Lec .3 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Hypothyroidism
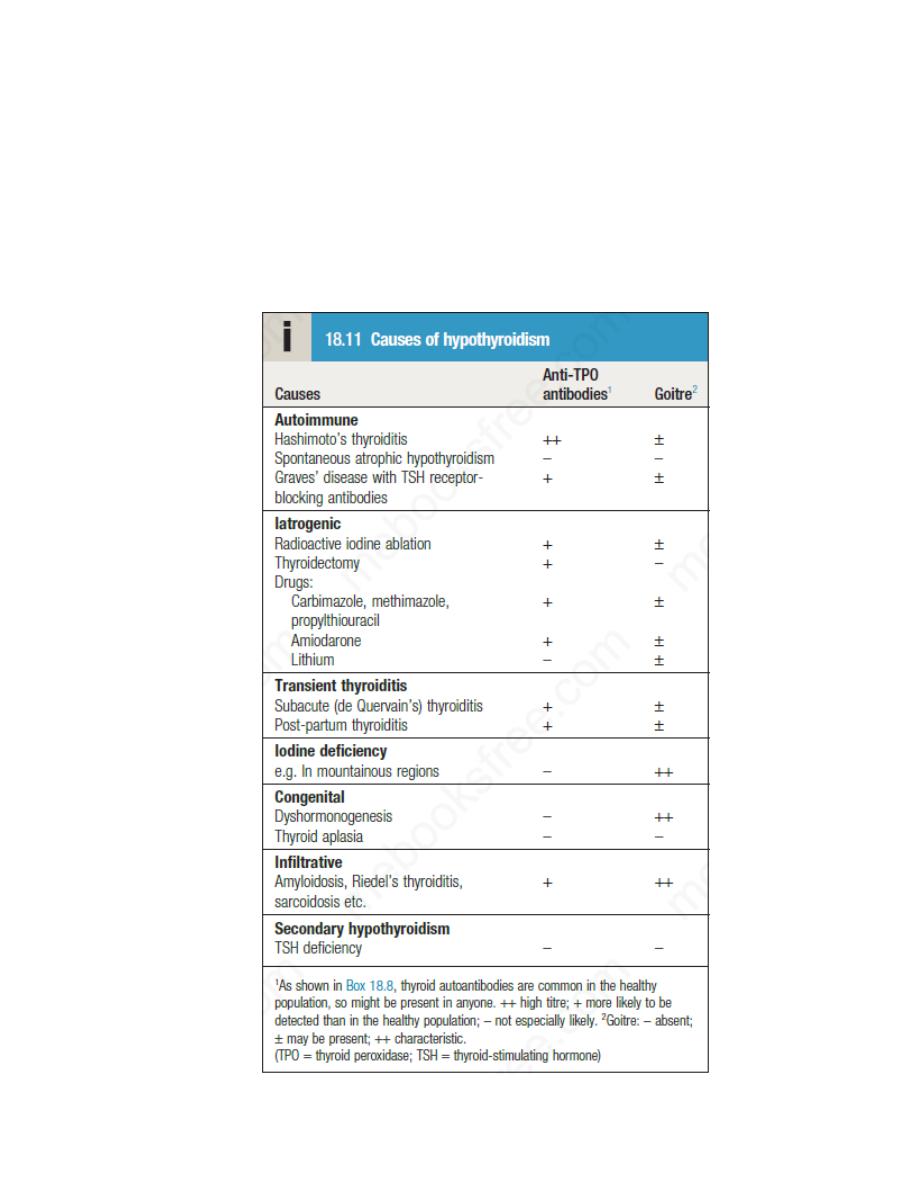
Hypothyroidism is a common condition with various causes , but
autoimmune disease (Hashimoto’s thyroiditis) and thyroid failure following
131I or surgical treatment of thyrotoxicosis account for over 90% of cases,
except in areas where iodine deficiency is endemic. Women are affected
approximately six times more frequently than men.
Lec .3 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Clinical assessment
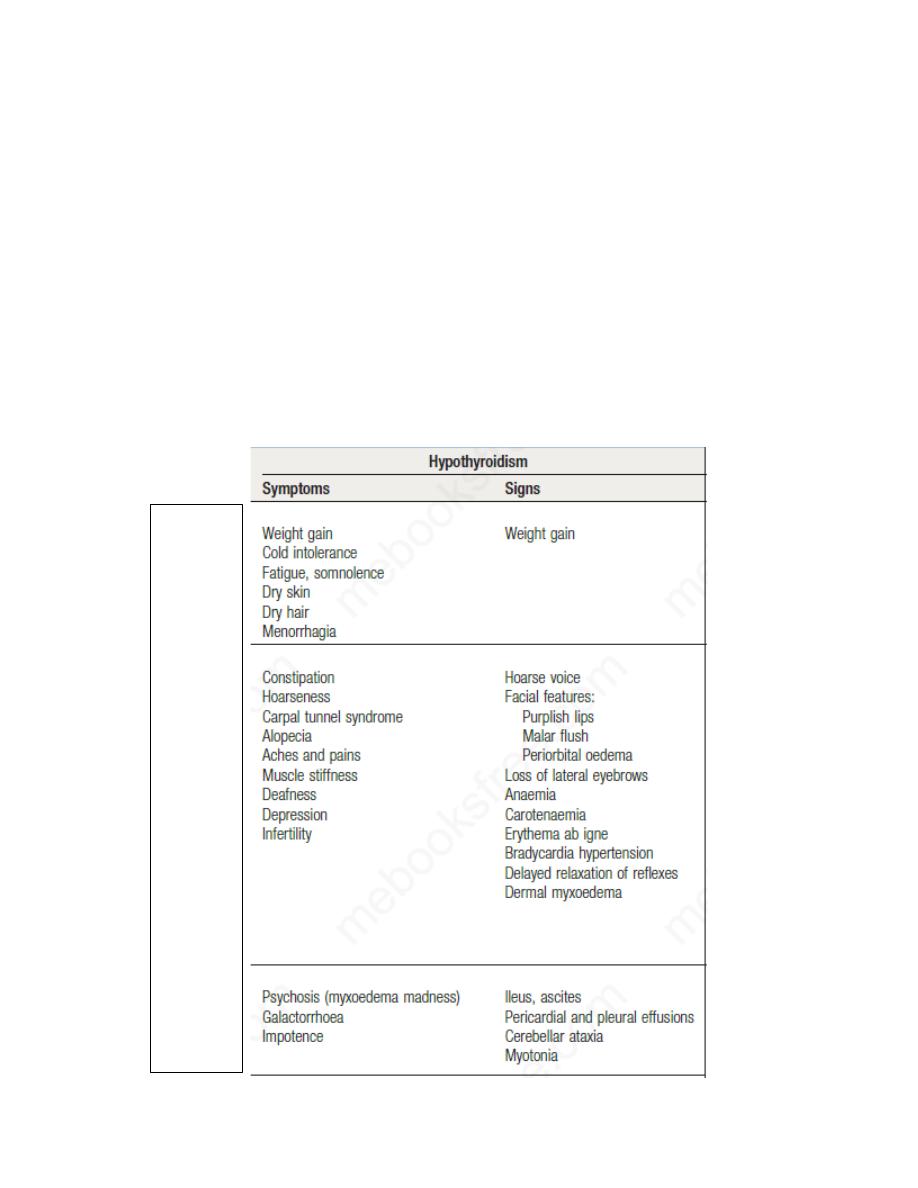
The clinical presentation depends on the duration and severity of the
hypothyroidism. Those in whom complete thyroid failure has developed
insidiously over months or years may present with many of the clinical
features listed below. A consequence of prolonged hypothyroidism is the
infiltration of many body tissues by the mucopolysaccharides hyaluronic
acid and chondroitin sulphate, resulting in a low-pitched voice, poor hearing,
slurred speech due to a large tongue, and compression of the median nerve at
the wrist (carpal tunnel syndrome). Infiltration of the dermis gives rise to
non-pitting oedema (myxoedema), which is most marked in the skin of the
hands, feet and eyelids.
Common
Less
common
Rare
Lec .3 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
The resultant periorbital puffiness is often striking and may be combined
with facial pallor due to vasoconstriction and anaemia, or a lemon-yellow
tint to the skin caused by carotenaemia, along with purplish lips and malar
flush. Most cases of hypothyroidism are not clinically obvious, however, and
a high index of suspicion needs to be maintained so that the diagnosis is not
overlooked in individuals complaining of non-specific symptoms such as
tiredness, weight gain, depression or carpal tunnel syndrome.
Care must be taken to identify patients with transient hypothyroidism, in
whom life-long levothyroxine therapy is inappropriate. This is often
observed during the first 6 months after thyroidectomy or 131I treatment of
Graves’ disease, in the post-thyrotoxic phase of subacute thyroiditis and in
post-partum thyroiditis
Investigations
In the vast majority of cases, hypothyroidism results from an intrinsic
disorder of the thyroid gland (primary hypothyroidism).
In this situation, serum T4 is low and TSH is elevated, usually in excess of
20 mIU/L. Measurements of serum T3 are unhelpful since they do not
discriminate reliably between euthyroidism and hypothyroidism. Secondary
hypothyroidism is rare and is caused by failure of TSH secretion in an
individual with hypothalamic or anterior pituitary disease. In severe,
prolonged hypothyroidism, the ECG classically demonstrates sinus
bradycardia with low voltage complexes and ST-segment and T-wave
abnormalities.
Measurement of thyroid peroxidase antibodies is helpful but further
investigations are rarely required.
Management
Treatment is with levothyroxine replacement. It is customary to start with a
low dose of 50 μg per day for 3 weeks, increasing thereafter to 100 μg per
day for a further 3 weeks and finally to a maintenance dose of 100–150 μg
per day. In younger patients, it is safe to initiate levothyroxine at a higher
dose (e.g. 100 μg per day), to allow a more rapid normalisation of thyroid

Lec .3 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
hormone levels. Levothyroxine has a half-life of 7 days so it should always
be taken as a single daily dose and at least 6 weeks should pass before
repeating thyroid function tests (as TSH takes several weeks to reach a
steady state) and adjusting the dose. Patients feel better within 2–3 weeks.
Reduction in weight and periorbital puffiness occurs quickly but the
restoration of skin and hair texture and resolution of any effusions may take
3–6 months.
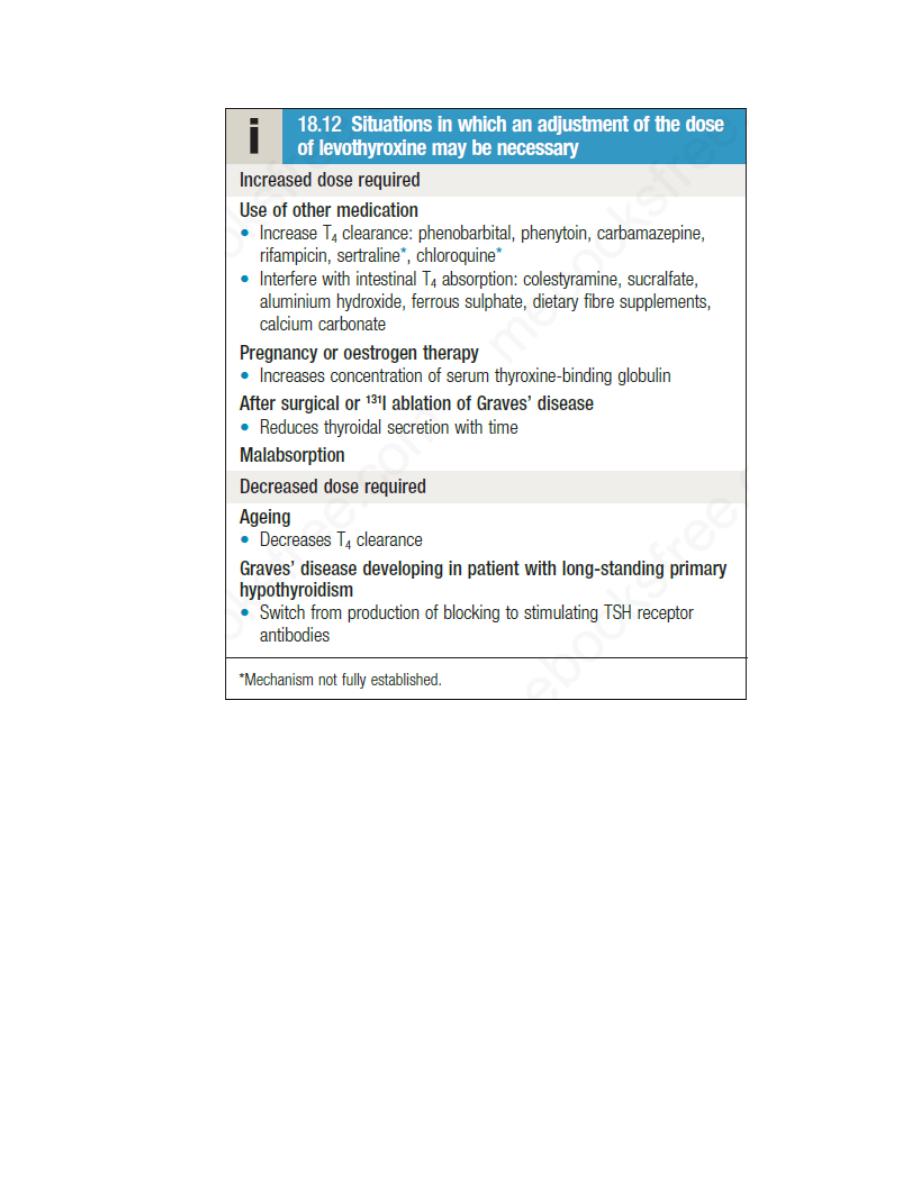
The dose of levothyroxine should be adjusted to maintain serum TSH within
the reference range. Some patients remain symptomatic despite
normalisation of TSH and may wish to take extra levothyroxine, which
suppresses TSH. However, suppressed TSH is a risk factor for osteoporosis
and atrial fibrillation , so this approach cannot be recommended.
Some patients have a persistent elevation of serum TSH despite an
ostensibly adequate replacement dose of levothyroxine; most commonly,
this is a consequence of suboptimal adherence to therapy. In some poorly
compliant patients, levothyroxine is taken diligently or even in excess for a
few days prior to a clinic visit, resulting in the seemingly anomalous
combination of a high serum T4 and high TSH.
Levothyroxine replacement in ischaemic heart disease:
Hypothyroidism and ischaemic heart disease are common conditions that
often occur together. Although angina may remain unchanged in severity or
paradoxically disappear with restoration of metabolic rate, exacerbation of
myocardial ischaemia, infarction and sudden death are recognised
complications of levothyroxine replacement, even using doses as low as 25
μg per day. In patients with known ischaemic heart disease, thyroid hormone
replacement should be introduced at low dose and increased very slowly
under specialist supervision.
Coronary intervention may be required if angina is exacerbated by
levothyroxine replacement therapy .
Lec .3 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Hypothyroidism in pregnancy
Untreated hypothyroidism is associated with subfertility and so is
uncommon in pregnancy. Subclinical hypothyroidism is more common, and
is often due to poor adherence to levothyroxine in known primary
hypothyroidism. Most pregnant women with primary hypothyroidism
require an increase in the dose of levothyroxine of approximately 25–50 μg
daily to maintain normal TSH levels because there is an increased
requirement for thyroxine during pregnancy. Furthermore, inadequately
treated maternal hypothyroidism may be associated with impaired brain
development in the fetus. Because of this, hypothyroid women
should be
monitored closely if planning a pregnancy; they should be advised to have
their thyroid function checked as soon as possible after conception and

Lec .3 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
increase their daily levothyroxine dose if necessary. During pregnancy,
serum TSH and free T4 should be measured during each trimester and the
dose of levothyroxine adjusted to maintain a normal TSH level.
Rarely, hypothyroidism may present during pregnancy with weight gain,
constipation and lethargy. The diagnosis is easily missed since these
symptoms are common in normal pregnancy. If suspected, the diagnosis can
be confirmed by checking thyroid function tests, which show a raised TSH
and low free T4.
Myxoedema coma
This is a very rare presentation of hypothyroidism in which there is a
depressed level of consciousness, usually in an elderly patient who appears
myxoedematous. Body temperature may be as low as 25°C, convulsions are
not uncommon, and cerebrospinal fluid (CSF) pressure and protein content
are raised. The mortality rate is 50% and survival depends on early
recognition an treatment of hypothyroidism and other factors contributing to
the altered consciousness level, such as medication, cardiac failure,
pneumonia, dilutional hyponatraemia and respiratory failure.
Myxoedema coma is a medical emergency and treatment must begin before
biochemical confirmation of the diagnosis. Suspected cases should be
treated with an intravenous injection of 20 μg liothyronine, followed by
further injections of 20 μg 3 times daily until there is sustained clinical
improvement. In survivors, there is a rise in body temperature within 24
hours and, after 48–72 hours, it is usually possible to switch patients to oral
levothyroxine in a dose of 50 μg daily. Unless it is apparent that the patient
has primary hypothyroidism, the thyroid failure should also be assumed to
be secondary to hypothalamic or pituitary disease and treatment given with
hydrocortisone 100 mg IM 3 times daily, pending the results of T4, TSH and
cortisol measurement . Other measures include slow rewarming cautious
use of intravenous fluids, broad-spectrum antibiotics and high-flow oxygen.

Lec .3 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Symptoms of hypothyroidism with normal thyroid function
tests:
The classic symptoms of hypothyroidism are, by their very nature, non-
specific . There is a wide differential diagnosis for symptoms such as
‘fatigue’, ‘weight gain’ and ‘low mood’. As has been noted, outside the
context of pituitary and hypothalamic disease, serum TSH is an excellent
measure of an individual’s thyroid hormone status. However, some
individuals believe that they have hypothyroidism despite normal serum
TSH concentrations. There are a large number of websites that claim that
serum TSH is not a good measure of thyroid hormone status and suggest that
other factors, such as abnormalities of T4 to T3 conversion, may lead to low
tissue levels of active thyroid hormones. Such websites often advocate a
variety of tests of thyroid function of dubious scientific validity, including
measurement of serum reverse T3, 24-hour urine T3, basal body
temperature, skin iodine absorption, and levels of selenium in blood and
urine. Individuals who believe they have hypothyroidism, despite normal
conventional tests of thyroid function, can be difficult to manage. They
require reassurance that their symptoms are being taken seriously and that
organic disease has been carefully considered; if their symptoms persist,
referral to a team specialising in medically unexplained symptoms should be
considered.