Lec .5 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Thyroid lump or swelling
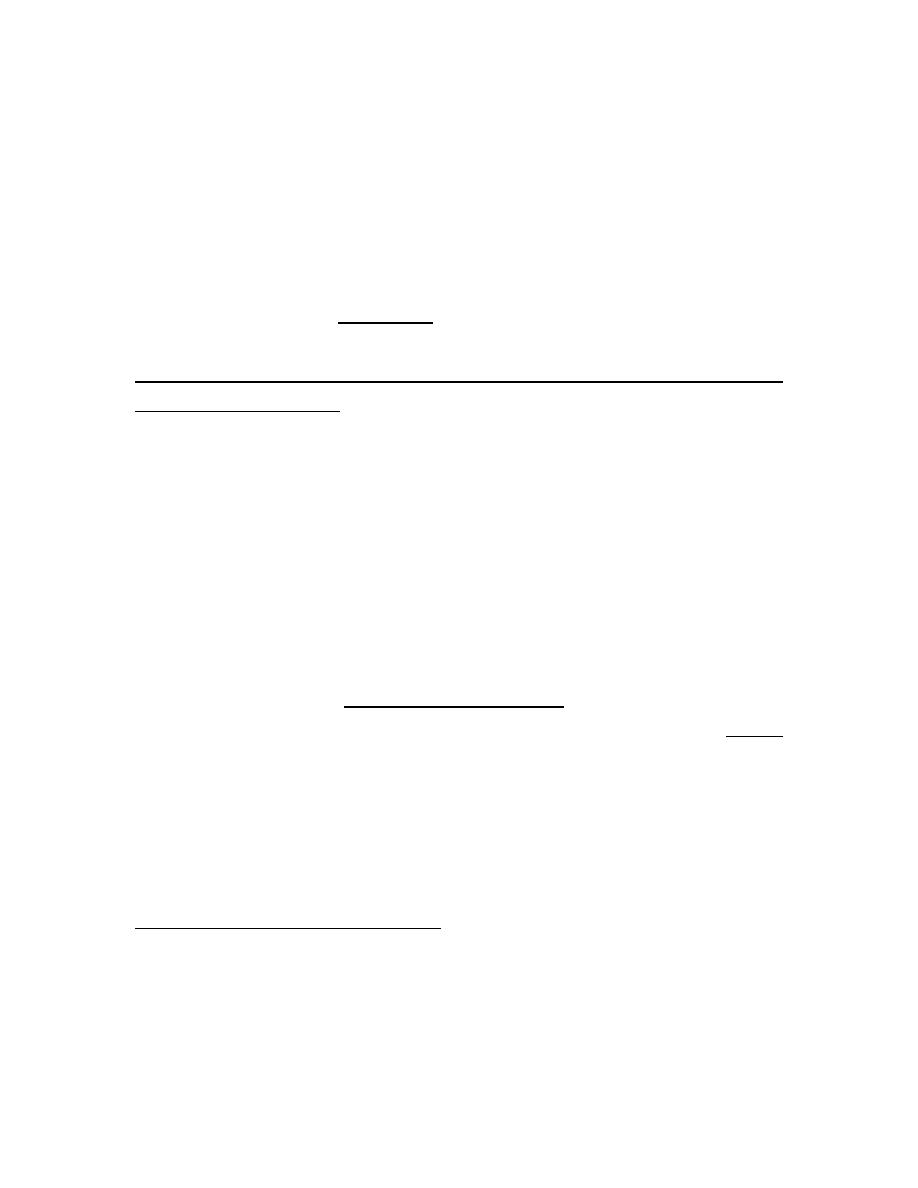
A lump or swelling in the thyroid gland can be a source of considerable
anxiety for patients. There are numerous causes but, broadly speaking, a
thyroid swelling is either a solitary nodule, a multinodular goitre or a
diffuse goitre . Nodular thyroid disease is more common in women and
occurs in approximately 30% of the adult female population. The majority
of thyroid nodules are impalpable but may be identified when imaging of
the neck is performed for another reason, such as during Doppler
ultrasonography of the carotid arteries or computed tomographic
pulmonary angiography. Increasingly, thyroid nodules are identified during
staging of patients with cancer with computed tomography (CT), magnetic
resonance imaging (MRI) or positron emission tomography (PET) scans.
Palpable thyroid nodules occur in 4–8% of adult women and 1–2% of adult
men, and classically present when the individual (or a friend or relative)
notices a lump in the neck. Multinodular goitre and solitary nodules
sometimes present with acute painful enlargement due to haemorrhage
into a nodule. Patients with thyroid nodules often worry that they have
cancer but the reality is that only 5–10% of thyroid nodules are malignant.
A nodule presenting in childhood or adolescence, particularly if there is a
past history of head and neck irradiation, or one presenting in an elderly
patient should heighten suspicion of a primary thyroid malignancy . The
presence of cervical lymphadenopathy also increases the likelihood of
malignancy.
Rarely, a secondary deposit from a renal, breast or lung carcinoma
presents as a painful, rapidly growing, solitary thyroid nodule. Thyroid
nodules identified on PET scanning have an approximately 33% chance of
being malignant.
Lec .5 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Clinical assessment and investigations
Swellings in the anterior part of the neck most commonly originate in the
thyroid and this can be confirmed by demonstrating that the swelling
moves on swallowing . It is often possible to distinguish clinically between
the three main causes of thyroid swelling. There is a broad differential
diagnosis of anterior neck swellings, which includes lymphadenopathy,
branchial cysts, dermoid cysts and thyroglossal duct cysts (the latter are
classically located in the midline and move on protrusion of the tongue).
An ultrasound scan should be performed urgently, if there is any doubt as
to the aetiology of an anterior neck swelling. Serum T3, T4 and TSH should
be measured in all patients with a goitre or solitary thyroid nodule. The
finding of biochemical thyrotoxicosis or hypothyroidism (both of which may
be subclinical) should lead to investigations, as already described in
previous lectures.
Lec .5 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Thyroid scintigraphy
Thyroid scintigraphy with 99m technetium should be performed in an
individual with a low serum TSH and a nodular thyroid to confirm the
presence of an autonomously functioning (‘
hot
’) nodule .In such
circumstances, further evaluation is not necessary. ‘
Cold
’ nodules on
scintigraphy have a much higher likelihood of malignancy, but the majority
are benign and so scintigraphy is not routinely used in the evaluation of
thyroid nodules when TSH is normal.
Toxic adenoma
A solitary toxic nodule is the cause of less than 5% of all cases of
thyrotoxicosis. The nodule is a follicular adenoma, which autonomously
secretes excess thyroid hormones and inhibits endogenous TSH secretion,
with subsequent atrophy of the rest of the thyroid gland. The adenoma is
usually greater than 3 cm in diameter.
Most patients are female and over 40 years of age. Although many nodules
are palpable, the diagnosis can be made with certainty only by thyroid
scintigraphy . The thyrotoxicosis is usually mild and in almost 50% of
patients the plasma T3 alone is elevated (T3 thyrotoxicosis). 131I (400–800
MBq (10–20 mCi)) is highly effective and is an ideal treatment since the
atrophic cells surrounding the nodule do not take up iodine and so receive
little or no radiation. For this reason, permanent hypothyroidism is unusual.
Hemithyroidectomy is an alternative management option.
Thyroid neoplasia
Patients with thyroid tumours usually present with a solitary nodule . Most
are benign and a few of these, called ‘toxic adenomas’, secrete excess
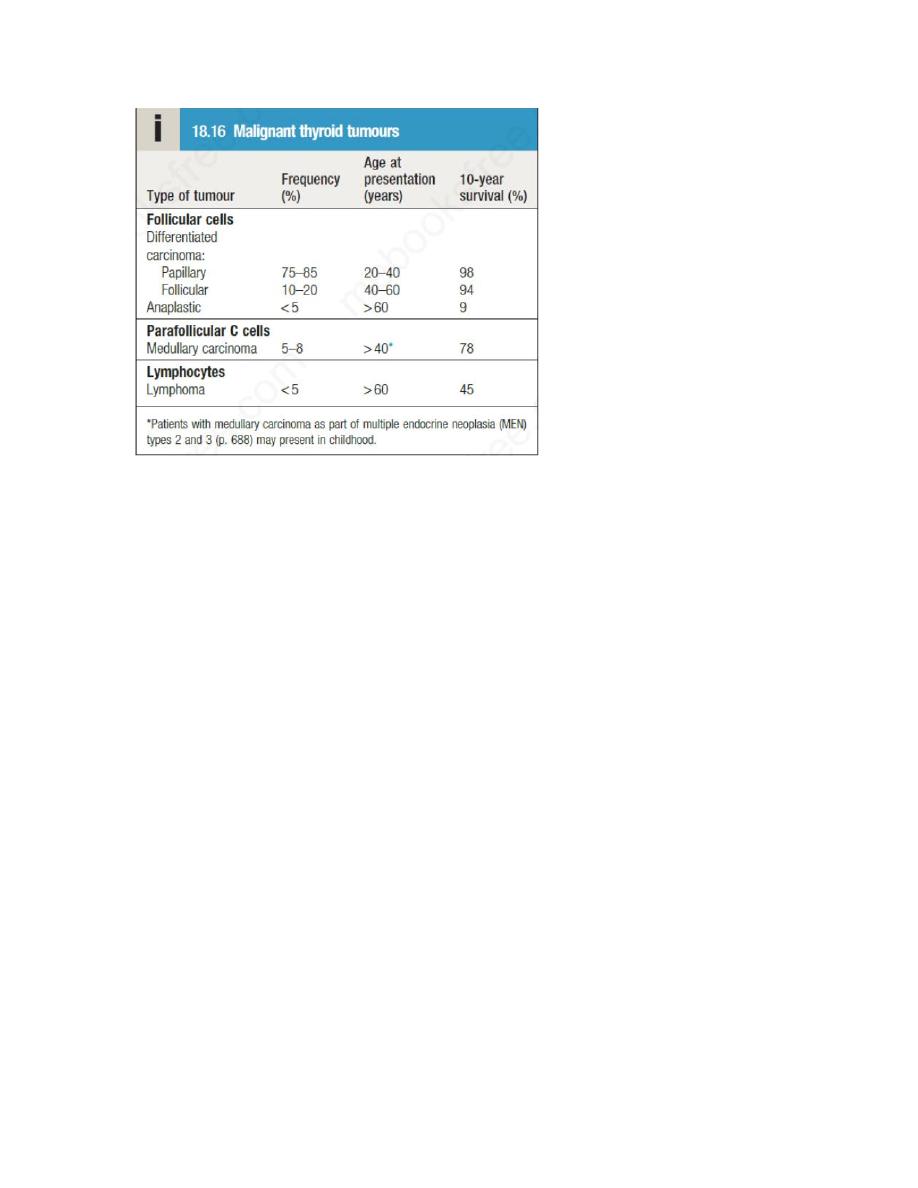
thyroid hormones. Primary thyroid malignancy is rare, accounting for less
than 1% of all carcinomas, and has an incidence of 25 per million per
annum. It can be classified according to the cell type of origin. With the
exception of medullary carcinoma, thyroid cancer is more common in
females.
Lec .5 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
Differentiated carcinoma
Papillary carcinoma
This is the most common of the malignant thyroid tumours and accounts
for 90% of radiation-induced thyroid cancer. It may be multifocal and
spread is initially to regional lymph nodes. Some patients present with
cervical lymphadenopathy and no apparent thyroid enlargement; in such
instances, the primary lesion may be less than 10 mm in diameter.
Follicular carcinoma
This is usually a single encapsulated lesion. Spread to cervical lymph nodes
is rare. Metastases are blood-borne and are most often found in bone,
lungs and brain.
Management
The management of thyroid cancers should be individualized and planned
in multidisciplinary team meetings that include all specialists involved in the
service; this should include thyroid surgeons, endocrinologists, oncologists,
pathologists, radiologists and nurse specialists. Large tumours, those with
adverse histological features and/or tumours with metastatic disease at
Lec .5 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
presentation are usually managed by total thyroidectomy followed by a
large dose of
131
I ( (approximately 30 or 100 mCi)) to ablate any remaining
normal or malignant thyroid tissue. Thereafter, long-term treatment with
levothyroxine in a dose sufficient to suppress TSH (usually 150–200 μg
daily) is given, as there is evidence that growth of differentiated thyroid
carcinomas is TSH-dependent. Smaller tumours with no adverse
histological features may require only thyroid lobectomy.
Follow-up involves measurement of serum thyroglobulin, which should be
undetectable in patients whose normal thyroid has been ablated and who
are taking a suppressive dose of levothyroxine. Thyroglobulin antibodies
may interfere with the assay and, depending on the method employed,
may result in a falsely low or high result. Detectable thyroglobulin, in the
absence of assay interference, is suggestive of tumour recurrence or
metastases, particularly if the thyroglobulin titre is rising across serial
measurements. Local recurrence or metastatic disease may be localised by
ultrasound, CT, MRI and/or whole-body scanning with
131
I, and may be
treated with further surgery and/or
131
I therapy.
Those with locally advanced or metastatic papillary and follicular carcinoma
that is refractive to
131
I may be considered for therapy with sorafenib or
lenvatinib. These drugs are multi-targeted tyrosine kinase inhibitors and
have been shown in trials to prolong progression-free survival by between
5 and 14 months.
Prognosis
Most patients with papillary and follicular thyroid cancer will be cured with
appropriate treatment. Adverse prognostic factors include older age at
presentation, the presence of distant metastases, male sex and certain
histological subtypes.
Anaplastic carcinoma and lymphoma
These two conditions are difficult to distinguish clinically but are distinct
cytologically and histologically. Patients are usually over 60 years of age and

Lec .5 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
present with rapid thyroid enlargement over 2–3 months. The goitre is hard
and there may be stridor due to tracheal compression and hoarseness due
to recurrent laryngeal nerve palsy. There is no effective treatment for
anaplastic carcinoma, although surgery and radiotherapy may be
considered in some circumstances. In older patients, median survival is
only 7 months.
The prognosis for lymphoma, which may arise from preexisting
Hashimoto’s thyroiditis, is better , with a median survival of 9 years. Some
98% of tumours are non-Hodgkin’s lymphomas, usually the diffuse large B-
cell subtype. Treatment is with combination chemotherapy and external
beam radiotherapy .
Medullary carcinoma
This tumour arises from the parafollicular C cells of the thyroid. In addition
to calcitonin, the tumour may secrete 5-hydroxytryptamine (5-HT,
serotonin), various peptides of the tachykinin family, adrenocorticotrophic
hormone (ACTH) and prostaglandins. As a consequence, carcinoid
syndrome and Cushing’s syndrome may occur.
Patients usually present in middle age with a firm thyroid mass. Cervical
lymph node involvement is common but distant metastases are rare
initially. Serum calcitonin levels are raised and are useful in monitoring
response to treatment.
Treatment
is by total thyroidectomy with removal of regional cervical
lymph nodes. Since the C cells do not concentrate iodine and are not
responsive to TSH, there is no role for 131I therapy or TSH suppression with
levothyroxine. External beam radiotherapy may be considered in some
patients at high risk of local recurrence. Vandetanib and cabozantinib are
tyrosine kinase inhibitors licensed for patients with progressive advanced
medullary cancer. The prognosis is less good than for papillary and
follicular. Medullary carcinoma of the thyroid occurs sporadically in 70–90%
cases; in 10–30% of cases, there is a genetic predisposition that is inherited

Lec .5 Dr. Nihad Abdallah Al-jeboori /Subspecialty Endocrinology &Diabetes
in an autosomal dominant fashion and is due to an activating mutation in
the RET gene. This inherited tendency normally forms part of one of the
MEN syndromes (MEN 2 (also known as MEN 2a) or MEN 3 (also known as
MEN 2b), but, occasionally, susceptibility to medullary carcinoma is the only
inherited trait (familial medullary thyroid cancer).
Riedel’s thyroiditis
This is not a form of thyroid cancer but the presentation is similar and the
differentiation can usually be made only by thyroid biopsy. It is an
exceptionally rare condition of unknown aetiology, in which thereis
extensive infiltration of the thyroid and surrounding structures with fibrous
tissue. There may be associated mediastinal and retroperitoneal fibrosis.
Presentation is with a slow-growing goitre that is irregular and stony-hard.
There is usually tracheal and oesophageal compression necessitating partial
thyroidectomy. Other recognised complications include recurrent laryngeal
nerve palsy, hypoparathyroidism and eventually hypothyroidism.