Assessment of
fetal wellbeing
during labor

Assessment is very
important because labor is
very stressful to the fetus
and intrauterine asphyxia is
a major cause of morbidity
and mortality.

One of the best
methods available for
detection of fetal
wellbeing is the FHR
because the FHR
change with condition
of the fetus.
explanation:
Intrauterine asphyxia or hypoxia produce
changes in the blood of the fetus this will
sensitize the chemoreceptor and
baroreceptor either sympathetic over
stimulation tachycardia or vagal
stimulation bradycardia.
** at first asphyxia sympathetic over
stimulation tachycardia late
asphyxia co2 accumulation and shift
from aerobic to anaerobic metabolism
accumulation of lactic acid lowering of
PH vagal stimulation bradycardia.

But FHR is regarded indirect evidence.
So it is screening test and not
diagnostic.
Even in the most serious of these
signs, bradycardia with passage of
meconium is found to be associated
with a significant fetal hypoxia in only
25%. In order to be sure we have to
take a scalp blood sample inutero for
acid, PH, PCO2 this show only 35% of
these fetuses with FHR abnormalities
are really affected.

*
Methods of assessing FHR:
1- inspection of amniotic fluid for
meconium
2- intermittent auscultation.
3- continuous external by CTG
4- Continuous electronic fetal
monitoring by internal fetal
electrode
5- fetal scalp PH

In the 1st method we auscultate every
¼ to ½ hour by pinard stethoscope
give us a clue only if the fetus is
viable and not to assess fetal wellbeing
(external method).
There is internal method which gives
more satisfactory and accurate results
but is invasive (electrode inserted in
the fetal scalp) here the fetal ECG is
recorded and can detect changes in
the pattern of FHR.
Etiology of fetal compromise during
labor could be due to maternal, fetal,
umbilical, placental, and uterine
factors:
1- Maternal: maternal hyper or
hypotension, severe anemia, heart
diseases, epilepsy, pulmonary
diseases, (asthma, COLD)
HYPOXIA.
2- Fetal factors: such as fetal anemia
(in case of Rh-isoimmunization),
infections, twin to twin transfusion.
3- Uterine factors: titanic uterine
contractions, or excessive or misuse
of oxytocic drugs.
4- Umbilical cord problems:
One artery, vasa brevia artery, short
cord, haematoma in the cord, cord
prolapse.
5- Placental factors:
Infarction, abruption, post mature
placenta (placental aging)
Monitoring the fetus during labor
There is probably little value in
continuous EFM (electronic fetal
monitoring) in low-risk pregnancies.
Such women may have a short (20
minutes) CTG recording on
admission to the labor ward. If the
CTG is normal thereafter the fetal
heart is listened to every 15 - 30
minutes with a Pinard stethoscope
/or sonicaid.

features of a normal FHR pattern include :
a baseline heart rate of between 110 and 160 bpm
(averaged over a 20 minute interval or more),
variability of between 5 and 25 bpm (variation in the FHR
above and below the baseline),
accelerations (a transient increase in FHR of at least 15 bpm
lasting at least 15 seconds)
and the absence of decelerations (transient decrease in the
FHR of 15 bpm or more).
Women who begin labour with intermittent auscultation
will be advised to change to continuous EFM if any
complications occur during labour.

The FHR should be auscultated with a Pinard stethoscope, or
by using a handheld
Doppler device, early on in the initial assessment.
It should be listened to for at least 1 minute immediately after
a contraction.
This should be repeated every 15 minutes during the first
stage of labour and at least every 5 minutes in the second
stage.
The practice of performing an ‘admission CTG’ on all women
is no longer recommended; however, a CTG should be
performed if there are issues
that might complicate labour and delivery.
Most of these women will also be advised to have continuous
EFM throughout labour, using the CTG.

There is a high risk of hypoxia in the
following circumstances so
continuous EFM is required:
See the notes of this slide

Risk factors for fetal compromise in labour
Placental insufficiency – FGR and pre-eclampsia.
Prematurity.
Postmaturity.
Multiple pregnancy.
Prolonged labour.
Augmentation with oxytocin/hyperstimulation.
Precipitate labour.
Intrapartum abruption.
Cord prolapse.
Uterine rupture/dehiscence.
Maternal diabetes.
Cholestasis of pregnancy.
Maternal pyrexia/chorioamnionitis.
Oligohydramnios.
Continuous electronic fetal heart
rate monitoring ( CEFM)
This is performed with either:
1) An external fetal heart rate
monitor with Doppler ultrasound
2) An electrode attached to the
fetal scalp showing the fetal heart
rate derived from the fetal ECG.

Either of these provides the fetal
heart rate and this is recorded on a
continuous trace. In normal labor,
this should be between 110 and
160 beats/minute EFM is used as a
screening test to detect those
babies who are developing
metabolic acidosis. The diagnostic
test is to perform a fetal scalp
sample and measure the scalp pH.
Changes in the fetal heart
rate may be classified into
three groups.
*1)Speed of heart rate changes
*2)Baseline variability changes
*3) Intermittent variations changes
*1)Speed of heart rate: either tachy or
bradycaria
1) fetal tachycardia. The causes of this
might be:
• A maternal tachycardia due to
pyrexia, pain, fear or dehydration.
• Fetal hypoxia.
Management is to exclude or correct a
maternal cause and, if the tachycardia
persists, a fetal blood sample should
be performed.
2) baseline fetal bradycardia: is
uncommon
*2)Baseline variability
The variation in fetal heart rate
from one beat to the next
(baseline variability) is due to
the balance between the
parasympathetic and the
sympathetic nervous system.
In normal labor this varies by
10–25 beats
Abnormality of baseline variability are:
Either loss of variability or increased
variability:
1) Loss of baseline variability may be
caused by:
• Administration of drugs to the mother
including pethidine, diazepam and many
anti-hypertensive agents, especially b-
blockers.
• Fetal sleep especially in early labor.
• Fetal hypoxia.

2) Increased baseline
variability
This is usually is of serious
significance. May be due to:
• Fetal asphyxia.
*3) Intermittent variations
1) Accelerations: are in
intermittent periods in which the
fetal heart rate is raised quite
markedly above the baseline. They
are a sign of fetal health.
Increase by 15 beats for 15
seconds
2) Decelerations:
Decelerations are
intermittent changes in the
baseline and fall into three
categories:
a- Early decelerations:
b-
Late decelerations.
(serious)
c- Variable decelerations.

a- Early decelerations:
These are due to vagal
stimulation following head
compression as the fetus
descends the birth canal
usually occur in the late 1st
stage and 2nd stage of labor.
They usually have no
significance
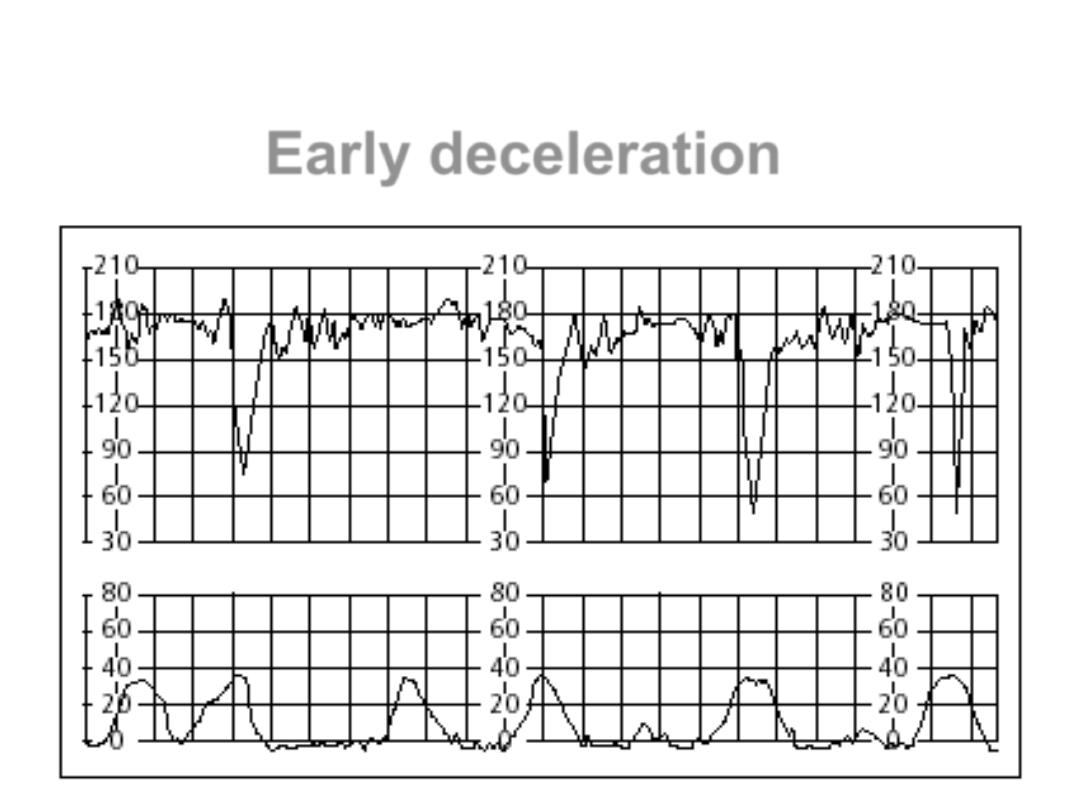
Early deceleration

b- Late decelerations.
They differ from early
decelerations in that they are U-
shaped, start more than 30
seconds after the contraction
has started and continue after
the contraction has finished.
They are thought to be
metabolic in nature and always
warrant a fetal blood sample.

Look for any reversible causes (e.g. dehydration, mother lying
flat) and if it persists, further assessment of the fetus is
necessary with FBS. If this is not possible or safe, then the
baby should be delivered without delay.
the CTG sometimes is difficult to interpret and has high false-
positive rate (i.e. it often raises the possibility of fetal
compromise when in fact the fetus is still in good condition).
In order that the use of the CTG does not lead to
unnecessary intervention, FBS may be performed during
labour to measure fetal pH and base excess directly
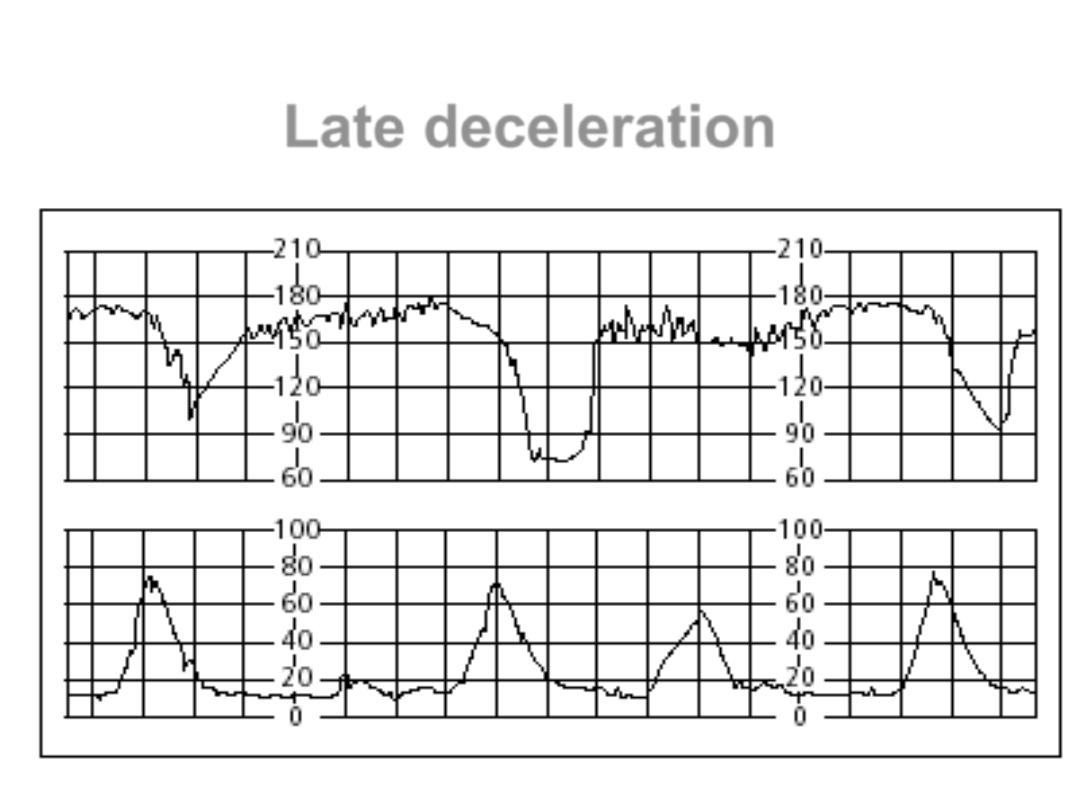
Late deceleration

Management of possible fetal compromise:
A number of resuscitative maneuvers should be considered
when a CTG is
classified as ‘suspicious’.
These include 1- repositioning of the mother, 2- intravenous
fluids, 3- reducing or stopping the oxytocin infusion 4- and
correction of epidural associated hypotension. It is reasonable
to continue observation of the CTG and
more complex intervention is not required.
If a CTG becomes ‘pathological’,these reversible factors
should also be considered, but it is also important to carry out
an immediate vaginal examination to exclude malpresentation
and cord prolapse and to assess the progress of the labour.
If the cervix is fully dilated, it may be possible to deliver the
baby vaginally using the forceps or ventouse.

Alternatively, if the cervix is not fully dilated, a fetal blood sampling
FBS can be
considered. This is usually only possible when the cervix is dilated 3
cm or more.
A normal result will permit labour to continue, although it may need
to be
repeated every 30–60 minutes if the CTG abnormalities persist or
worsen.
An abnormal result mandates immediate delivery by caesarean
section if the cervix is not fully dilated.
Fresh, thick meconium in the presence of a reassuring CTG is still a
cause for
concern, and although the labour may be allowed to continue, the
threshold for
intervention will be lowered and a paediatrician should be present at
delivery.

c- Variable decelerations.
Recurrent variable decelerations: the
important features to note are that the
decelerations vary both in shape and in
their relationship to the uterine
contraction. The most common cause of
these is cord compression. Either the
cord is compressed between the
presenting part and the pelvic side walls
or the cord is around the fetal neck or a
limb. Usually they do not indicate a fetal
blood sample but, if associated with
meconium or a change in the baseline
heart rate, one should be performed.
Passage of meconium
Stimulation of the vagus inutero causes
the fetal gut to contract and the anal
sphincter to relax so that meconium (fetal
stool) is passed into the amniotic fluid.
Meconium is made up of swallowed cells in
late pregnancy and alimentary tract cells,
all of which are stained with bile.
With a normal fetal heart rate trace, the
fetus is unlikely to be hypoxic, but if the
fetal heart rate trace is abnormal when
meconium is passed, then a fetal blood
sample (FBS) should be performed.
FBS
fetal blood sampling
The pH results are interpreted
as follows:
• PH >7.25: normal.
• PH 7.20–7.25: pre-asphyxia.
• PH <7.20: asphyxia.

Fetal blood sampling procedure
Explanation is given and consent obtained from the woman.
She is asked to lie in the left lateral position. An amnioscope
is inserted into the vagina and its distal end is applied to the
fetal head. The scalp is cleaned and a small cut is made using a
blade with a guard. The resulting blood is collected into a
microtube. The amount of blood required is approximately
0.25 ml. A normal pH value is above 7.25. A pH below 7.20 is
confirmation of fetal compromise. Values between 7.20 and
7.25 are ‘borderline’.

The base deficit can also be useful in interpretation of the
fetal scalp pH. A base excess of more than −12.0 mmol/l
demonstrates a significant metabolic acidosis, with increasing
risk of fetal neurological injury beyond this level. More than
one fetal scalp sample may be necessary over the course of
the labour. A downward trend in the fetal scalp pH values is
to be expected and should be assessed together with how
the labour is progressing.
If an abnormal CTG persists in labour, then, despite normal
values, fetal scalp sampling should be repeated every 60
minutes, or sooner if the CTG deteriorates.
If the result is borderline, it should be repeated no more than
30 minutes later.