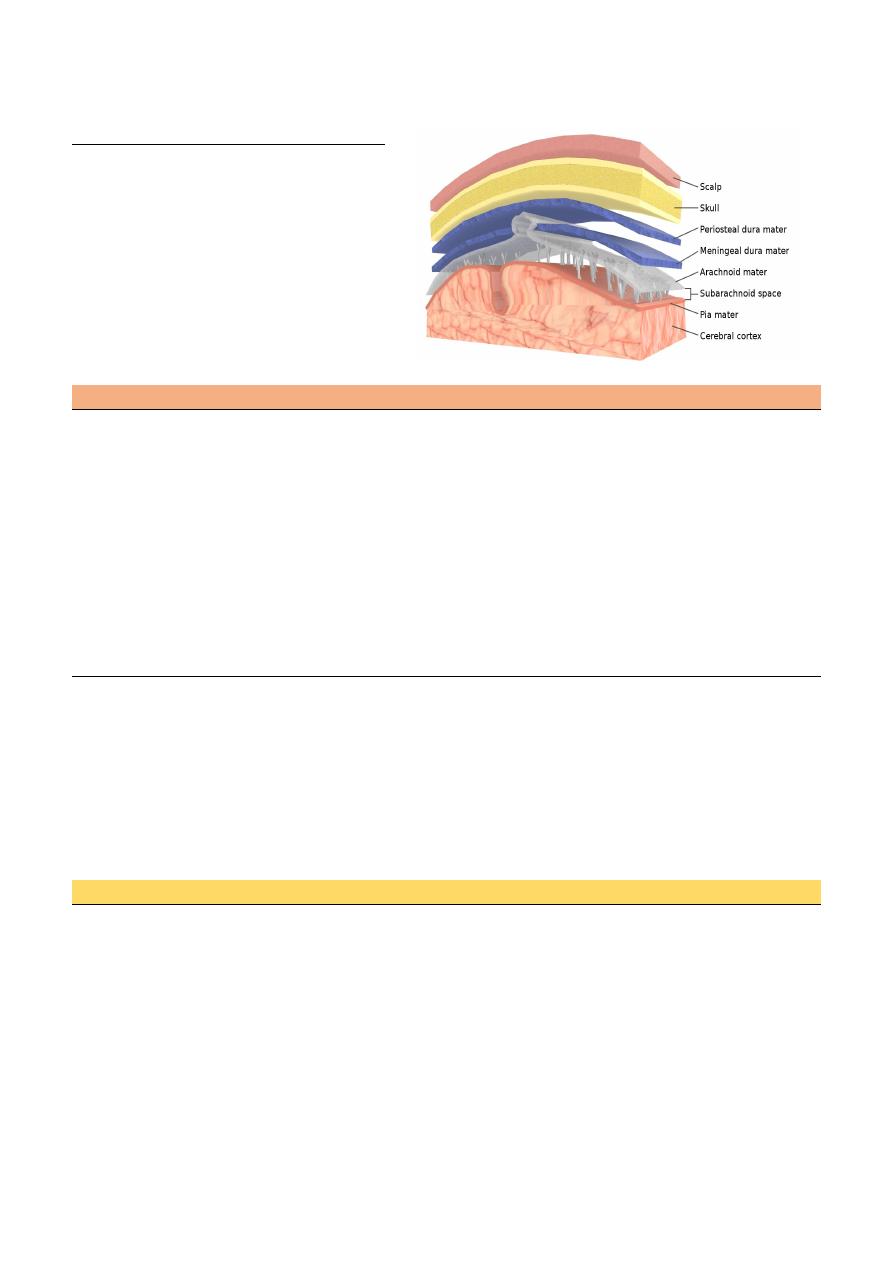
Meningitis
Acute infection of the meninges presents with a characteristic combination of
Pyrexia.
Headache.
Meningism.
Meningism, which can occur in other situations (e.g. subarachnoid hemorrhage), consists of:
Stiffness of the neck, often with other signs of meningeal irritation:
Kernig's sign (with the hip joint flexed, extension at the knee causes spasm in the hamstring
muscles).
Brudzinski's sign (passive flexion of the neck causes flexion of the thighs and knees).
Meningitis could be:
Viral
Bacterial (TB, pyogenic).
fungal
Carcinomatous
Acute 1-3 days
Subacute 3d – 3 wk.
Chronic more than 3 wk.
Bacterial meningitis
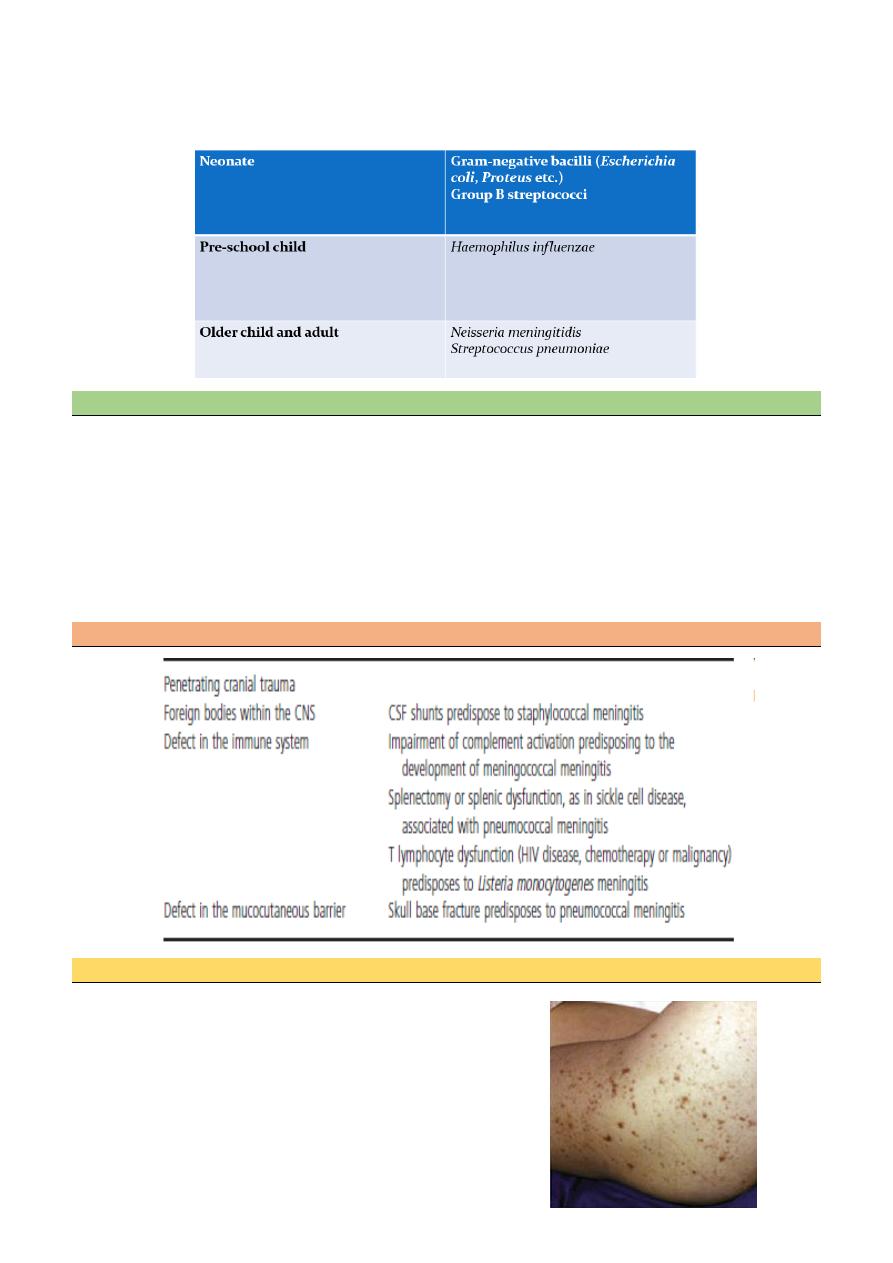
The most 3 common organisms causing meningitis in young age group are:
Strept. Pneumococci (mostly after age of 20)
Neisseria. Meningococcal
H. Influenza
Strept. pneumia are the most common nowadays, but in a certain group of patients there is a predilection to
develop pneumococcal type of meningitis especially in alcoholic ,immunocompromised ,splenectomaized
patients and those with complement deficiency.
2
Listeria monocytogens is a very important cause of meningitis in patients who are:
Pregnancy
Alcoholic
Imunocompromised
Elderly
Pathogenesis
Bacterial infection reaches the CNS either by
direct invasion
haematogenous spread
embolisation of infected thrombi.
There can also be direct extension from contiguous structures via erosion of an osteomyelitic focus.
Iatrogenic (e.g. following ventriculo-peritoneal shunt, intracranial pressure monitor or surgery).
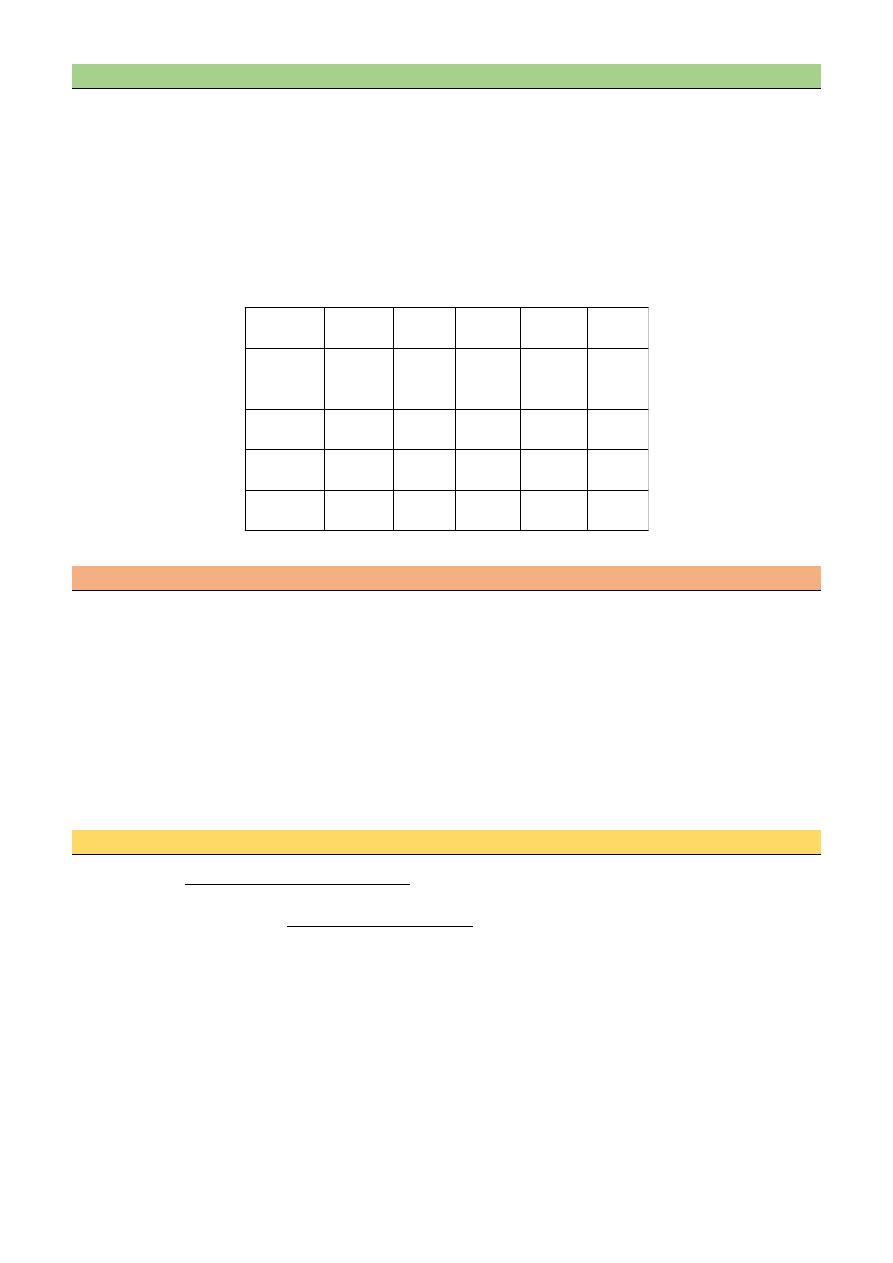
Risk factors
Clinical features
Headache, drowsiness, fever and neck stiffness are the usual
presenting features.
In severe bacterial meningitis, the patient may be comatose
and later there may be focal neurological signs.
Meningococcal meningitis is associated with a purpuric rash
in 70% of cases.
3
Diagnosis
Mortality rate is high in meningitis reaches 30 % in developed countries, so any delay in treatment will
increase the percentage of mortality
For diagnosis of meningitis, we need a high index of suspicion
CT scan is not mandatory but it is preferable in meningitis we must examine fundi to ensure there is no
raised ICP, and then we do lumbar puncture to assess the CSF.
Chemotherapy of bacterial meningitis
N-meningitides Benzyl penicillin
Strep. pneumoniae Cefotaxime
— Sensitive to B-lactams Ceftriaxone
— Resistant add Vancomycin
H. Influenza Cefotaxime
Ceftriaxone
Listeria monocytogens Ampicillin + gentamicin
Treatment of pyogenic meningitis of unknown cause.
1. Patients with a typical meningococcal rash
benzyl penicillin 2.4gIV.6-hourly
2. Adult aged 18-50 years without meningococcal rash
Cefotaxime 2 g IV.6-hourly
Ceftriaxone 2g IV.12-hourly
3. Patient in whom penicillin-resistant pneumococcal infection is suspected
Cefotaxime or ceftriaxone and add- Vancomycin I g Iv12-hourly
4. Adult aged over 50years and those in whom Listeria monocytogens suspected
As for 2 but add Ampicillin 2g IV4-hourly or Co-trimoxazole
5. Patients with a clear history of anaphylaxis to B-lactams
Chloramphenicol 25 mg/kg IV.6-hourly plus 1
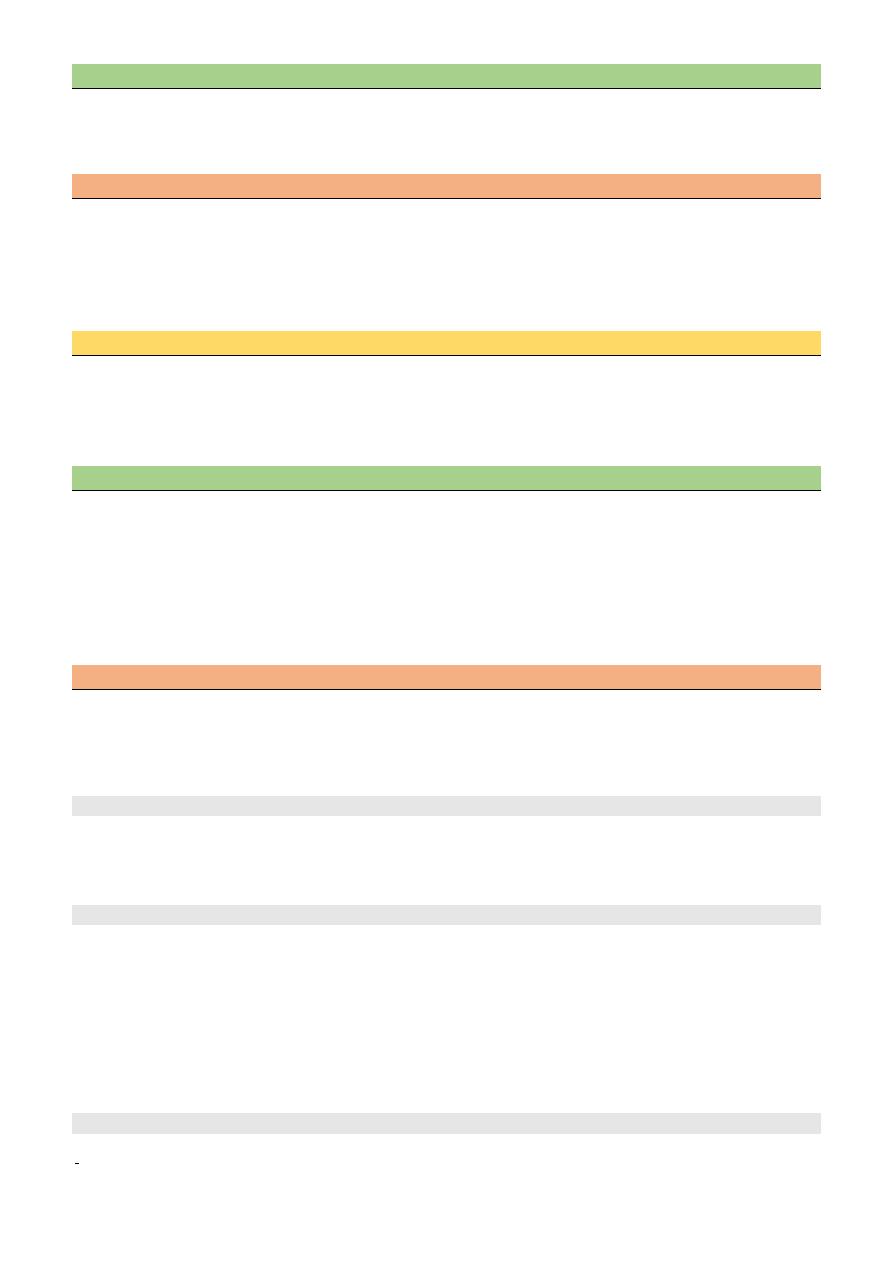
CSF INDICES IN MENINGITIS
Condition Cell
type
Cell
count
glucose protein Gm
stain
normal
lymph
0-4
60%or
more of
B.S
N
-
viral
lymph
10-
2000
N
N
-
bacterial polymor 1000-
5000
Low
Nor
increase
+
TB
L/P,M
50-
5000
Low
increase often
4
Steroid
— Steroid must be given for all patients and preferable to be given before antibiotics, four hours before
antibiotics then for 4 days only DEXAMETHASONE is preferable. Strept. Is the most organism that
benefit from steroid because it is the most to cause adhesion an hydrocephalus.
Complication of meningococcal meningitis
Rash
Shock
Renal failure
Intravascular coagulation
Pericarditis
Major intracranial complication of bacterial meningitis
Transtentorial herniation
Hydrocephalus
Infarction
Seizures
Chronic and recurrent meningitis
Characteristic neurological syndrome for>4weeks & persistent inflammation in CSF.
Causes:
Meningeal infection (TB ,FUNGAL)
Malignancy
Chemical meningitis
Tuberculos meningitis
Account of 1 % of clinical TB
Increase with HIV
Long history of fever, vomiting, anorexia, focal neurological signs, urinary retention, reduce
conscious.
Symptoms
Vomiting
Low-grade fever
Lassitude
Depression'
Confusion
Behavioral changes
Signs
Meningism (may be absent)
Ocular palsies
Cranial nerve palsies are common and often initially involve eye movements resulting from III, IV
or VI nerve palsy.
There may be facial weakness (VII), optic neuropathy (II), progressive hearing loss (VIII).
Papilledema
Depression of conscious level
Focal hemispheric signs
Diagnosis
CSF
5
1) The diagnosis is made by demonstration of AFB by ZN stain of CSF can use PCR.
2) CSF culture is the golden diagnostic tech take up to 6 weeks
3) Slightly yellow, lymphocytic, with low glucose, and high protein
Radiology
patients may show evidence of previous TB on chest X-ray
CT brain scanning is commonly abnormal
There may be hydrocephalus, parenchymal enhancement,
Evidence of cerebral infarction or cerebral edema or focal tuberculoma.
MRI is sensitive in showing meningeal enhancement, focal parenchymal abnormalities or the
development of communicating or obstructive hydrocephalus.
Mubark A. Wilkins
Treatment
:
INH 300mg 9-12 months
Rifampicin 600 mg 9-12.
Pyrazinamide 1.5_2 g 2months
Ethambutol 15mg/Kg or streptomycin 15mg/Kg 2months
Dexamethasone 6wk